04 August 2020: Articles 
A Rare Case of Elongated Styloid Process Fracture
Rare disease
Kojiro Hirano1ABCEF*, Tomoaki Mori2B, Takahiro Suzuki3A, Yasuyuki Hinohira4A, Hitome Kobayashi1DDOI: 10.12659/AJCR.925405
Am J Case Rep 2020; 21:e925405






Abstract
BACKGROUND: An elongated styloid process occurs with Eagle syndrome and causes a variety of symptoms. Fracture of the elongated styloid process is a rare condition. With spontaneous fractures, appropriate treatment cannot be performed in many cases due to unexplained symptoms and indefinite complaints that are not thoroughly examined.
CASE REPORT: We encountered a case of fractured elongate styloid process reaching the hyoid bone. Based on the findings from cervical 3-dimensional computed tomography (3D-CT), we chose surgery using the transcervical approach instead of the intraoral approach. Symptoms resolved following surgery.
CONCLUSIONS: A fractured styloid process is a rare event, but it needs to be recognized. If drug therapy does not work, surgical treatment is needed and has been shown to be effective. Surgical therapies include an intraoral approach and a transcervical approach. In the case presented here, 3D-CT was very useful for diagnosis and surgery selection.
Keywords: Cough, Fractures, Spontaneous, Imaging, Three-Dimensional, Eagles, Hyoid Bone, Ossification, Heterotopic, Temporal Bone, Tomography, X-Ray Computed
Background
An elongated styloid process occurs with Eagle syndrome and causes a variety of symptoms [1]. Fracture of the elongated styloid process is a rare condition. With spontaneous fractures, appropriate treatment cannot be performed in many cases due to unexplained symptoms and indefinite complaints that are not thoroughly examined. We encountered a case of fractured elongate styloid process reaching the hyoid bone. Based on the findings from cervical 3-dimension computed tomography (3D-CT), we chose surgery using the transcervical approach instead of the intraoral approach. The symptoms resolved following surgery. The fractured styloid process is a rare event, but it needs to be recognized. Here, we report a case and present a review of the literature.
Case Report
A 45-year-old woman presented with fever, pain when swallowing, pain in the left submandibular region, ear pain, tooth pain, and an unusual sound heard upon swallowing. She had no health hazards (tobacco smoking, alcohol consumption, substance abuse) and no co-existing diseases. She had experienced a fracture of the left elongated styloid process at the age of 30, but no recent trauma. Her symptoms developed spontaneously after she had a cold. The symptoms were suspected to have been caused by coughing while she was ill, but the definite cause was unknown. Initially, she considered her symptoms to be due to her cold, but they persisted. She visited multiple hospitals and underwent cervical CT about 3 months later, which revealed a left styloid process fracture. The discomfort and unusual sound heard when swallowing remained.
The patient experienced pain accompanied by a loud sound in the left neck when she coughed. Her symptoms of pain when swallowing, ear pain, tooth pain, and the unusual sound upon swallowing worsened. The patient also had a fever and consulted our department. The left amygdala region was slightly hard at the initial examination. In addition, a pleural friction rub was heard near the left mandible. Cervical 3D-CT revealed a left giant elongated styloid process approximately 80 mm in length, reaching to the hyoid bone (Figure 1). Two fractures were present. The upper fracture showed malunion and was considered to be a previous fracture. The site of the lower fracture was consistent with the location where pleural friction was heard. The right styloid process was also elongated to 45 mm. The acute symptoms due to the fractures, including fever, left mandible tenderness, and left pleural friction rub, were alleviated with conservative treatment based on oral nonsteroidal anti-inflammatory drugs (NSAIDs) at 180 mg/d, carbamazepine at 200 mg/d, and pregabalin at 300 mg/d. However, other symptoms remained, including pain with swallowing, discomfort due to hyoid movement restriction when swallowing, earache associated with the glossopharyngeal nerve, and an audible sound during swallowing due to physical friction of the fractured styloid process itself. The patient underwent surgery approximately 3 months after onset of her symptoms.
Surgery was performed under general anesthesia using the transcervical approach. The skin incision was performed according to the method of resection of the submandibular gland. The deep side of the submandibular gland was separated, and the submandibular gland, facial artery and vein, and hypoglossal nerve were lifted en bloc in a cranial direction. The digastric muscle was placed caudal to maintain the operative field. On palpation, a bony ridge was confirmed. The fascia of the hypoglossal muscle was incised and the tip of the styloid process was exposed. The styloid process was grasped with a Pean forceps, and the attached muscles (the stylopharyngeus muscle and styloglossus muscle) were separated. On the hyoid bone side, the stylohyoid ligament with ossification toward the lesser horn of the hyoid bone was dissected and bluntly separated in a cranial direction. On the fracture side, the connective tissue extending into the fracture space was dissected, and the caudal part of the styloid process was extracted from the fracture site. The tip of the remaining styloid process in the cranial side was made blunt. After a drain was inserted, the wound was closed. The extracted bone tissue was 30 mm in length, and its tip had a nodular shape (Figure 2).
Pain and discomfort in the fracture site disappeared immediately after surgery, and the radiating pain to the ear and unusual sound heard upon swallowing resolved 1 month after a previous fracture. The lower fracture (double arrows) was consistent with the location where pleural friction was heard. H – hyoid bone. surgery. The discomfort when swallowing did not improve in the early postoperative period. In addition, mild difficulty in swallowing developed after surgery and it was attributed to the dissection of the stylopharyngeus muscle and styloglossus muscle. Endoscopic evaluation of swallowing was performed, but there was no difficulty in swallowing or aspiration, and the patient was followed up without treatment. The discomfort upon swallowing and the perceived difficulty in swallowing improved gradually. These symptoms resolved 10 months after surgery, and no recurrence has been noted since that time. The right elongated styloid process has remained asymptomatic upon follow-up.
Discussion
In 1937, Eagle [1] examined the relationship between the length of the styloid process and various symptoms and proposed the resection of the styloid process. Since then, the elongated styloid process has also been referred to as Eagle syndrome.
Eagle defined a styloid process of 25 mm or longer as being elongated and reported an elongated styloid process was present in 4% of autopsies, among which 4% were symptomatic [2]. A recent study [3] reported that the frequency is higher than that reported by Eagle. Currently, many authors define a styloid process that is 30 mm or longer as being elongated [4]. Correl et al. [5] reported that the proportion of patients with a styloid process that is longer than 30 mm was up to 18.2%, but very few were symptomatic. Fewer studies have reported on a large styloid process as in the present case. Kaufmann et al. [4] examined the styloid process in 2000 autopsies and reported that only 2 were longer than 50 mm. An elongated styloid process is bilateral in the majority of cases, but the symptoms are almost always unilateral [2,5]. In our case, the right styloid process was 45 mm in length but asymptomatic.
An elongated styloid process causes multiple symptoms, largely due to physical stimulation directly caused by the structure, restriction in the movement of the hyoid bone, and compression of nerves such as the cranial nerve and cervical sympathetic nerve (Table 1). Symptoms may result from inflammation of the ligament attached to the styloid process, degeneration of the styloid process and ligament with age, changes in the mobility of the styloid process, and changes in the swallowing muscle function [6]. In our case, these factors might have contributed to the persistent pain and discomfort. The previous fracture of the elongated styloid process showed mal-union, and the ligament was completely ossified, forming a long bony diaphysis and resulting in reduced mobility. This reduced mobility decreased the tolerance of the styloid process-stylohyoid ligament (ossification)-hyoid bone structure against external forces, which may have led to the fracture when the patient had a strong cough.
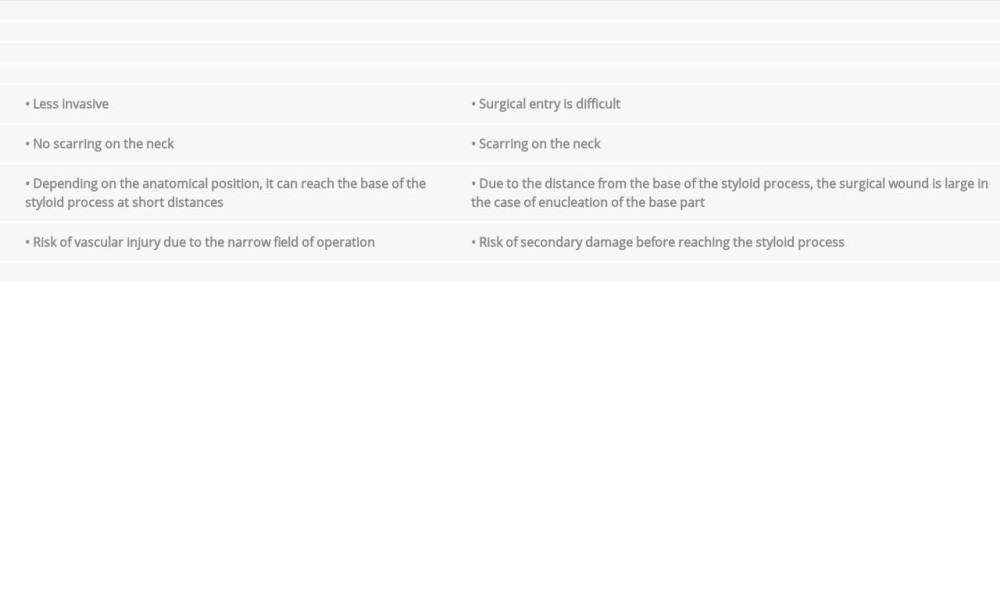
Treatment strategies for an elongated styloid process include conservative and invasive treatments. Conservative treatment includes NSAIDs and antiepileptic drugs, while surgical treatment includes an intraoral or a transcervical approach (Table 2). The use of the intraoral approach has been frequently reported [1,6], but this approach is not practical for dissecting and retrieving the joint part with the hyoid bone when the whole length of the ligament of the styloid process involving the joint part of the hyoid bone is ossified [7]. According to the 3D-CT findings, the ossification in the present case extended close to the hyoid bone, and the fractured part was deformed and thickened. Therefore, we considered the transcervical approach as being safer and more efficient than the intraoral approach for this case. Many studies have reported that partial resection is sufficiently effective. An approach using a skin incision in the submandibular region was reported to be sufficiently effective when the symptoms were related to the submandibular region and hyoid bone only [8]. We employed the transcervical approach using skin incision in the submandibular region because the symptoms had developed and were exacerbated because of the fracture and there was an aesthetic need.
The fracture of an elongated styloid process is a very rare condition. The fracture is caused by trauma in the vast majority of the cases, although other causes such as dental treatment have been reported [9]. Arechvo et al. [10] reported that traumatic fracture is often caused by car accidents and can also be caused by dental treatment and tonsillectomy. Spontaneous fracture may occur due to swallowing, yawning, coughing, or sudden laughing [10]. The underlying causes of traumatic fracture are clear, while those of spontaneous fracture are not; therefore, patients may often be left undiagnosed and the symptoms may be interpreted as “symptoms of unknown cause” or “indefinite complaints.” Recently, many studies have used 3D-CT or 3D-CT angiography when an elongated styloid process is suspected [3,7]. The use of 3D-CT is recommended because it is better than panoramic X-ray in detecting minor fractures. Further, it can confirm the thickness of the styloid process, the presence of bone union with the hyoid bone, and the positional relationship with the surrounding vessels. Because minor fractures often cannot be detected with panoramic X-ray, the frequency of the disease is expected to be higher than reported.
Regarding the treatment of fracture of the styloid process, Reichart et al. [11] reported a case of fracture due to dental treatment that was conservatively treated, with symptoms resolving after follow-up. They suggested that surgical treatment is indicated for individuals with an elongated styloid process or significant dislocation of the styloid process. Smith et al. [12] reported a patient with a fracture of the styloid process who had been conservatively treated with an intermaxillary fixation for 3 weeks without improvement. The authors performed surgery using an intraoral approach, and the symptoms resolved immediately after retrieval of the bone fragment. Hampf et al. [13] reported that among 20 patients in whom the bone fragments were retrieved by surgery, 1 achieved remission, 12 were resolved, 6 were unchanged, and 1 showed exacerbation. The possibility of psychogenic pain needs to be confirmed before considering surgery. Conservative treatment may be effective for patients with fracture of the styloid process when there is little dislocation of the styloid process.
Such treatment should be performed first. After a period of follow-up, surgical treatment using the intraoral approach or the transcervical approach is recommended for patients with persistent symptoms. In the present case, we performed conservative treatment with NSAIDs, carbamazepine, and pregabalin for 3 months, but the symptoms did not resolve. The 3D-CT findings revealed that the styloid hyoid ligament was ossified, and since the area of fracture was deformed, fused, and abnormally thickened, we chose the transcervical approach instead of the intraoral approach and the patient’s symptoms resolved. The thickness of the styloid process and the state of fracture can be determined with 3D-CT. In cases in which the styloid process is very thick, as in this case, 3D-CT is very useful in deciding the treatment method. We recommend performing 3D-CT in surgical cases.
Conclusions
Fracture of an elongated styloid process is rarely reported, but spontaneous fractures can occur due to nontraumatic events such as coughing. It is necessary to choose a treatment method that is appropriate to the case. We obtained an accurate diagnosis from 3D-CT, which was also useful in selecting the appropriate surgical method.
Figures
References:
1.. Eagle WW, Elongated styloid process: Arch Otolaryngol, 1937; 25; 584-86
2.. Eagle WW, Elongated styloid process: Arch Otolaryngol, 1958; 67; 172-76
3.. Eraslan C, Ozer MA, Govsa F, Relationship of stylohyoid chain and cervical internal carotid artery detected by 3D angiography: Surg Radiol Anat, 2017; 39; 897-904
4.. Kaufmann SM, Elzay RP, Irish EF, Styloid process variation. Radiologic and clinical study: Arch Otolaryngol, 1970; 91; 460-63
5.. Correl RW, Jensen JL, Taylor JB, Rhyne RR, Mineralization of the styloid-stylomandibular ligament complex: Oral Surg Oral Med Oral Pathol, 1979; 48; 286-91
6.. Ghosh LM, Siba PD, The syndrome of elongated styloid process: Ayris Nasus Larynx, 1999; 26; 169-75
7.. Galletta K, Granata F, Longo M, An unusual internal carotid artery compression as a possible cause of Eagle syndrome – a novel hypothesis and an innovative surgical technique: Surg Neurol Int, 2019; 10; 174
8.. Sakaguti H, Asano J, Sado F, [An elongated styloid process surgically shortened with external approach]: The Society of Practical Otolaryngology, 2000; 93; 971-77 [in Japanese]
9.. Khan HM, Fraser AD, Daws S, Fractured styloid process masquerading as neck pain: Cone-beam computed tomography investigation and review of the literature: Imaging Sci Dent, 2018; 48; 67-72
10.. Arechvo I, Giniunaite AM, Balseris S, Bilateral fracture of the styloid process with parapharyngeal emphysema: Otol Neurotol, 2014; 35; 155-56
11.. Reichart PA, Sooss W, Fracture of the styloid process of the temporal bone: An unusual complication of dental treatment. Report of a case: Oral Surg Oral Med Oral Pathol, 1976; 42(2); 150-54
12.. Smith RG, Cherry JE, Traumatic Eagle’s syndrome: Report of a case and review of the literature: J Oral Maxillofac Surg, 1976; 46; 606-9
13.. Hampf G, Aalberg V, Tasanen A, Nyman C, A holistic approach to stylalgia: Int J Oral Maxillofac Surg, 1986; 15; 549-52
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133