12 October 2022: Articles 
Effectiveness of Prolotherapy Combined with Physical Therapy Versus Physical Therapy Only for Frozen Shoulder: A Case Report
Unknown etiology, Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents, Rare coexistence of disease or pathology
Nuralam Sam1ABCDEF*, Irawan Yusuf1ABCDEF, Irfan Idris2ABCDEF, Endy Adnan3ABCDEF, Ratna Darjanti Haryadi4ABCDEF, Firdaus Hamid5ABCDEF, Muhammad Andry Usman6ABCDEF, Muhammad Phetrus JohanDOI: 10.12659/AJCR.936995
Am J Case Rep 2022; 23:e936995






Abstract
BACKGROUND: Frozen shoulder (FS) is a common conditions that causes significant morbidity. It is characterized by restriction of both active and passive shoulder motion (ROM) of the glenohumeral joint. The etiology, pathology, and most efficacious treatments are unclear. The purpose of FS treatment is complete elimination of pain and recovery of shoulder joint function. Prolotherapy injects certain compounds into articular spaces, ligaments, and/or tendons to relieve pain and disability around joint spaces and to stimulate a proliferation cascade to enhance tissue repair and strength. This case report aims to describe functional outcome changes in 2 patients with FS, comparing prolotherapy combined with physical therapy vs physical therapy only.
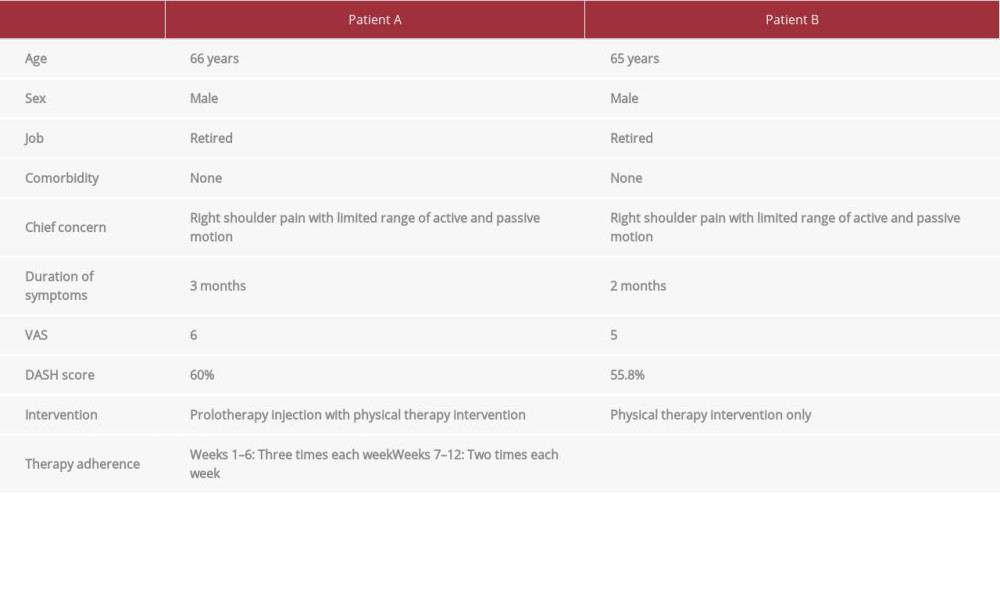
CASE REPORT: We report the cases of 2 patients with confirmed FS. Patient A was 66-year-old man with chief concern of right shoulder pain and limited ROM in the past 3 months, which disrupted daily life, with a visual analog scale (VAS) of 6 out of 10. Patient B was 65-year-old man with chief concern of right shoulder pain and limited ROM in the past 2 months. The symptoms affected his general quality of life, with a VAS of 5 out of 10. Patient A underwent prolotherapy combined with physical therapy and had significantly improved ROM after 2 weeks, with relieved pain and improved shoulder function. Patient B underwent physical therapy only and showed similar ROM and no significant pain improvement.
CONCLUSIONS: Initial treatment with prolotherapy combined with physical therapy for patients with frozen shoulder achieved fast improvement of active and passive ROM, significantly decreased pain, and improved quality of life compared to physical therapy intervention only.
Keywords: Bursitis, Prolotherapy, Physical Therapy Modalities, functional status, Aged, Humans, Male, Quality of Life, Range of Motion, Articular, shoulder pain, Treatment Outcome
Background
Frozen shoulder (FS) is a common conditions that causes significant morbidity and is characterized by restriction of active and passive motion of the glenohumeral joint. The etiology, pathology, and most efficacious treatments are unclear. The lifetime prevalence of frozen shoulder is estimated to be 2–5% of the general population and it occurs more commonly in women [1,2].
The purpose of treatment of FS is complete recovery of joint function and elimination of pain [3]. FS has been regarded as self-limiting, but in a prospective study, 50% of patients were still experiencing pain or stiffness of the shoulder at a mean of 7 years from onset of the condition [4].
Due to the increasing prevalence and morbidity, current management of FS includes non-operative and operative interventions. Conservative treatment of FS is successful in up to 90% of patients [5]. Prolotherapy is an injection-based complementary therapy that uses 15% dextrose in a 10-ml disposable syringe filled with 3.75 ml 40%, 1 ml lidocaine, and 5.25 ml aquadest, which affects the articular spaces, ligaments, and/or tendons, and treats the causes of pain and disability around joint spaces [6,7]. Injection of solutions that include dextrose can cause local inflammation that stimulates a proliferation cascade in which various cells, including fibroblasts, endothelial cells, and myofibroblasts, enhance tissue repair and strength. The final phase of healing is tissue remodeling, which decreases pain, improves joint stability, biomechanics, and function, and also increased active and passive shoulder motion [7–10].
Here, we report 2 cases with the different interventions of patients with FS diagnosed. This case report aims to describe the functional outcomes of 2 patients – 1 treated with prolo-therapy combined with physical therapy and the other only receiving physical therapy – using the Disability of the Arm, Shoulder, and Hand (DASH) score, to maintain and improve the quality of life (return with no limited range of motion) and to reduce morbidity.
Case Reports
PATIENT A:
A 66-year-old man came to the rehabilitation clinic with a chief concern of right shoulder pain and limited range of active and passive motion starting 3 months ago. He reported not being able to move his right arm and having a hard time doing activities of daily life such as dressing and washing. The pain in the shoulder was felt radiating into the neck and elbows. He was awakened at night due to pain. His pain was measured based on the Visual Analog Scale (VAS), which was 6 out of 10 in daily activities. He had is no comorbidities.
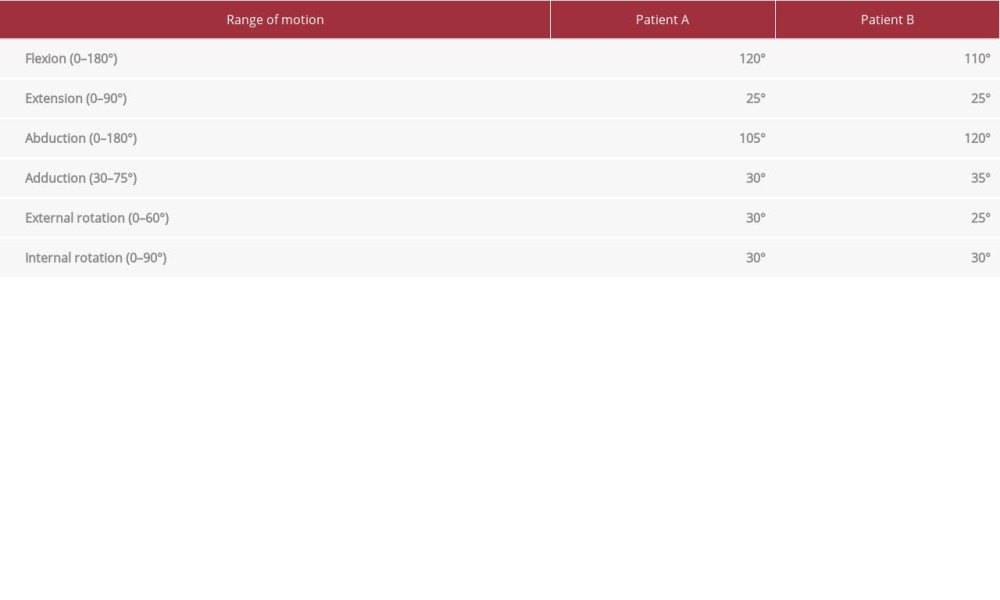
On examination, his right glenohumeral joint active ranges of motion (ROM) were: flexion 130 degrees, extension 25 degrees, abduction 135 degrees, adduction 30 degrees, external rotation 30 degrees, and internal rotation 30 degrees. The resisted right glenohumeral joint with each range of motion was graded 3/5. Anterior, posterior, and posteroinferior joint play of the right glenohumeral joint was restricted and painful. His right rotator cuff muscle (supraspinatus, infraspinatus, teres minor, and subscapularis) were tender upon palpation.
The diagnosis of the frozen shoulder was determined following anamnesis, physical therapy examination, and evaluation.
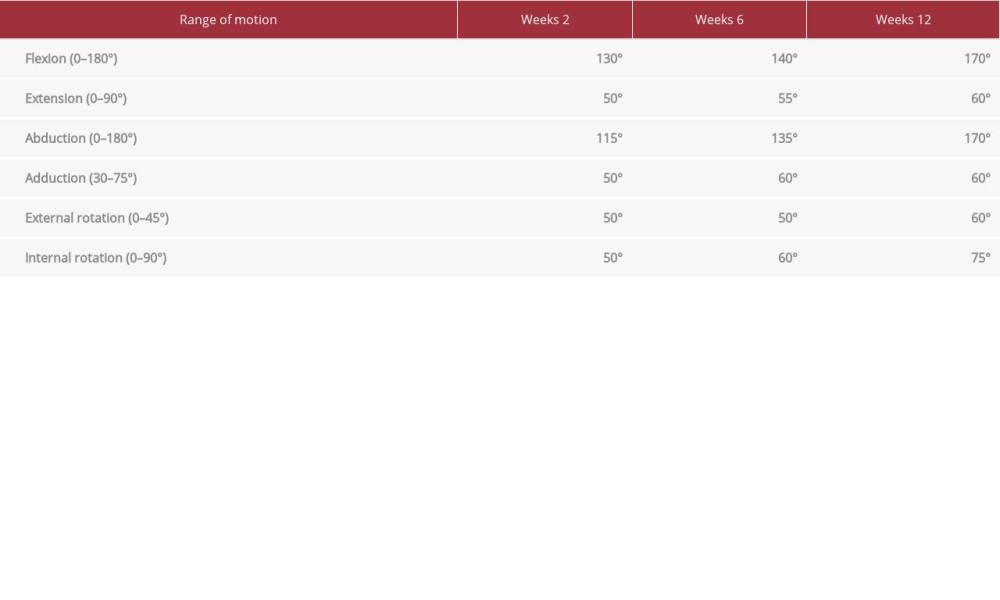
Treatment for the patient consisted of injection of prolotherapy, which contained dextrose 15% with disposable syringe 10 ml with 3.75 ml 40%, 1 ml lidocaine, and 5.25% ml sterile water. The injection points on the rotator cuff included the supraspinatus, infraspinatus, teres minor, subscapularis, and intraarticular glenohumeral joint, subacromial bursa, long head tendon of the biceps, and acromioclavicular joint [19]. Injections are administered 4 times with an interval of 2 weeks between each injection. The treatment combined with intervention therapy consisted of shoulder-strengthening exercise, gentle stretching, and ultrasound diathermy of the shoulder region. Interventions included a home exercise program, instruction in shoulder compress heat/ice use, ROM, and muscle stretching.
The patient was scheduled for therapy 3 times a week, in these patients during the first to sixth weeks had complete and regular therapy. At weeks 7 and 12, he missed 1 therapy session each.
At the 12- week visit, the active ROM right glenohumeral were: flexion 170 degrees, extension 60 degrees, abduction 170 degrees, adduction 60 degrees, external rotation 60 degrees, and internal rotation 75 degrees, showing more improvements in ROM. After 12 weeks of injection prolotherapy combined with physical therapy, he had further relief of pain and improved function based on the improved DASH score.
PATIENT B:
The patient was a 65-year-old man came to the rehabilitation clinic with a chief concern of right shoulder pain and limited range of active and passive motion starting 2 months ago. These problems started gradually but over time the symptoms began to affect his general quality of life. His pain got worse at night and disrupted his sleep. The patient reported difficulty working and dressing. Pain measured based on the VAS was 5 out of 10 in daily activities. He had no comorbidities.
During examination, his right glenohumeral joint active ranges of motion (ROM) were: flexion 110 degrees, extension 25 degrees, abduction 120 degrees, adduction 35 degrees, external rotation 25 degrees, and internal rotation 30 degrees. The resisted right glenohumeral joint with each range of motion were graded 3/5. His right rotator cuff muscles (supraspinatus, infra-spinatus, teres minor and subscapularis) were tender upon palpation. The diagnosis of frozen shoulder was determined following anamnesis, physical therapy examination, and evaluation.
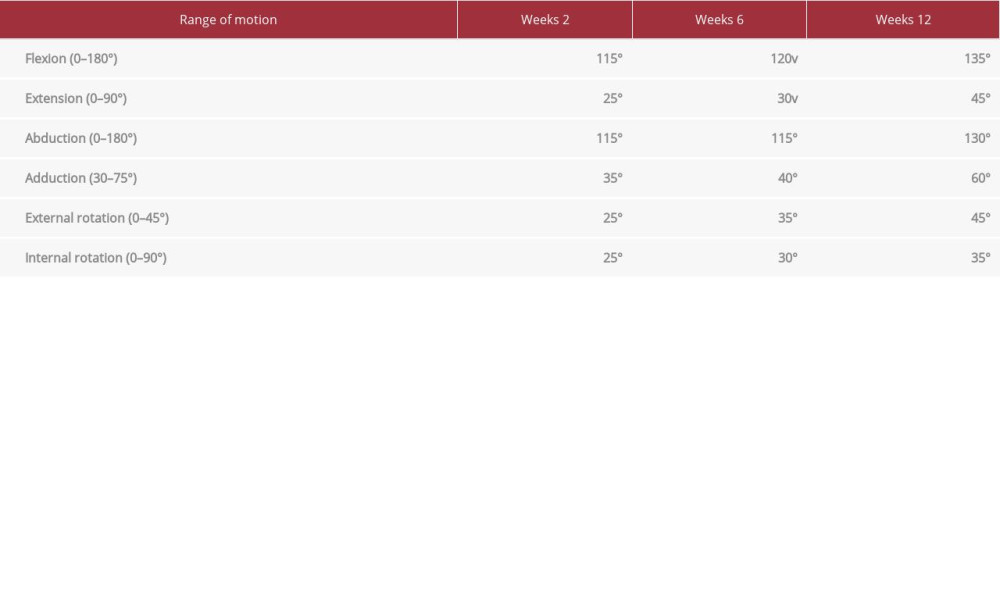
Initial treatment with physical therapy intervention consisted of shoulder-strengthening exercise, gentle stretching, and ultrasound diathermy of shoulder region. Interventions included a home exercise program, and instruction on shoulder compress heat/ice use, ROM, and muscle stretching.
The patient was scheduled for therapy 3 times a week during weeks 1–12 for complete and regularly therapy.
At the 12-week visit, the active ROM right glenohumeral were: flexion 135 degrees, extension 45 degrees, abduction 130 degrees, adduction 60 degrees, external rotation 45 degrees, and internal rotation 35 degrees, showing improvements of ROM. After 12 weeks of physical therapy, he had decreased pain and improved function based on the improved DASH score (Tables 1–4).
Discussion
As shown in Table 1, both of these patients had a frozen shoulder diagnosis. Reeves [11] identified 3 phases in the natural history of the frozen shoulder: (1) an early painful phase lasting 10–36 weeks; (2) an intermediate, stiff or frozen phase characterized mainly by a limited range of motion lasting 4–12 months; and (3) a recovery or thawing phase lasting 5–24 months or more. Both of these patients were in the first phase when they initially visited the clinic.
Hai le et al [5] found that clinical FS patients usually first present with shoulder pain followed by gradual loss of active and passive range of motion (ROM) due to fibrosis of the glenohumeral joint capsule. Boyle-Walker et al [12] observed that the majority of patients (90.6%) reported developing shoulder pain before loss of motion. These previous case reports are similar to our clinical findings from our patients. They also emphasize the problem of shoulder pain with limited active and passive ROM.
By presenting a chronic course, pain, and unwieldy treatment, this condition affects shoulder function for daily living activities, compromising the quality of life (QoL) of patients, such as writing, washing their back, wearing clothes, and also difficulty sleeping due to pain. The Disability of the Arm, Shoulder, and Hand Questionnaire (DASH) is a self-administered regional questionnaire consisting of 30 specific questions used to evaluate functional capacity of the affected arm. It has a score that ranges from zero to 100, and the higher the score, the greater the functional disability. DASH has been recommended for use in evaluation of patients with shoulder disabilities [13]. Although Patient A had a higher DASH score than Patient B, both patients were classified as having a severe quality of life disruption. Outcomes from Patient A were much better than Patient B, which might be the result of combined prolotherapy and physical therapy intervention.
Prolotherapy has been used in clinical practice to treat various chronic musculoskeletal conditions, such as ligamentous laxity, arthritic conditions, osteoarthritis, and tendinosis. Prolotherapy is prepared with hypertonic dextrose in distinct concentrations that introduce small amounts of an irritant solution to the site of pain and cause the osmotic rupture of local cells. Increased glucose in the extracellular matrix stimulates local tissue irritation, which produces acute inflammatory response and improves fibroblast proliferation and subsequent collagen synthesis, which are key factors for healing and tissue renewal. Dextrose prolotherapy can reduce pain and improve shoulder function and patient satisfaction, which improves patient quality of life [14]. The aim of this case report was to present the results of prolotherapy for treatment of frozen shoulder. Seven et al used prolotherapy in treatment of chronic rotator cuff lesions in 101 patients (44 controls and 57 in the prolo-therapy group); the prolotherapy group achieved a significant improvement in VAS, quality of life, and shoulder range of motion at 3 weeks of treatment when compared to pre-injection values and this significant improvement continued after the repeated injections (
Conclusions
Initial treatment with prolotherapy combined with physical therapy in a patient with frozen shoulder showed benefits, including fast improvement of active and passive ROM, significantly decreases pain, and improved quality of life compared to physical therapy intervention only. Prolotherapy can provide effective management of a patient with a frozen shoulder and its effects are sustained until full recovery. Physical therapy is sufficient for regaining the previous range of motion.
References:
1.. Zuckerman JD, Rokito A, Frozen shoulder: A consensus definition: J Shoulder Elbow Surg, 2011; 20(2); 322-25
2.. Zreik NH, Malik RA, Charalambous CP, Adhesive capsulitis of the shoulder and diabetes: A meta-analysis of prevalence: Muscles Ligaments Tendons J, 2016; 6; 26
3.. Uppal HS, Evans JP, Smith C, Frozen shoulder: A systematic review of therapeutic options: World J Orthop, 2015; 18; 263-68
4.. Cho CH, Bae KC, Kim DH, Treatment strategy for frozen shoulder: Clin Orthop Surg, 2019; 11(3); 249-57
5.. Le HV, Lee SJ, Nazarian A, Rodriguez EK, Adhesive capsulitis of the shoulder: Review of pathophysiology and current clinical treatments: Shoulder Elbow, 2016; 9(2); 75-84
6.. Distel LM, Best TM, Prolotherapy: A clinical review of its role in treating chronic musculoskeletal pain: P MR, 2011; 3(6 Suppl. 1); S78-S81
7.. Rabago D, Reeves KD, Doherty MP, Fleck M, Prolotherapy for musculoskeletal pain and disability in low- and middle-income countries: Phys Med Rehabil Clin N Am, 2019; 30(4); 775-86
8.. Hauser RA, Lackner JB, Steilen-Matias D, Harris DK, A systematic review of dextrose prolotherapy for chronic musculoskeletal pain: Clin Med Insights Arthritis Musculoskelet Disord, 2016; 9; 139-59
9.. Rabago D, Zgierska A, Fortney L, Hypertonic dextrose injections (prolo-therapy) for knee osteoarthritis: Results of a single-arm uncontrolled study with 1-year follow-up: J Altern Complement Med, 2012; 18; 408-14
10.. Waluyo Y, Budu , Bukhari A, Changes in levels of cartilage oligomeric proteinase and urinary C-terminal telopeptide of type II collagen in subjects with knee osteoarthritis after dextrose prolotherapy: A randomized controlled trial: J Rehabil Med, 2021; 53(5); jrm00196
11.. Reeves B, The natural history of the frozen shoulder syndrome: Scand J Rheumatol, 1975; 4; 193-96
12.. Boyle-Walker KL, Gabard DL, Bietsch E, A profile of patients with adhesive capsulitis: J Hand Ther, 1997; 10; 222-28
13.. Fernandes MR, Correlation between functional disability and quality of life in patients with adhesive capsulitis: Acta Ortop Bras, 2015; 23(2); 81-84
14.. Seven MM, Ersen O, Akpancar S, Effectiveness of prolotherapy in the treatment of chronic rotator cuff lesions: Orthop Traumatol Surg Res, 2017; 103(3); 427-33
15.. Page MJ, Green S, Kramer S, Manual therapy and exercise for adhesive capsulitis (frozen shoulder): Cochrane Database Syst Rev, 2014(8); CD011275
16.. Hanchard NCA, Goodchild L, Thompson J, A questionnaire survey of UK physiotherapists on the diagnosis and management of contracted (frozen) shoulder: Physiotherapy, 2011; 97; 115-25
17.. Akpancar S, Örsçelik A, Seven MM, Koca K, The effectiveness of prolo-therapy on failed rotator cuff repair surgery: Turk J Phys Med Rehabil, 2019; 65(4); 394-401
In Press
12 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.943244
13 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.943275
13 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.943411
13 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.942864
Most Viewed Current Articles
07 Mar 2024 : Case report 
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133
10 Jan 2022 : Case report 
DOI :10.12659/AJCR.935263
Am J Case Rep 2022; 23:e935263
19 Jul 2022 : Case report 
DOI :10.12659/AJCR.936128
Am J Case Rep 2022; 23:e936128
23 Feb 2022 : Case report
DOI :10.12659/AJCR.935250
Am J Case Rep 2022; 23:e935250