06 July 2023: Articles 
Recurrent Bioprosthetic Valve Endocarditis in Intravenous Drug Users
Unusual clinical course, Challenging differential diagnosis, Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents, Adverse events of drug therapy, Educational Purpose (only if useful for a systematic review or synthesis)
Dana Sadaqa1BDEFG*, Amro Daoud2ABD, Fuad Zeid2A, Hamza M. AlsaidDOI: 10.12659/AJCR.939292
Am J Case Rep 2023; 24:e939292






Abstract
BACKGROUND: We report 2 cases of recurrent right-sided endocarditis in 2 young patients known to be intravenous (i.v.) drug users. We highlight the importance of early diagnosis and management, especially in recurrent infection, which has a higher mortality rate and poor prognostic outcome despite antibiotic treatment.
CASE REPORT: A 30-year-old woman with a medical history of active i.v. drug use and tricuspid valve replacement owing to Serratia marcescens endocarditis 2 months prior to presentation was admitted to the Intensive Care Unit for septic shock. The patient did not respond to i.v. fluids and required vasopressors. Blood cultures returned positive for S. marcescens again. The antibiotic regimen consisted of meropenem and vancomycin. The patient underwent redo sternotomy, explant of old tricuspid valve bioprosthesis, debridement of tricuspid valve annulus, and bioprosthetic valve replacement. She continued antibiotic treatment during hospital admission for 6 weeks. In another similar case, a 30-year-old woman, also an i.v. drug user, was admitted to the hospital for tricuspid bioprosthetic valve S. marcescens endocarditis after tricuspid valve replacement 5 months prior to her presentation with S. marcescens endocarditis. Her antibiotic regimen consisted of meropenem and vancomycin. She was eventually transferred to a tertiary cardiovascular surgery center for further case management.
CONCLUSIONS: In the setting of recurrent bioprosthetic valve S. marcescens endocarditis, it is suggested that treatment should be more focused on source control, including cessation of i.v. drug abuse and providing appropriate antibiotic treatment to prevent recurrence because, in the case of recurrence, morbidity and mortality risk can increase significantly.
Keywords: Endocarditis, Endocarditis, Bacterial, Serratia marcescens, Female, Humans, Adult, drug users, Vancomycin, meropenem, Substance Abuse, Intravenous, Anti-Bacterial Agents
Background
Infective endocarditis (infective endocarditis) caused by
Among the Enterobacteriaceae group, it is rare that any of the microorganisms in this group is resistant to carbapenems through production of beta-lactamases, but some strains of Serratia have been found to be resistant to carbapenems by 2 mechanisms either through beta-lactamase production or diminished outer membrane permeability and AmpC cephalosporinase production [2]. In the 2 cases presented here, meropenem was used as part of the treatment regimen and thus could have led to recurrence.
We present 2 cases of recurrent
Case Reports
CASE 1:
A 30-year-old woman with a body mass index of 25 had a significant medical history of active i.v. heroin use for a 5-year period and tricuspid valve replacement due to S. marcescens endocarditis 2 months prior to this incident presentation. The patient presented to the Emergency Department (ED) with fever, chills, shortness of breath, and chest pain. Laboratory test results revealed a WBC count of 20×109/L and a C-reactive protein level of 20 mg/L. She was later admitted to the Intensive Care Unit because of septic shock, as her clinical condition worsened and her systolic blood pressure dropped to 85 mmHg. She also showed signs of confusion and mental disorientation. The patient did not respond to i.v. fluids and required vasopressors. Owing to the recent medical history of infective endocarditis and the patient’s symptoms, blood cultures were taken. A trans-esophageal echocardiogram showed a bio-prosthetic valve in the tricuspid position with thickened leaflets and 1.7×1-cm mobile vegetation and infection (Figure 1).
The patient underwent redo sternotomy, an explant of an old tricuspid valve bioprosthesis, debridement of tricuspid valve annulus, and valve replacement.
The initial antibiotic regimen consisted of gentamicin 3 mg/kg/day divided twice per day and ciprofloxacin 200 mg i.v. twice daily. The patient’s blood cultures again came back positive for
CASE 2:
In another very similar case, a 30-year-old female patient with a body mass index of 22 was admitted to the hospital for tricuspid bioprosthetic valve S. marcescens endocarditis after tricuspid valve replacement 5 months prior to her incident presentation. The patient remained healthy during the prior 5-month period after her tricuspid valve replacement with a bio-prosthesis, with no signs or symptoms of infection. However, the patient continued i.v. drug use during this period after the surgery. She had been a cocaine and heroin i.v. drug user for over 3 years. She presented to the ED with pleuritic chest pain and night sweats. On physical examination, her temperature was 38.9°C, and she had edema of the lower extremities and a grade 3/6 systolic murmur without any signs of radiation. Laboratory test results revealed a WBC count of 15×109/L and an erythrocyte sedimentation rate of 40 mm/h. Transesophageal echocardiography (TEE) was performed, and the size of the vegetation on the valve was found to be 0.68×0.87 cm (Figure 2).
Her initial antibiotic regimen consisted of ciprofloxacin 200 mg i.v. twice daily until the blood cultures were reported. The patient’s antibiotic regimen was switched to i.v. meropenem 2 g every 8 h and i.v. vancomycin 2 g every 24 h for 4 weeks based on cultures, and she was eventually transferred to a tertiary cardiovascular surgery center. No signs of valvular failure, no changes in ECG or abscess, or any indications for surgery were seen in the patient; therefore, a second surgery was not needed. The patient had a follow-up after 2 months. Blood cultures were negative, and TEE showed no vegetations on the prosthetic tricuspid valve.
Discussion
It is possible in our first case that the first infection was not properly treated, as blood cultures were negative after the first infection, but valve cultures were not repeated after treatment had ended, as the patient had a bioprosthetic valve. We believe that the insufficient treatment period of this patient’s previous infection and continued i.v. drug use had contributed the most to the relapse of infection. The patient underwent a TEE after 1 month of finishing the treatment, and her valves showed no signs of vegetation or infection.
Also, recurrent tricuspid valve endocarditis, despite valve replacement for the same infection, warrants investigations to rule out possible distant seeding that is unique to
A previous study on 19 cases of endocarditis caused by
Another report of
Cases of drug abuse-associated left-sided infective endocarditis have a higher fatality rate, of 65.9%, following treatment, compared with a fatality rate of 6.5% for right-sided infective endocarditis after treatment. It has also been reported that surgical treatment has a slightly increased mortality for right-sided infective endocarditis [10]. However, it has been recommended that patients with left-sided
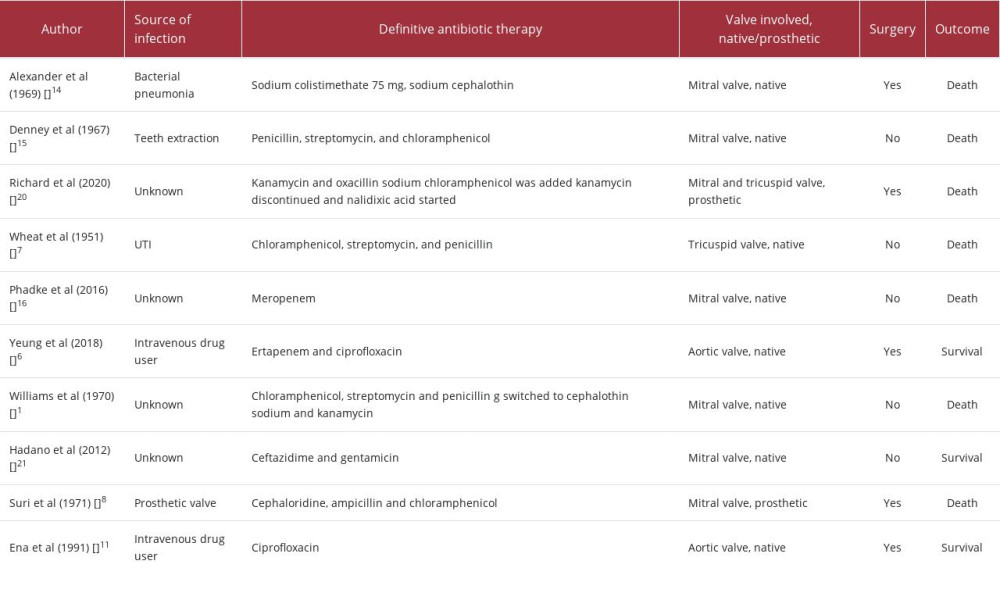
As shown in Table 1, a selection of 11 case reports of infective endocarditis caused by
The second case shows a patient who underwent multiple teeth extractions, leading to endocarditis involving the mitral valve. She was treated with a combination of 3 antibiotics, chloramphenicol, streptomycin, and penicillin, and the outcome was the same as the previous case, sepsis and death. The third case involved treatment with 4 different antibiotics for a case of bilateral vegetation endocarditis in the mitral and tricuspid valves. Although the strain was sensitive to all of the antimicrobial agents used, the patient’s condition deteriorated and resulted in death. The last case showed successful treatment of endocarditis caused by a strain of
Eight out of the 12 cases mentioned below resulted in patient death. Half of the cases had vegetations on the mitral valve only, and 1 of them involved both the tricuspid and mitral valves, while 2 cases involved the aortic valve. First-generation cephalosporins were used in 3 cases; penicillin and chloramphenicol were the most used antibiotics. Aminoglycosides were also commonly used. In our 2 cases, the choice of antibiotic treatment was made according to sensitivity and was consistent with previous reported studies.
Another report of a case of mitral valve infective endocarditis caused by teeth extraction was treated with penicillin, streptomycin, and chloramphenicol; however, the outcome was septicemia and death [15]. Another case of mitral valve endocarditis was treated only with meropenem and resulted in death due to brain herniation [16]. Another report described treatment of a case of
Recurrent
Although very rare, treatment of recurrent
It can be concluded that most cases with negative cultures have included cephalosporins and gentamicin in the treatment regimen; therefore, these agents have mostly promising outcomes in the management of infective endocarditis caused by
It has been reported in the literature that prosthetic valve infective endocarditis is mostly caused by staphylococci, which makes vancomycin an essential agent in the treatment of these patients, as was seen in the cases in this report [18]. Intravenous drug use is one of the common causes of recurrent infective endocarditis, as seen in a case of a man with 3 infections within 7 months; social support, compliance with treatment, and abstaining from i.v. drug use are essential for avoiding recurrence and for successful recovery [19].
Conclusions
This case series reinforces that patients who previously had infective endocarditis are at higher risk of recurrence, leading to higher morbidity and mortality; thus, they should be followed up more frequently, especially when it comes to highly resistant organisms, such as
Figures
References:
1.. Williams JC, Johnson JE: Arch Intern Med, 1970; 125(6); 1038-40
2.. Hejazi A, Falkiner FR: J Med Microbiol, 1997; 46(11); 903-12
3.. Khanna A, Khanna M, Aggarwal A: J Clin Diagn Res, 2013; 7(2); 243
4.. Cristina ML, Sartini M, Spagnolo AM: Int J Environ Res Public Health, 2019; 16(4); 610
5.. Morpeth S, Murdoch D, Cabell CH, Non-HACEK gram-negative bacillus endocarditis: Ann Intern Med, 2007; 147(12); 829-35
6.. Yeung HM, Chavarria B, Shahsavari D: Case Rep Infect Dis, 2018; 2018; 5903589
7.. Wheat RP, Zuckerman A, Rantz LA, Infection due to chromobacteria; Report of 11 cases: AMA Arch Intern Med, 1951; 88(4); 461-66
8.. Suri RK, Selby DA, Hawks GH, Baker CB: Can Med Assoc J, 1971; 104(11); 1013
9.. Mahlen SD, Serratia infections: From military experiments to current practice: Clin Microbiol Rev, 2011; 24(4); 755-91
10.. Cohen PS, Maguire JH, Weinstein L, Infective endocarditis caused by gram-negative bacteria: A review of the literature, 1945–1977: Prog Cardiovasc Dis, 1980; 22(4); 205-42
11.. Ena J, Amador C, Parras F, Bouza E, Ciprofloxacin as an effective antibacterial agent in serratia endocarditis: J Infect, 1991; 22(1); 103-5
12.. Mills J, Drew D: Ann Intern Med, 1976; 84(1); 29-35
13.. Baddour LM, Wilson WR, Bayer AS, Infective endocarditis in adults: Diagnosis, antimicrobial therapy, and management of complications: Circulation, 2015; 132(15); 1435-86
14.. Alexander RH, Reichenbach DD, Merendino KA: Arch Surg, 1969; 98(3); 287-91
15.. Denney JD, Kaye D, Hagstrom JWC: N Engl J Med, 2010; 276(24); 1362
16.. Phadke VK, Jacob JT: Infect Dis Clin Pract (Baltim Md), 2016; 24(3); 143
17.. Poyet R, Kerebel S, Pons F, [Recurrent infective endocarditis. A case report.]: Ann Cardiol Angeiol (Paris), 2010; 59(1); 44-47 [in French]
18.. Antunes MJ, Sanches MF, Fernandes LE, Antibiotic prophylaxis and prosthetic valve endocarditis: J Heart Valve Dis, 1992; 1(2); 201-5
19.. Cannon JW, Awori Hayanga JW, Drvar TB, A 34-year-old male intravenous drug user with a third episode of tricuspid valve endocarditis treated with repeat valve surgery: Am J Case Rep, 2021; 22(1); e927385
20.. Towbin JA, McKenna WJ, Abrams DJ, 2019 HRS expert consensus statement on evaluation, risk stratification, and management of arrhythmogenic cardiomyopathy: Heart Rhythm, 2019; 16(11); e301-e72
21.. Hadano Y, Kamiya T, Uenishi N: Intern Med, 2012; 51(11); 1425-28
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report  22,760,204
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133