11 November 2023: Articles 
Two Cases of Degenerative Cervical Spondylotic Myelopathy in Adults with Athetoid and Dystonic Cerebral Palsy
Rare disease
Hayato Kinoshita1ABE*, Michio Hongo1CDG, Yuji Kasukawa1BDF, Daisuke Kudo1CEG, Ryota KimuraDOI: 10.12659/AJCR.941158
Am J Case Rep 2023; 24:e941158






Abstract
BACKGROUND: Patients with athetoid and dystonic cerebral palsy (ADCP) may develop degenerative changes in the cervical spine that can aggravate their neurological symptoms in adulthood. This report is of 2 cases of ADCP associated with degenerative cervical spondylotic myelopathy in a 39-year-old woman and a 52-year-old man, requiring different surgical treatments.
CASE REPORT: Case 1. The patient was a 39-year-old woman who had fallen down 7 years before surgery and had since been walking with a cane. Her gait disturbance had worsened in the 2 years prior to surgery, and numbness in her upper limbs appeared. In the year before surgery, spasticity and numbness in the lower limbs worsened, and fine motor impairment also appeared. Because of mild involuntary movements of the neck, cervical laminoplasty from C3 to C6 was performed, and her symptoms remained stable until the last follow-up 4.5 years after surgery. Case 2. The patient was a 52-year-old man who had fallen down 7 years before surgery, resulting in transient limb weakness. In the year before surgery, he had developed fine motor impairment. He subsequently developed gait disturbance and requested cervical surgery. Because of involuntary movements involving the neck and trunk, he underwent cervical posterior fusion from C2 to T1. Six months after surgery, the gait disturbance had improved.
CONCLUSIONS: This report describes 2 adults with a history of ADCP since birth and highlights that degenerative changes of the cervical spine can occur at a relatively early age in adulthood, requiring an individualized approach to management.
Keywords: Athetosis, Cerebral Palsy, Cervical Vertebrae, Male, Female, Humans, Adult, Middle Aged, Hypesthesia, Spinal Cord Diseases, Dyskinesias
Background
Cerebral palsy (CP), which occurs in 1.5 to 2.5 per 1000 live births, is a group of non-progressive, permanent disorders. CP develops from insults during fetal development or insults in the infant’s brain that cause limitation of activity by affecting the developing motor control circuit [1]. The most common subtype of CP is the spastic type, followed by the dyskinetic or athetoid type [2].
Athetoid and dystonic cerebral palsy (ADCP) is a clinical diagnosis taking into account patient history, such as perinatal asphyxia and severe hyperbilirubinemia, and family history, including other neurological diseases and movement disorders [3]. The presence of lesions in the basal ganglia and thalamus on brain magnetic resonance imaging (MRI) can also aid in the diagnosis [4].
Patients with ADCP often show a slow, irregular, torsional, and persistent involuntary movement induced or worsened by emotions, stress, and illness [4]. Treatment of ADCP focuses on the management of symptoms and improvement in the quality of life for the patient [5]. One specific treatment is medication, such as GABA-B agonists and trihexyphenidyl, but these are reportedly less effective [6,7]. Other treatments include deep brain stimulation and injection of botulinum toxin, which have been reported to have some efficacy [8,9]. The prognosis for patients with ADCP is generally reported to be poor, with early deaths due to aspiration and pneumonia [1].
As one of the complications of ADCP, involuntary neck movements induced by ADCP can cause spinal canal stenosis with cervical spondylotic myelopathy (CSM), resulting in fine motor impairment and gait disturbance in young patients [10,11].
Approximately 31% of patients with ADCP develop CSM [12]. Because of persistent involuntary neck movements, postoperative outcomes are generally worse in patients with than without CP. In some reports, the incidence of postoperative complications in patients with CP has been 36% to 39% [13,14], whereas in patients without CP it has been 9% to 30% [15–18].
We herein describe 2 patients with ADCP who developed CSM, and present a literature review.
Case Reports
CASE 1:
A 39-year-old woman presented for evaluation of numbness in the limbs, fine motor impairment, and gait disturbance. She had fallen down 7 years before surgery and had since been walking with a cane. Her gait disturbance had worsened over the 2 years before surgery, and numbness in her upper limbs had also appeared. Since 1 year before surgery, spasticity and numbness in the lower limbs had worsened and fine motor impairment had also appeared. She was then referred to our hospital by her family doctor for surgery. Her medical history included CP and developmental dysplasia of the left hip, which had been surgically treated twice. She had grade 1 athetosis according to the classification established by Mihara et al [19]. Physical examination revealed hyperreflexia of deep tendon reflexes in the upper and lower limbs. Manual muscle testing showed predominantly right-sided weakness (right deltoid: fair level; tibialis anterior: poor level). The Japanese Orthopaedic Association (JOA) score was 6.5 out of 17 points. Radiography showed cervical deformity. MRI showed C4/5 spinal cord signal changes, but the degree of stenosis was mild, suggesting that dynamic factors were largely involved (Figure 1). The patient underwent C3–C6 laminoplasty. At the time of discharge, the numbness in her limbs was mildly relieved, and her mobility improved from full wheelchair assistance to partial assistance. Four months after surgery, the C4 and C5 spacers were dislocated; however, because her symptoms had not worsened, no additional surgery was performed. At the final follow-up 4.5 years after surgery, the limb numbness had not worsened and the JOA score was 7.5 (Figure 2).
CASE 2:
A 52-year-old man presented with numbness in the limbs, fine motor impairment, and gait disturbance. He had fallen down 7 years before surgery, resulting in transient limb weakness. One year before surgery, he had developed fine motor impairment. He subsequently developed gait disturbance and requested cervical surgery. He had CP with grade 3 athetosis, as classified by Mihara et al [19]. Physical examination revealed hyperreflexia of deep tendon reflexes in the upper and lower limbs. Manual muscle testing showed predominantly right-sided weakness (right deltoid, triceps, and finger abduction: fair level). The JOA score was 7. Radiography showed lower cervical deformity. MRI showed spinal canal stenosis from C3/4 to C6/7 in the axial view and intramedullary signal changes from C2/3 to C6/7 in the sagittal view (Figure 3). The patient underwent C2-T1 posterior fixation, C3 laminectomy, and C4–C6 laminoplasty. The bilaterally opened lamina was fixed to cobalt-chrome rods on each side using nonabsorbable thread. The rods were molded with minimal bending using a computer-assisted rod-bending system. Bone fragments were grafted over the cervical facets (Figure 4). The patient’s limb numbness improved, and his mobility also improved from full wheelchair assistance to partial assistance by the time he was discharged. He developed postoperative right upper limb paralysis, but this showed a tendency to improve in the third postoperative month. At 6 months after surgery, the patient was able to hold the upright position for a short time, and radiological findings showed no implant problems. His JOA score was 9 (Figure 4).
Discussion
The main indication of cervical spondylosis is age-related degeneration of the intervertebral disc and cervical spinal elements. Degenerative changes, such as facet joints, posterior longitudinal ligament, or ligamentum flavum, cause stenosis of the spinal canal and intervertebral foramina. The diagnosis of CSM is conducted by the total assessment of physical findings (including pathological hyper- or hyporeflexia of tendon reflexes, hand weakness, clumsiness, gait instability, and sometimes urinary symptoms) and imaging evaluation, such as whether MRI images show spinal cord compression lesions or spinal cord signal changes [20].
Common treatment options for CSM include conservative and surgical therapy. Conservative treatment consists of physical therapy, including isometric and resistance exercises to strengthen the neck and upper back muscles, medications (nonsteroidal anti-inflammatory drugs, oral steroids, muscle relaxants, anticonvulsants, antidepressants, and sometimes opioid analgesics), and a soft cervical collar. A surgical approach should be selected for severe or progressive cervical myelopathy [21].
Jameson et al [22] reviewed 7 patients with ADCP complicated by CSM. They mentioned that, because the initial presentation was insidious and symptoms were only latterly detected, surgical treatment was often delayed. In our 2 cases, we were aware of the CSM 7 years before the surgery, but the patients did not initially want to undergo surgery. Therefore, a delay in diagnosis does not apply to these cases, although the timing of the surgery may have been late.
In patients who have CSM with ADCP, conservative treatments are generally ineffective and surgery is often required [23]. However, the surgical outcomes tend to be worse in these patients than in patients without CP because they are more prone to implant failures and recurrence of spinal canal stenosis caused by persistent involuntary movements.
Kim et al [23] compared the postoperative outcomes and complications of 35 patients with CP and 35 without CP. Motor weakness, adjacent segment disease, time-related neurological deteriorations, and the revision rate were significantly higher in patients with CP than in those without CP. Furthermore, they divided the patients with CP into those with and without complications and found that the incidence of fixed cervical deformities was significantly higher in patients with complications. No significant differences were found in complications related to the type of CP, such as dyskinetic/athetoid, spastic/diplegic, or mixed [23].
In the present study, the patient in case 1 had fixed cervical deformity and showed dislocation of the spacers. Despite the position of the spacers, she developed no neurological deterioration for 4.5 years after surgery. The patient in case 2 showed postoperative motor weakness of the upper limb. Fortunately, his upper limb paralysis slowly improved. Further follow-up of case 1 is required to ensure that complications such as rod breakage, screw loosening, adjacent segment disease, or neurological deteriorations do not occur in the future. Various reports have described the results of different surgical procedures, such as posterior, anterior, or combined posterior and anterior approaches [4,24,25]. Watanabe et al [25] reported the surgical outcomes of CSM in patients with ADCP. The revision rate of posterior fixation and combined anterior and posterior fixation were almost equal (22% vs 25%, respectively). The reason for all revisions was screw loosening.
Instrumentation was employed in only 1 of our 2 patients. No short-term complications occurred in this patient; however, further follow-up is necessary. Jameson et al [22] presented the postoperative CSM results of 7 ADCP patients with JOA scores, all of whom had some posterior or anterior fixations. Their JOA scores showed an improvement of 0.5 to 2.5 points compared with preoperative scores. By contrast, our 2 patients showed an improvement of 1.0 to 2.0 points. Both results might even out in the short term.
Various methods have been devised to inhibit involuntary movements in patients with ADCP, such as orthopedic selective spasticity-control surgery or injection of botulinum toxin into the sternocleidomastoid muscle [26–28]. Postoperative rest with braces can also be provided. These additional peri-operative methods can contribute to better postoperative outcomes for patients who have ADCP with CSM, but they are still uncommonly performed, and the optimal period of postoperative immobilization using braces has not been established. Further research is necessary. Our patients underwent neither orthopedic selective spasticity-control surgery nor injection of botulinum toxin. The patient in case 1 used a neck collar for 2 months. Longer-term or more extensive immobilization might have been needed because of dislocation of the spacers. The patient in case 2 used a sternal occipital mandibular immobilization brace for the first 6 months after surgery, and remained well without implant failure or a skin problem.
In this report, we mainly discuss the possibility of preoperative evaluation with a classification of athetosis specific to cervical spine lesions, which could allow selection of surgical methods according to the degree of classification. There are some assessment tools designed to help measure the severity of dystonia, such as the Barry-Albright Dystonia Rating Scale, Burke-Fahn-Marsden Dystonia Rating Scale, and Dyskinesia Impairment Scale. However, these tools have the disadvantage of being complex and difficult to measure. In addition, they do not directly lead to treatment decisions for cervical spine disease in patients with ADCP [29].
Mihara et al [19] considered athetosis motor strength to be a contributing factor to the difficulty of cervical spine surgery in patients with ADCP, and classified the athetosis intensity from grade 1 to grade 5 (Table 1). Initially, they defined difficult-to-control head and neck involuntary movements by external fixation with a halo vest as grade ≥4 or above. In our study, the patient in case 1 had grade 1 athetosis and that in case 2 had grade 3. Because patient 2 had developed no postoperative implant problems by 6 months, external fixation using the sternal occipital mandibular immobilization brace in this patient was considered effective for postoperative cervical immobilization.
Kuroki et al [30] stated that it is important to evaluate athetosis intensity preoperatively and to select a surgical technique according to that intensity. Our patient in case 1 underwent laminoplasty and developed no postoperative complications requiring reoperation. This might have been due to the grade 1 athetosis, although this patient still developed dislocation of 2 spacers. Therefore, fixation techniques appear to be essential for patients who have ADCP with CSM.
Surgeons should be aware of various limitations in the use of fixation techniques, one of which is rod weakness caused by bending of the rod during installation. Kim et al [31] researched the mechanical strength of rods with 3 different bending methods: French single bending, multiple bending, and in situ bending. They concluded that French single bending has the highest risk of rod breakage. One disadvantage is that the cervical spine of patients with ADCP is often deformed, and multiple rod bending using a French bender is often required during rod installation. In case 2, we used a computer-assisted rod-bending system, which minimized the number of bending operations and maintained the strength of the rod. Furthermore, we did not use a spacer at the portion of laminoplasty; the split laminae were simply tied to the rods on both sides with thread to avoid spinal cord compression when the spacers dislocated. Nevertheless, these measures might not avoid proximal junctional failure, screw loosening, or worsening of neurological findings. Thus, we plan to continue carefully monitoring the patient’s progress.
Conclusions
This report has described 2 adults with a history of ADCP since birth and has highlighted that degenerative changes of the cervical spine can occur at a relatively early age in adulthood, requiring an individualized approach to management.
Figures
References:
1.. Hallman-Cooper JL, Rocha Cabrero F: Cerebral palsy, 2022, Treasure Island (FL), StatPearls Publishing
2.. Michael-Asalu A, Taylor G, Campbell H, Cerebral palsy: Diagnosis, epidemiology, genetics, and clinical update: Adv Pediatr, 2019; 66; 189-208
3.. Monbaliu E, Himmelmann K, Lin JP, Clinical presentation and management of dyskinetic cerebral palsy: Lancet Neurol, 2017; 16(9); 741-49
4.. Zhou H, Liu ZJ, Wang SB, Laminoplasty with lateral mass screw fixation for cervical spondylotic myelopathy in patients with athetoid cerebral palsy: A retrospective study: Medicine (Baltimore), 2016; 95(39); e5033
5.. Novak I, Morgan C, Adde L, Early, accurate diagnosis and early intervention in cerebral palsy: Advances in diagnosis and treatment: JAMA Pediatr, 2017; 171(9); 897-907
6.. Lumsden DE, Kaminska M, Tomlin S, Lin JP, Medication use in childhood dystonia: Eur J Paediatr Neurol, 2016; 20(4); 625-29
7.. Rice J, Waugh MC, Pilot study on trihexyphenidyl in the treatment of dystonia in children with cerebral palsy: J Child Neurol, 2009; 24(2); 176-82
8.. Gimeno H, Lin JP, The International Classification of Functioning (ICF) to evaluate deep brain stimulation neuromodulation in childhood dystoniahyperkinesia informs future clinical & research priorities in a multidisciplinary model of care: Eur J Paediatr Neurol, 2017; 21(1); 147-67
9.. Lundy CT, Doherty GM, Fairhurst CB, Botulinum toxin type A injections can be an effective treatment for pain in children with hip spasms and cerebral palsy: Dev Med Child Neurol, 2009; 51(9); 705-10
10.. Anderson WW, Wise BL, Itabashi HH, Jones M, Cervical spondylosis in patients with athetosis: Neurology, 1962; 12; 410-12
11.. Hirose G, Kadoya S, Cervical spondylotic radiculo-myelopathy in patients with athetoid-dystonic cerebral palsy: Clinical evaluation and surgical treatment: J Neurol Neurosurg Psychiatry, 1984; 47(8); 775-80
12.. Guettard E, Ricard D, Roze E, Risk factors for spinal cord lesions in dys-tonic cerebral palsy and generalised dystonia: J Neurol Neurosurg Psychiatry, 2012; 83(2); 159-63
13.. Yaszay B, Bartley CE, Sponseller PD, Major complications following surgical correction of spine deformity in 257 patients with cerebral palsy: Spine Deform, 2020; 8(6); 1305-12
14.. Samdani AF, Belin EJ, Bennett JT, Major perioperative complications after spine surgery in patients with cerebral palsy: assessment of risk factors: Eur Spine J, 2016; 25(3); 795-800
15.. Master DL, Son-Hing JP, Poe-Kochert C, Armstrong DG, Thompson GH, Risk factors for major complications after surgery for neuromuscular scoliosis: Spine (Phila Pa 1976), 2011; 36(7); 564-71
16.. Sharma S, Wu C, Andersen T, Prevalence of complications in neuro-muscular scoliosis surgery: A literature meta-analysis from the past 15 years: Eur Spine J, 2013; 22(6); 1230-49
17.. Rumalla K, Yarbrough CK, Pugely AJ, Spinal fusion for pediatric neuromuscular scoliosis: national trends, complications, and in-hospital outcomes: J Neurosurg Spine, 2016; 25(4); 500-8
18.. Wewel JT, Brahimaj BC, Kasliwal MK, Traynelis VC, Perioperative complications with multilevel anterior and posterior cervical decompression and fusion: J Neurosurg Spine; 2019 [Online ahead of print]
19.. Mihara H, Kondo S, Kohno M, [Clinical analysis of reoperation following surgical treatments for cervical spondylotic myelopathy accompanied with athetoid cerebral palsy]: Rinshoseikeigeka (Clinical Orthopaedic Surgery), 2008; 43(5); 465-72 [in Japanese]
20.. McCormick WE, Steinmetz MP, Benzel EC, Cervical spondylotic myelopathy: Make the difficult diagnosis, then refer for surgery: Cleve Clin J Med, 2003; 70(10); 899-904
21.. Rao RD, Currier BL, Albert TJ, Degenerative cervical spondylosis: Clinical syndromes, pathogenesis, and management: J Bone Joint Surg Am, 2007; 89(6); 1360-78
22.. Jameson R, Rech C, Garreau de Loubresse C, Cervical myelopathy in athetoid and dystonic cerebral palsy: retrospective study and literature review: Eur Spine J, 2010; 19(5); 706-12
23.. Kim HC, Jeon H, Jeong YH, Factors affecting postoperative complications and outcomes of cervical spondylotic myelopathy with cerebral palsy: A retrospective analysis: J Korean Neurosurg Soc, 2021; 64(5); 808-17
24.. Okamoto T, Neo M, Fujibayashi S, Mechanical implant failure in posterior cervical spine fusion: Eur Spine J, 2012; 21(2); 328-34
25.. Watanabe K, Otani K, Nikaido T, Surgical outcomes of cervical myelopathy in patients with athetoid cerebral palsy: A 5-year follow-up: Asian Spine J, 2017; 11(6); 928-34
26.. Matsuo T: [Cerebral palsy: Spasticity-control and orthopaedics: An introduction to orthopaedic selective spasticity-control surgery (OSSCS).], 2002, Tokyo (JPN), Sofusha [in Japanese]
27.. Sharma A, Vats S, Chahal A, Physical exercises in combination with botulinum toxin in treating children with cerebral palsy: A literature review: J Lifestyle Med, 2022; 12(3); 138-47
28.. Traynelis VC, Rodnitzky RL, Menezes AH, Botulinum toxin enhancement of postoperative immobilization in patients with cervical dystonia: J Neurosurg, 1992; 77(5); 808-9
29.. Monbaliu E, Ortibus E, De Cat J, The Dyskinesia Impairment Scale: A new instrument to measure dystonia and choreoathetosis in dyskinetic cerebral palsy: Dev Med Child Neurol, 2012; 54(3); 278-83
30.. Kuroki H, Hamanaka H, Inomata N, Clinical results of surgical treatment for cervical myelopathy in patients with athetoid cerebral palsy: J. Spine Res, 2011; 2(10); 1572-77
31.. Kim KD, Panchal R, Moldavsky M, Effects of pre-contoured and in situ contoured rods on the mechanical strength and durability of posterior cervical instrumentation: A finite-element analysis and scanning electron microscopy investigation: Spine Deform, 2020; 8(4); 569-76
Figures
Tables
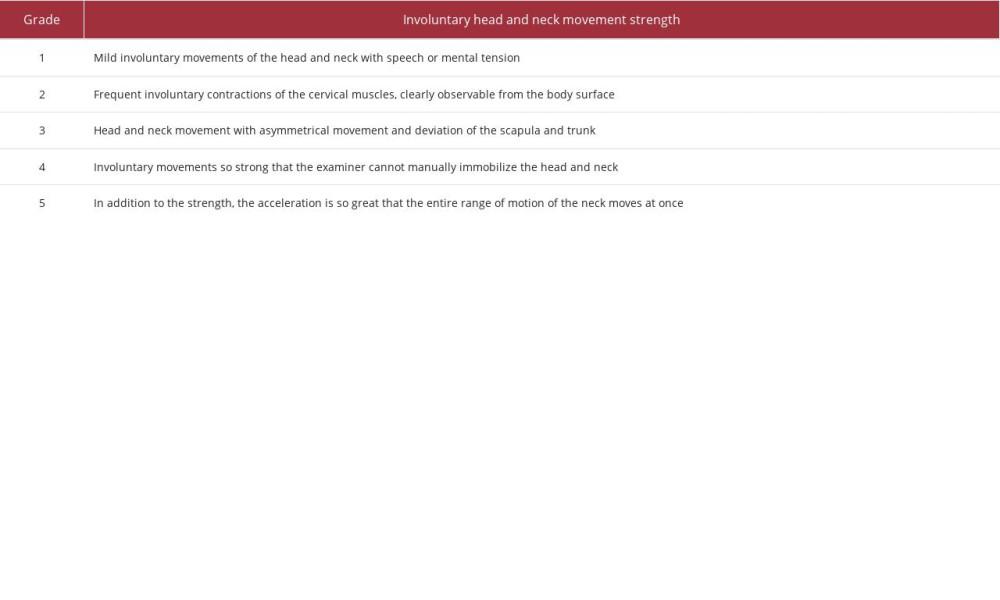 Table 1.. Classification of athetosis intensity.Mihara’s classification of athetosis intensity. The classification is a 5-point scale from grade 1 to grade 5. The higher the number, the stronger the athetosis intensity.Table 1.. Classification of athetosis intensity.Mihara’s classification of athetosis intensity. The classification is a 5-point scale from grade 1 to grade 5. The higher the number, the stronger the athetosis intensity.
Table 1.. Classification of athetosis intensity.Mihara’s classification of athetosis intensity. The classification is a 5-point scale from grade 1 to grade 5. The higher the number, the stronger the athetosis intensity.Table 1.. Classification of athetosis intensity.Mihara’s classification of athetosis intensity. The classification is a 5-point scale from grade 1 to grade 5. The higher the number, the stronger the athetosis intensity. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133