13 August 2020: Articles 
Three Cases of Pediatric Multisystem Inflammatory Syndrome Associated with COVID-19 Due to SARS-CoV-2
Unusual clinical course, Challenging differential diagnosis
Sabrina M. Heidemann12ABCDEF*, Bradley Tilford12CDE, Christian Bauerfeld12CDE, Amarilis Martin1BCDEF, Richard U. Garcia12CDE, Lauren Yagiela12CDE, Ashok P. Sarnaik13CDEDOI: 10.12659/AJCR.925779
Am J Case Rep 2020; 21:e925779






Abstract
BACKGROUND: Coronavirus disease 2019 (COVID-19) infection commonly presents as fever, cough, and shortness of breath in adults. Children are thought to have milder respiratory symptoms and to recover more quickly. We describe a new presentation of COVID-19 infection in children consisting of multisystem inflammation with decreased left ventricular function and evidence of lung disease.
CASE REPORT: Three children presented with fever, conjunctivitis, dry and cracked lips, rash, and/or cervical lymphadenopathy for at least 5 days. Two of these children required mechanical ventilation, and 1 of the 2 needed extracorporeal membrane oxygenation (ECMO) to support cardiorespiratory function. All of these children had moderate to severe hyponatremia and lymphopenia, which is usually seen in COVID-19. They were treated with intravenous immunoglobulin and high-dose aspirin. All of the children recovered.
CONCLUSIONS: Early recognition of children with multisystem inflammation is important because they are at increased risk for deterioration. Treatment with intravenous immunoglobulin and aspirin was used because this regimen has been shown to be beneficial in vasculitis of Kawasaki disease. The development of shock due to cardiac involvement may require ECMO.
Keywords: Aspirin, COVID-19, Extracorporeal Membrane Oxygenation, Immunoglobulins, Intravenous, Mucocutaneous Lymph Node Syndrome, antipyretics, Betacoronavirus, COVID-19, Child, Child, Preschool, Conjunctivitis, Coronavirus Infections, Exanthema, Fever, Hyponatremia, lymphadenopathy, Lymphopenia, Pandemics, Pneumonia, Viral, Respiration, Artificial, SARS-CoV-2, Systemic Inflammatory Response Syndrome, Vasculitis
Background
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was discovered in early December 2019 in Wuhan, China and has since spread throughout China and to 185 countries [1,2]. Adults commonly present with fever, cough, and difficulty in breathing. Lymphopenia is usually present and ground glass opacities are seen on chest computed tomography (CT) [3]. Most children with coronavirus disease 2019 (COVID-19) have milder symptoms and recover from the disease within 1 to 2 weeks. They commonly present with fever, cough, and fatigue, while some have sore throat, rhinorrhea, and congestion [4]. Vomiting and diarrhea have also been described. Laboratory findings include lymphopenia, elevation in serum troponin, liver enzymes, D-dimer, and ferritin. C-reactive protein and sedimentation rate, along with cytokines such as tumor necrosis factor α, interleukin (IL)-4, IL-6, and IL-10, are elevated [2]. We report 3 children who presented with vasculitis and cardiac manifestations who responded positively to intravenous immunoglobulin and aspirin. The first child was exposed to his mother who tested positive for SARS-CoV-2, and he later had IgG antibodies to SARS-CoV-2, which were detected after hospital discharge. The second child tested positive for SARSCoV-2 by nasopharyngeal swab and later had IgG antibodies to SARS-CoV-2. The third child was exposed to his severely ill grandfather who tested positive for SARS-CoV-2, but the child was negative for SARS-COV-2 and antibodies were not tested. All of these children presented at the end of April 2020.
Case Reports
CASE 1:
A previously healthy 7-year-old boy presented with abdominal pain, vomiting, diarrhea, fever, chest pain, difficulty in breathing, and a maculopapular rash involving the back and extremities for 1–2 days. His mother was treated for pneumonia and had a positive SARS-CoV-2, 12 days prior to the onset of the boy’s symptoms. The boy was tested for SARS-CoV-2 (real-time [RT]-PCR, Cepheid, Sunnyville, CA) at the onset of symptoms, and results were negative at this time. On examination, his heart rate was 168 beats/min; respiratory rate, 18/min; blood pressure, 97/54 mmHg; oral temperature, 37.8°C; and 95% oxygen saturation on room air. His respiratory, cardiovascular, and abdominal examinations were initially normal. No conjunctivitis or lymphadenopathy was noted. There was a morbilliform rash on his back, arms, hands, and feet without involvement of the palms and soles. His clinical characteristics are shown in Table 1. His sodium was 129 mmol/L and chlo-ride 92 mmol/L. No viruses were detected on the respiratory viral panel. The rest of the laboratory tests are shown in the Table 2. Chest x-ray showed decreased lung volume and mild peribronchial cuffing. Abdominal CT showed significant gall-bladder thickening consistent with acute cholecystitis. Twelve hours after admission he developed hypoxia and required an escalation of his respiratory support from 2 L/min nasal cannula to 15 L/min high-flow nasal cannula. He developed worsening hypoxia and required increased respiratory support and endotracheal intubation with mechanical ventilation a day after admission. Chest x-ray showed new patchy opacities in both lungs and small pleural effusions bilaterally. He remained on mechanical ventilation for 4 days. He developed hypotension requiring multiple fluid boluses and continuous infusion of epinephrine. His electrocardiogram (ECG) showed sinus tachycardia. An echocardiogram showed mildly decreased left ventricular function, mild mitral insufficiency, and dilation of the mean left coronary artery (diameter: 0.39 cm, Z-score: 2.3) and the proximal left arterial descending coronary artery (diameter: 0.32 cm, Z-score: 2.1) as shown in Figure 1. He subsequently developed swollen feet and hands and conjunctival injection. He was treated for vasculitis on the fourth day of symptoms with aspirin and intravenous immunoglobulin (IVIG). He required a second dose of IVIG as fever persisted for more than 36 h following the first infusion. He remained afebrile following the second IVIG infusion. He received antibiotics throughout his hospitalization. He improved over the next 7 days and was discharged from the hospital. His IgG antibodies for SARSCoV-2 were positive by immunoassay (Abbott, Abbott Park, IL) on a follow-up visit that occurred 2 weeks after presentation.
CASE 2:
A 6-year-old girl presented with syncope lasting 1 min, fever for 3 days, and a new onset of abdominal pain and a maculopapular rash on her wrists, palms, arms, and abdomen. Swelling of hands and feet had resolved prior to presentation. On physical examination, her heart rate was 138 beats/min; respiratory rate, 22/min; blood pressure, 119/73 mmHg; and temperature, 39.5°C. Her throat was erythematous without exudates. Her respiratory, cardiovascular, and abdominal examinations were normal. Her clinical characteristics are shown in Table 1. A rapid strep screen was positive. Her chest x-ray was normal. She was sent home with amoxicillin with a diagnosis of possible streptococcal pharyngitis versus acute viral syndrome.
She returned to the hospital 3 days later with persistent fever and rash, and abdominal pain with a new onset of conjunctivitis and shortness of breath. Her only intake was oral electrolyte solution and fruit juice. On examination, her heart rate was 122 beats/min; respiratory rate, 40/min; blood pressure, 70/30 mmHg; and oral temperature 36.8°C. She had conjunctival injection and no cracking of the lips or a strawberry tongue. Her oxygen saturation was 90% on room air, and she was tachypneic with intercostal retractions. Auscultation revealed a gallop rhythm. Capillary refill time was 5 s. Her abdomen was slightly tender to palpation. A maculopapular rash was noted on her arms and legs. Her chest x-ray showed decreased lung volume, prominent heart size, and central and basilar pulmonary markings consistent with a viral process. She was treated with a fluid bolus, ceftriaxone, and vancomycin. A continuous infusion of epinephrine was started due to persistent poor perfusion. Her sodium concentration was 118 mmol/L and chloride was 84 mmol/L. Three percent saline was administered. Liver enzymes were within normal limits. Capillary blood gas showed a pH 7.42 and PCO2 was 35 torr. Her respiratory viral panel did not detect any viruses. Her nasopharyngeal secretions tested positive for SARSCoV-2 by RT-PCR (Cepheid). The rest of her laboratory results are shown in Table 3.
During the first 7 h of admission to the pediatric intensive care unit, hypotension was treated with intravenous infusion of dopamine and epinephrine. Initial ECG showed low voltages in the limb leads, PR interval prolongation, and early repolarization in the lateral precordial leads. Echocardiogram was remarkable for mildly depressed left ventricular function, mild tricuspid/mitral incompetence, and normal coronary anatomy. She was treated for vasculitis on her sixth day of symptoms with aspirin and IVIG. Clindamycin was added for possible streptococcal endotoxemia. Respirations were supported with high-flow nasal cannula up to 10 L/min. She developed an intermittent atrioventricular dissociation with persistent accelerated junctional tachycardia and hypotension. An acute episode of hypoxia occurred with possible seizure activity and subsequent bradycardia and cardiac arrest. Return of spontaneous circulation (ROSC) was achieved in less than 5 min with bag-mask ventilation and chest compressions. Following ROSC, a code dose (0.01 mg/kg) of epinephrine was administered for hypo-tension. The child was subsequently intubated without incident.
She was unable to be weaned from 100% oxygen and remained on epinephrine and dopamine infusions. Approximately 4 h following intubation, she developed nonsustained ventricular tachycardia for which she was given amiodarone. A repeat echocardiogram was performed and demonstrated worsening of left ventricular function. She was subsequently cannulated for veno-arterial extracorporeal membrane oxygenation (ECMO) given worsening hemodynamic instability and arrhythmias. She required ECMO for 5 days, was weaned off and recovered. Her IgG antibodies for SARS-CoV-2 were positive by immunoassay (Abbott, Abbott Park, IL) 2 weeks after presentation.
CASE 3:
A previously healthy 5-year-old boy presented with a 6-day history of fever, 2-day history of conjunctivitis, and 1-day history of decreased oral intake, lethargy, and mild abdominal pain. SARS-CoV-2 was absent from his nasopharyngeal secretions (RT-PCR, Cepheid), but his grandfather had tested positive for SARS-CoV-2 and required intensive care unit admission for respiratory illness. On examination, the boy’s heart rate was 104 beats/min; respiratory rate, 24/min; blood pressure, 80/55 mmHg; axillary temperature, 37°C; and an oxygen saturation of 98% on room air. He had conjunctival injection and shotty cervical lymph nodes. The rest of his physical examination was normal. Chest x-ray showed decreased lung volume with bilateral perihilar opacities and a mild prominence of the cardiac silhouette. Small bilateral pleural effusions were noted. Abdominal ultrasound showed a dilated common bile duct and mild splenomegaly. ECG was normal. Echocardiogram showed low-normal left ventricular function, a trace global pericardial effusion, and normal cardiac anatomy. He had a sodium of 124 mmol/L, chloride 88 mmol/L, normal aspartate aminotransferase and alanine aminotransferase, a white blood cell count of 6100/mm3, lymphocyte count of 600/mm3, neutrophil count of 4900/mm3, troponin (high sensitivity) of 44 ng/mL, and a ferritin of 378.9 ng/mL. The C-reactive protein (CRP) was initially 148.3 mg/dL on admission and fell to 50.4 mg/dL 5 days later. No viruses were detected on the respiratory viral panel. The patient was treated with aspirin and IVIG on his seventh day of symptoms. His fever resolved, and he was discharged home only to return the next day with high fever and lethargy. A second dose of IVIG was administered, after which he improved and was discharged home after 2 days.
Discussion
The 3 cases of vasculitis due to SARS-CoV-2 infection presented at the end of April 2020. Initially, these children were diagnosed as incomplete Kawasaki disease because they met the criteria set by the American Heart Association in 2017 [6]. The criteria for Kawasaki disease include (1) fever lasting more than 5 days, (2) erythema of the palms and soles or more commonly edema of the hands and feet, (3) periungual peeling, (4) diffuse rash, (5) conjunctival injection, (6) erythema of the lips and oral cavity, (7) cervical lymphadenopathy, and (8) exclusion of other diseases [5]. Coronary artery abnormalities including dilation of coronary arteries and aneurysms may also occur. Evidence of myocarditis is commonly seen but patients rarely present with hemodynamic instability and shock [6,7]. Incomplete Kawasaki disease occurs in children <1 year or ≥5–9 years of age, which is outside the usual age group of 1–4 years. It is defined as fever with 2 or 3 of the principal clinical findings described above in the guidelines [8]. In addition, the American Heart Association has 6 laboratory and echocardiography criteria that may aid in making the diagnosis [9]. In spite of meeting criteria for incomplete Kawasaki disease including physical attributes and laboratory evidence of severe inflammation, lymphopenia which is not typically seen in Kawasaki disease was present in all 3 children. Also, myocardial dysfunction and hyperferritinemia are not usually observed in Kawasaki disease to the degree observed. All 3 children had a partial response to IVIG in that 2 doses were required in 2 of the cases and ECMO for cardiovascular support in the other. The arrhythmias may have been related to the inflammation and/or ischemia of the myocardium and conduction system.
In the United Kingdom, the North Central London Clinical Commissioning Group released a statement on April 26, 2020, with concerns of children presenting with abdominal symptoms, cardiac inflammation, and Kawasaki disease with laboratory findings similar to children with COVID-19, whether or not the child tested positive or negative for SARS-CoV-2 [10]. The presentation of these symptoms after known exposure to SARS-CoV-2 in the absence of known active infection suggests that this illness is postinfectious. One of the earliest reports was a case in which SARS-CoV-2 was thought to cause Kawasaki disease in a 6-month-old [11]. This was followed by a report of 8 children with similar manifestations to Kawasaki disease due to SARS-CoV-2, which is now known to be a new syndrome called multisystem inflammatory syndrome in children (MIS-C). The disorder likely occurs after SARS-CoV-2 infection and the child may test negative for SARS-CoV-2 [12]. In our institution, we have seen a surge of children with MIS-C who tested positive for SARS-CoV-2 or had significant SARS-CoV-2 exposure despite a negative PCR test. However, it is likely that this disease is a postinfectious complication as shown in 2 of our patients who tested positive for IgG antibodies.
Conclusions
As more pediatric cases accumulate, it is becoming clearer that the response to SARS-CoV-2 infection in some children is not limited to the lungs but is instead systemic, with cutaneous, generalized vasculitis and myocarditis. It is important to quickly recognize these children because they are at increased risk for significant deterioration. Early treatment with aspirin and IVIG may be considered because this regimen is the recommended treatment for the vasculitis of Kawasaki disease. Progression of cardiac failure may require ECMO, and referral to the appropriate center is recommended.
References:
1.. Huang C, Wang Y, Li X, Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China: Lancet, 2020; 395(10223); 497-506
2.. Shen KL, Yang YH, Jiang RM, Updated diagnosis, treatment and prevention of COVID-19 in children: Experts’ consensus statement (condensed version of the second edition): World J Pediatr, 2020; 16(3); 232-39
3.. Guan WJ, Ni ZY, Hu Y, Clinical characteristics of coronavirus disease 2019 in China: N Engl J Med, 2020; 382(18); 1708-20
4.. , Coronavirus disease 2019 in Children – United States, February 12–April 2, 2020: Morb Mortal Wkly Rep, 2020; 69(14); 422-26
5.. Singh S, Jindal AK, Pilania RK, Diagnosis of Kawasaki disease: Int J Rheum Dis, 2018; 21(1); 36-44
6.. McCrindle BW, Rowley AH, Newburger JW, Diagnosis, treatment, and long-term management of Kawasaki disease: A scientific statement for health professionals from the American Heart Association: Circulation, 2017; 135(17); e927-99
7.. Dionne A, Dahdah N, Myocarditis and Kawasaki disease: Int J Rheum Dis, 2018; 21(1); 45-49
8.. Yu JJ, Diagnosis of incomplete Kawasaki disease: Korean J Pediatr, 2012; 55(3); 83-87
9.. Newburger JW, Takahashi M, Gerber MA, Diagnosis, treatment, and long-term management of Kawasaki disease: A statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association: Circulation, 2004; 110(17); 2747-71
10.. , Critical Update – Children and Paediatric Shock, 2020 http://coronavirus.ncl.nhs.sitekit.net/coronavirus-updates/critical-update-children-and-paediatric-shock/109225
11.. Jones VG, Mills M, Suarez D, COVID-19 and Kawasaki disease: Novel virus and novel case: Hosp Pediatr, 2020; 10(6); 537-40
12.. Riphagen S, Gomez X, Gonzalez-Martinez C, Hyperinflammatory shock in children during COVID-19 pandemic: Lancet, 2020; 395(10237); 1607-8
Tables
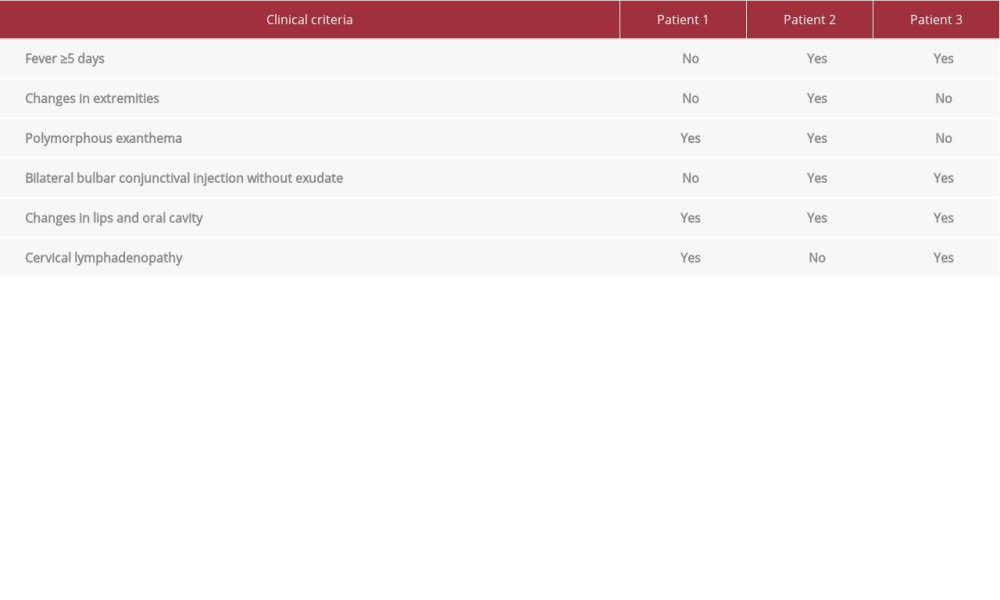 Table 1.. Clinical criteria for multisystem inflammatory syndrome in children.
Table 1.. Clinical criteria for multisystem inflammatory syndrome in children.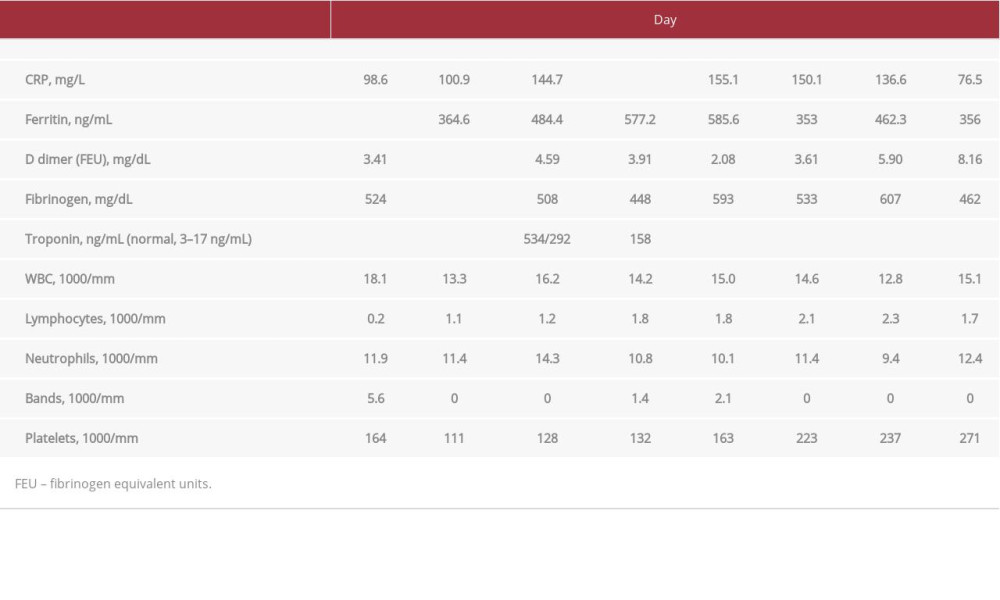 Table 2.. Laboratory findings for Case 1.
Table 2.. Laboratory findings for Case 1.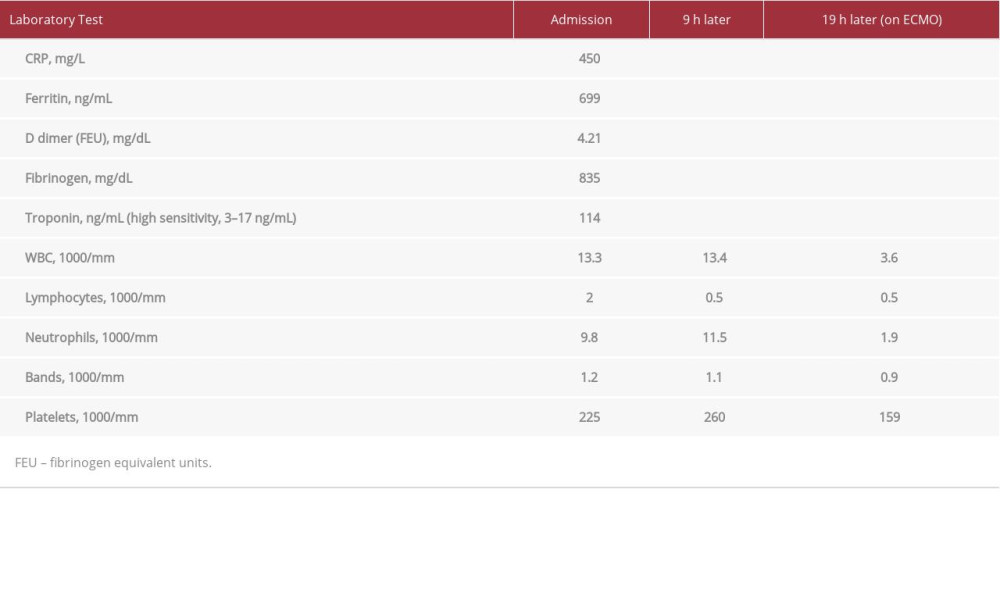 Table 3.. Laboratory findings for Case 2.Table 1.. Clinical criteria for multisystem inflammatory syndrome in children.Table 2.. Laboratory findings for Case 1.Table 3.. Laboratory findings for Case 2.
Table 3.. Laboratory findings for Case 2.Table 1.. Clinical criteria for multisystem inflammatory syndrome in children.Table 2.. Laboratory findings for Case 1.Table 3.. Laboratory findings for Case 2. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133