02 May 2023: Articles 
A Huge Malignant Ovarian Tumor: A Case Report
Unusual setting of medical care, Rare disease
Brahmana Askandar TjokroprawiroDOI: 10.12659/AJCR.939387
Am J Case Rep 2023; 24:e939387






Abstract
BACKGROUND: Huge ovarian tumors are rare. In developing countries, many women with huge ovarian tumors only seek consultation when the tumor has become very large. Most cases are benign, and only a few cases were reported to be malignant. This case report presents a case of huge malignant ovarian tumor with a final diagnosis of stage III epithelial ovarian cancer. The tumor was completely removed. The huge malignant ovarian tumor in this case report was completely excisable.
CASE REPORT: A 43-year-old woman visited the tertiary hospital in Surabaya Indonesia in early September 2020 with a complaint of an enlarged abdomen. The patients had 3 children and normal menstrual periods. Her bowel function was normal. The patient started to notice the abdominal enlargement at 3 months prior to seeking treatment. Ultrasound examination showed a unilocular cystic mass with a diameter of >25 cm, and a solid nodule with normal vascularity was seen. No ascites was noted. Histopathologic examination showed an ovarian mass weighing 9700 g with a size of 30×28×14 cm. The final result showed that the tumor was malignant; specifically, the tumor was a sero-mucinous adenocarcinoma of the left ovary, grade II, which had metastasized to the omentum.
CONCLUSIONS: Huge malignant ovarian tumors tend to be at an early stage when the diagnosis is made, and they are completely excisable.
Keywords: Carcinoma, Ovarian Epithelial, Giant Cell Tumors, Child, Humans, Female, Adult, Ovarian Neoplasms, Adenocarcinoma, Mucinous, Abdomen, Ascites, Indonesia
Background
Huge ovarian tumors are rare. Most patients seek treatment before the tumor becomes very large. In some developing countries, patients often come late to health facilities to seek treatment because of poverty. Patients with a huge ovarian tumor may experience pressure in the abdomen and heavy breathing, prompting them to seek treatment. A huge ovarian tumor may be benign or malignant [1–3], but most of the cases are benign, and only a few are malignant. An early-stage ovarian cancer is twice as large as an advanced-stage ovarian cancer, and a huge ovarian tumor does not always mean a tumor in an advanced stage [4]. We reported a rare case of a huge ovarian tumor with a final diagnosis of epithelial ovarian cancer.
Case Report
A 43-year-old woman visited the tertiary hospital in Surabaya Indonesia in early September 2020 with a complaint of an enlarged abdomen. The patients had 3 children and normal menstrual periods. Her bowel function was normal. The patient started to notice the abdominal enlargement at 3 months prior to seeking treatment. Ultrasound examination showed a unilocular cystic mass with a diameter of >25 cm, and a solid nodule with normal vascularity was seen. No ascites was noted. Computed tomography was not performed because of the patient’s low socioeconomic status. The cancer antigen 125 and carcinoembryonic antigen levels were 16.6 U/mL and 0.04 ng, respectively (within normal limit). Chest X-ray showed normal findings. Many patients in Indonesia come to the hospital with ovarian masses that already have grown very large.
The patient underwent surgery 1 week later. A frozen section was not planned because it was not available in the hospital. Frozen sections are not always available in most hospitals in Indonesia. In fact, frozen section examinations during surgery can only be performed in a few hospitals in Indonesia. The laboratory tests performed preoperatively showed the following normal findings: hemoglobin level, 11.7 gr/dL; bleeding time, 5 minutes; and clotting time, 10 minutes. Laparotomy was performed under general anesthesia. A midline incision extending up to 10 cm above the umbilicus was performed. After the incision, a huge left ovarian mass was seen, with mild adhesion to the omentum and left abdominal wall (Figure 1A, 1B). The uterus, right ovary, omentum, and peritoneum appeared normal, without any nodules. Adhesiolysis and left salpingooophorectomy were performed, followed by total abdominal hysterectomy, right salpingo-oophorectomy, and omentectomy. The patient’s hemodynamic condition remained stable until the end of the surgery. The operative time was 1 hour 15 minutes, and the amount of blood loss was 200 mL. All specimens were sent for pathological examination (Figure 2).
Histopathologic examination showed an ovarian mass weighing 9700 g with a size of 30×28×14 cm. The final result showed that the tumor was malignant; specifically, the tumor was a sero-mucinous adenocarcinoma of the left ovary, grade II, which had metastasized to the omentum. The contralateral ovary was normal, with no metastasis to the uterus. The patient underwent chemotherapy with 6 cycles of paclitaxel-carboplatin regimen and has lived for 2 years with no evidence of disease.
Discussion
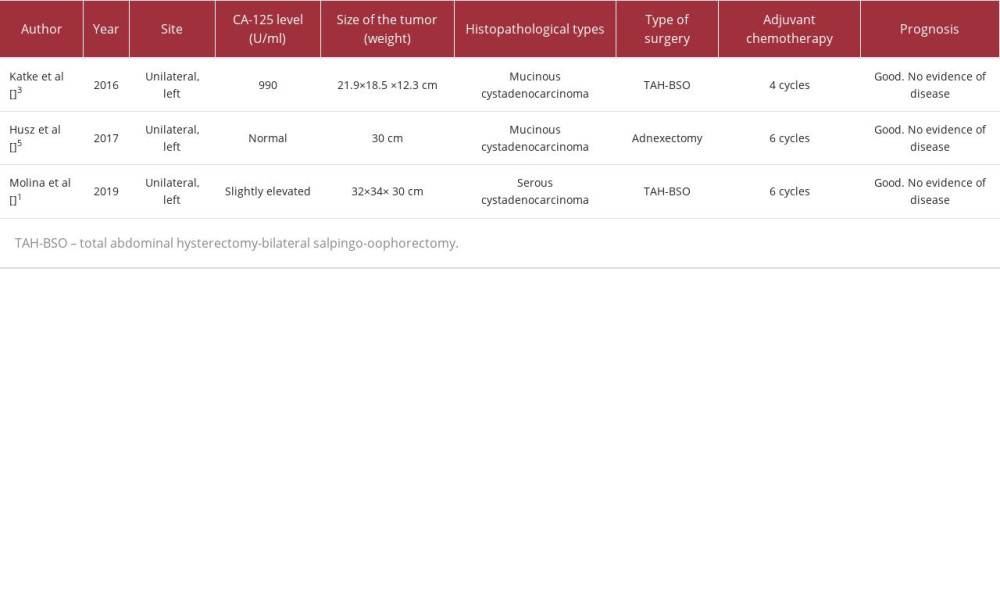
We present a rare case of a woman with a huge malignant ovarian tumor. There is currently no consensus on what constitutes a huge ovarian tumor. If the diameter of an ovarian mass is between 5 and 15 cm, it is termed large; if the diameter is greater than 20 cm, it is commonly referred to as giant [1]. Other authors regard a tumor larger than 10 cm or reaching above the umbilicus as large [5]. Most large ovarian tumors are benign, and only a few are malignant. To our knowledge, only a few studies have reported huge malignant ovarian tumors (Table 1) [6].
In this patient, the malignant ovarian tumor was unilateral (left ovary), similar to those of other case reports. The patient did not have specific symptoms until she noticed a large mass in the abdomen. Several case reports of large ovarian tumor have also shown that patients only experienced abdominal distension or pain, without any other specific symptoms [1,2]. Huge ovarian tumors do not always indicate that they are in the advanced stage; in fact, most cases of large malignant ovarian tumors are at an early stage. In our case, the patient was in stage III with micro-metastasis to the omentum.
In our patient, the cancer antigen (CA)-125 level was normal despite having a malignant ovarian cancer. A study showed that half of ovarian cancer patients with residual tumor after surgery had a normal CA-125 level, and Molina et al [1] also reported a case of giant ovarian cystadenocarcinoma with only slightly elevated CA-125 level. This study confirmed that malignant ovarian tissues do not always produce CA-125. Early diagnosis in ovarian cancer is challenging owing to the lack of early symptoms and absence of specific tumor marker for epithelial ovarian cancer, and not all epithelial ovarian cancer produces CA-125. The level of CA-125 is elevated in 80% of ovarian cancer patients and 20% of them have normal CA-125 level [1]. The most common symptoms of early-stage ovarian cancer in primary care medicine are lower abdominal pain and abdominal distention [7]. These symptoms are only noticed by the patient if the ovarian tumor is already large enough to cause symptoms. In our patient, no symptom was felt until the ovarian mass had already grown large.
We considered that ovarian cancers could be classified into 2 types based on their growth pattern. The first type includes ovarian cancers that grow locally, without spreading via lymphatic or vascular vessels to the other tissue. These tumors grow from being small ones to becoming very huge tumors without spreading to other tissues. The second type includes ovarian cancers that tend to spread distantly or to other tissues. Our patient had a unilateral ovarian mass from the left ovary, and the right ovary, omentum, and peritoneum appeared normal without any nodules; however, the histopathological examination showed omental metastasis. Two mechanisms of omental metastasis from ovarian cancer are known: direct surface spread and hematogenous spread [8,9]. In our case, it was very likely that the omental metastasis was caused by direct surface spread because there was omental adhesion with the ovarian tumor without any metastasis to other tissues or organs. A study showed that left malignant ovarian tumors are more likely metastasize to the omentum than are right malignant ovarian tumors [10].
The main management of a large ovarian tumor is removal by surgery. Large abdominal tumors may cause complications such as breathing difficulty, bloating, and pain, and removal of the tumor will relieve these symptoms. Laparoscopy is still limited as a first-line treatment for large adnexal cysts. Only a few surgeons perform laparoscopic management of exceedingly large ovarian cysts due to technological challenges, such as limited room. Furthermore, there is a danger of cyst rupture, intra-abdominal spillage, and malignant cell implantation at the trocar site. In terms of practicality and safety in comparison to laparoscopy, laparotomy is preferred [2].
In our case, solid nodules were detected by ultrasonography, and malignancy could not be ruled out despite the normal level of CA-125, so we performed total removal of the ovarian mass to prevent spillage. The clinical importance of ovarian cancer capsule rupture is still debatable, but we tried to remove the tumor completely because the patient had good hemodynamic status and the anesthetist team was well prepared. Total removal of a large ovarian tumor may cause splanchnic shock because tumor removal can release the compression of splanchnic vessels but drainage of the tumor during surgery can cause spillage of the cancer cells into the abdomen and sudden pulmonary edema [2]. As a result, meticulous intraoperative and postoperative vigilance is required during the management of these high-risk multidisciplinary cases to avoid undesirable consequences.
Surgical staging should be performed for early-stage ovarian cancer to accurately determine the stage, and complete debulking should be performed for advanced ovarian cancer. Systematic pelvic and para-aortic lymphadenectomy was not associated with longer overall or progression-free survival in patients with advanced ovarian cancer who had no macroscopically residual tumors after surgery [11]. In our patient, the tumor was completely removed without any gross residual tumor. Ovarian cancer with a larger tumor may be detected by ultrasonography earlier, which is also a possible reason for early surgery in patients with a large ovarian tumor. A large malignant ovarian tumor also tends to be at an early stage, so it can be removed without any residual tumor.
Our patient underwent chemotherapy because the histopathological examination showed a malignant ovarian mass with micro-metastasis in the omentum. The patient was in good condition with no evidence of disease for 2 years. Studies have shown that advanced ovarian cancer with no gross residual tumor after surgery has a better prognosis than those with gross residual tumor [12].
Conclusions
In conclusion, huge ovarian cancers are rare, and most of them are completely excisable and have a better prognosis.
Figures
References:
1.. Molina GA, Izurieta AN, Moyon MA, Giant ovarian cystadenocarcinoma in an adult patient, a rare finding in modern times: J Surg Case Rep, 2019; 2019(7); rjz207
2.. Fatema N, Mubarak Al Badi M, A postmenopausal woman with giant ovarian serous cyst adenoma: A case report with brief literature review: Case Rep Obstet Gynecol, 2018; 2018; 5478328
3.. Katke RD, Giant mucinous cystadenocarcinoma of ovary: A case report and review of literature: J Midlife Health, 2016; 7; 41
4.. Horvath LE, Werner T, Boucher K, The relationship between tumor size and stage in early versus advanced ovarian cancer: Med Hypotheses, 2013; 80; 684-87
5.. Grigore M, Murarasu M, Himiniuc LM, Large ovarian tumors in adolescents, a systematic review of reported cases, diagnostic findings and surgical management: Taiwan J Obstet Gynecol, 2021; 60; 602-8
6.. Husz V, Bus D, Vajda G, Extremely large epithelial ovarian cancer associated with pregnancy: A case report: Mol Clin Oncol, 2018; 8(1); 103-6
7.. Hamilton W, Peters TJ, Bankhead C, Risk of ovarian cancer in women with symptoms in primary care: Population based case-control study: BMJ, 2009; 339; b2998
8.. Pradeep S, Kim SW, Wu SY, Hematogenous metastasis of ovarian cancer: Rethinking mode of spread: Cancer Cell, 2014; 26(1); 77-91
9.. Lengyel E, Ovarian cancer development and metastasis: Am J Pathol, 2010; 177; 1053-64
10.. Ayhan A, Yüksel H, Dursun P, The spread pattern of right and left epithelial ovarian cancers: Eur J Gynaecol Oncol, 2010; 31; 654-57
11.. Harter P, Sehouli J, Lorusso D, A randomized trial of lymphadenectomy in patients with advanced ovarian neoplasms: N Engl J Med, 2019; 380; 822-32
12.. Polterauer S, Vergote I, Concin N, Prognostic value of residual tumor size in patients with epithelial ovarian cancer FIGO stages IIA–IV: Analysis of the OVCAD data: Int J Gynecol Cancer, 2012; 22; 380-85
Figures
In Press
06 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.942937
12 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.943244
13 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.943275
13 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.943411
Most Viewed Current Articles
07 Mar 2024 : Case report 
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133
10 Jan 2022 : Case report 
DOI :10.12659/AJCR.935263
Am J Case Rep 2022; 23:e935263
19 Jul 2022 : Case report
DOI :10.12659/AJCR.936128
Am J Case Rep 2022; 23:e936128
23 Feb 2022 : Case report
DOI :10.12659/AJCR.935250
Am J Case Rep 2022; 23:e935250