09 February 2024: Articles 
Recurrent Var. Bacteremia and Review of the Literature on : The First Case Report
Challenging differential diagnosis, Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents, Rare disease
Kazuhiro IshikawaDOI: 10.12659/AJCR.942553
Am J Case Rep 2024; 25:e942553






Abstract
BACKGROUND: Fermented foods, such as yogurt, are often considered healthy; however, there have been numerous reported cases of bacteremia associated with their consumption. In this report, we present a case of Bacillus subtilis var. natto (B. subtilis var. natto) bacteremia related to the consumption of natto, a traditional Japanese food made from fermented soybeans. We also conducted a literature review on B. subtilis bacteremia.
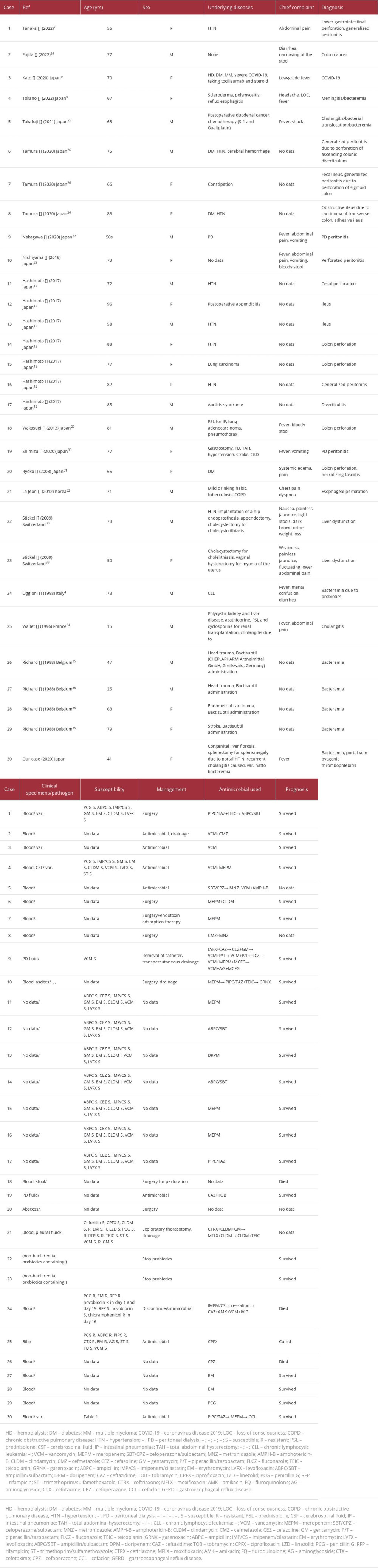
CASE REPORT: We report the case of a 41-year-old woman who presented with fever, had a medical history of congenital liver fibrosis, and experienced recurrent B. subtilis var. natto bacteremia along with acute cholangitis. Although she discontinued eating natto, she developed pyogenic thrombophlebitis due to B. subtilis var. natto. We successfully treated her with meropenem and an anti-coagulant. To investigate the management and prognosis of B. subtilis var. natto bacteremia, we conducted a literature review of B. subtilis intra-abdominal infection. We identified 17 papers describing 30 cases of B. subtilis intra-abdominal infection, 4 cases of which were caused by B. subtilis var. natto; the median age of the patients was 71 years (range, 15-96 years), 14 patients (47%) were female, and 3 patients (10%) died. From our findings, our case was the only one of recurrent B. subtilis var. natto infection. Even after patients discontinue eating natto, they should be carefully monitored.
CONCLUSIONS: Due to advancements in PCR identification techniques, case reports of infections caused by B. subtilis var. natto are increasing.
Keywords: Bacillus subtilis, Bacteremia, Gastrointestinal Diseases, Probiotics, Humans, Female, Adolescent, young adult, adult, Middle Aged, Aged, Aged, 80 and over, Male, Soy Foods, Intraabdominal Infections
Background
Some fermented foods, such as natto and yogurt, are considered healthy, but some cases of
Case Report
A 41-year-old Japanese woman presenting with fever was admitted to St Luke’s International Hospital. One month before admission, she developed portal vein pyogenic thrombophlebitis. She was treated with amoxicillin/clavulanate, levofloxacin, and rivaroxaban. However, 1 week before admission, her antimicrobials were discontinued due to antibiotic-related diarrhea. She was admitted to St Luke’s International Hospital for recurrent portal vein pyogenic thrombophlebitis. Our patient had congenital liver fibrosis and splenomegaly due to portal hypertension status post-splenectomy and had a history of acute suppurative cholangitis caused by
The fever resolved, and the clinical findings improved. Thus, the patient’s antibiotic was switched back to cefaclor 500 mg 3 times daily, and she was discharged on day 11. Nine months after discharge, her clinical status was stable, and the portal vein thrombus disappeared while she was on prophylactic cefaclor (Figure 1).
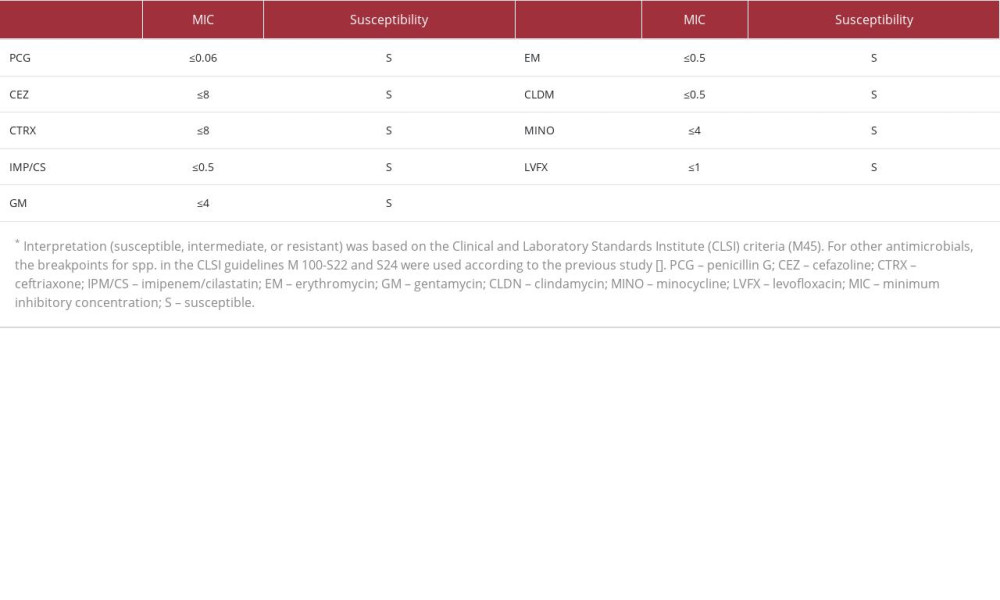
The specific strain of
Discussion
We encountered a case of recurrent
We performed a search using the keywords “
In this review,
Our way of identifying the
There have been reports of bacteremia related to
Congenital liver fibrosis is characterized by bile duct dysplasia due to defective ductal plate formation during the embryonic period of bile duct formation and fibrosis in the region of the hepatic portal vein. The main symptoms of congenital liver fibrosis are splenomegaly due to portal hypertension, rupture of esophageal varices, and recurrent cholangitis [12].
Bacterial translocation is a phenomenon in which bacteria penetrate the intestinal epithelium and invade other organs by hematologic or lymphatic spread. Bacteria that invade the blood vessels of the intestinal tract reach the liver through the portal vein, whereas those that invade lymphatically reach the mesenteric lymph nodes [13,14]. The risks of bacterial trans-location include intestinal disease, neutropenia, immunosuppression, low nutrition, prolonged transvenous nutritional management, high levels of stress, and portal hypertension [15,16]. Therefore, the mechanism of bacteremia caused by
Furthermore, portal vein pyogenic thrombophlebitis is a rare but serious complication of intra-abdominal infection and has been previously reported as a complication of appendicitis [17], but in recent years, reports of its secondary occurrence in diverticulitis, inflammatory bowel disease, and cholangitis have increased [18,19]. Cirrhosis and portal hypertension are also risks for portal vein thrombosis [20]. Therefore, our case had several risk factors for portal vein thrombosis.
In our case, the patient had completely stopped eating natto and was on long-term suppression with cefaclor, but she relapsed after discontinuing cefaclor. We could not determine the cause of the relapse, but we considered that
There is little evidence for the effectiveness of anticoagulation for portal vein pyogenic thrombosis. Some observational studies have shown that the use of anticoagulation led to rapid dissolution of the portal vein thrombus, with no risk of bleeding [22], but no randomized trials or other studies have been performed. In the present case, we used rivaroxaban because of the low likelihood of spontaneous dissolution with antimicrobials alone. The patient did not experience bleeding, and complete resolution of the thrombus in the portal vein was confirmed on follow-up.
Conclusions
We reported a case of recurrent
Due to advancements in PCR identification techniques, case reports of infections caused by
Figures
References:
1.. Haghighat L, Crum-Cianflone NF: Int J STD AIDS, 2016; 27; 1223-30
2.. Haziri D, Prechter F, Stallmach A, Yoghurt-induced Lactobacillus bacteremia in a patient with Crohn’s disease on therapy with ustekinumab and concomitant HIV-infection: Z Gastroenterol, 2021; 59; 317-20
3.. Nishito Y, Osana Y, Hachiya T: BMC Genomics, 2010; 11; 243
4.. Oggioni MR, Pozzi G, Valensin PE: J Clin Microbiol, 1998; 36; 325-26
5.. Weber DJ, Saviteer SM, Rutala WA, Thomann CA, Clinical significance of Bacillus species isolated from blood cultures: South Med J, 1989; 82; 705-9
6.. Tokano M, Tarumoto N, Imai K: Intern Med; 202362(13); 1989-93
7.. Tanaka I, Kutsuna S, Ohkusu M: Emerg Infect Dis, 2022; 28; 1718-19
8.. Tam NK, Uyen NQ, Hong HA: J Bacteriol, 2006; 188; 2692-700
9.. Kato A, Yoshifuji A, Komori K: J Infect Chemother, 2022; 28; 1212-15
10.. Sumi H, Hamada H, Tsushima H, A novel fibrinolytic enzyme (nattokinase) in the vegetable cheese natto; A typical and popular soybean food in the Japanese diet: Experientia, 1987; 43; 1110-11
11.. Hashimoto T, Hayakawa K, Mezaki K: Kansenshogaku Zasshi, 2017; 91; 151-54
12.. Hasbaoui BE, Rifai Z, Saghir S, Congenital hepatic fibrosis: Case report and review of literature: Pan Afr Med J, 2021; 38; 188
13.. Alexander JW, Boyce ST, Babcock GF, The process of microbial trans-location: Ann Surg, 1990; 212; 496-510 ; discussion 511–12
14.. Takeuchi A: Am J Pathol, 1967; 50; 109-36
15.. Vaishnavi C, Translocation of gut flora and its role in sepsis: Indian J Med Microbiol, 2013; 31; 334-42
16.. Cohen SA, Woodfield MC, Boyle N, Incidence and outcomes of bloodstream infections among hematopoietic cell transplant recipients from species commonly reported to be in over-the-counter probiotic formulations: Transpl Infect Dis, 2016; 18; 699-705
17.. Soro Y, Pylephlebitis and liver abscesses due to appendicitis: J Int Coll Surg, 1948; 11; 464-68
18.. Kanellopoulou T, Alexopoulou A, Theodossiades G, Pylephlebitis: An overview of non-cirrhotic cases and factors related to outcome: Scand J Infect Dis, 2010; 42; 804-11
19.. Plemmons RM, Dooley DP, Longfield RN, Septic thrombophlebitis of the portal vein (pylephlebitis): Diagnosis and management in the modern era: Clin Infect Dis, 1995; 21; 1114-20
20.. Intagliata NM, Caldwell SH, Tripodi A, Diagnosis, development, and treatment of portal vein thrombosis in patients with and without cirrhosis: Gastroenterology, 2019; 156; 1582-99 e1
21.. Drobniewski FA, Bacillus cereus and related species: Clin Microbiol Rev, 1993; 6; 324-38
22.. Naymagon L, Tremblay D, Schiano T, Mascarenhas J, The role of anticoagulation in pylephlebitis: A retrospective examination of characteristics and outcomes: J Thromb Thrombolysis, 2020; 49; 325-31
23.. Luna VA: J Antimicrob Chemother, 2007; 60(3); 555-67
24.. Fujita K: The 678th: P.23 Kanto Regional Meeting of the Japanese Society of Internal Medicine, 2022 [in Japanese].
25.. Takafuji Y: J Abdom Emerg Med, 2021; 41; 228 [in Japanese]
26.. Tamura T: J Jpn Soc Surg Infect, 2020; 17; 456 [in Japanese]
27.. Nakagawa Y: Kidney Dial, 2020; 89; 248-49 [in Japanese]
28.. Nishiyama N, [A case of Bacillus subtilis bacteremia and intra-abdominal abscess due to perforated peritonitis.]: J Jpn Soc Surg Infect, 2016; 13; 593 [in Japanese]
29.. Wakasugi T: Niigata Med J, 2013; 127; 389 [in Japanese]
30.. Shimizu Y, [Introduction experience in introducing peritoneal dialysis to patients with gastrostomy.]: Kidney Dial, 2010; 69; 273-75 [in Japanese]
31.. Kyan R, [A case of extensive necrotizing fasciitis caused by retroperitoneal abscess from intestinal perforation spreading to the left side of the abdomen and lower leg.]: Acute Med Surg, 2003; 14; 657 [in Japanese]
32.. La Jeon Y, Yang JJ, Kim MJ: J Med Microbiol, 2012; 61; 1766-69
33.. Stickel F, Droz S, Patsenker E: J Hepatol, 2009; 50; 111-17
34.. Wallet F, Crunelle V, Roussel-Delvallez M: Am J Gastroenterol, 1996; 91; 1477-78
35.. Richard V, Van der Auwera P: Eur J Clin Microbiol Infect Dis, 1988; 7; 783-85
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,422
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133