05 February 2024: Articles 
Pharmacogenetic Analysis of an 8-Year Old Girl with Reye Syndrome Associated with Use of Naproxen
Challenging differential diagnosis, Diagnostic / therapeutic accidents, Management of emergency care, Unexpected drug reaction, Rare disease, Clinical situation which can not be reproduced for ethical reasons
Byungwook KimDOI: 10.12659/AJCR.942242
Am J Case Rep 2024; 25:e942242






Abstract
BACKGROUND: Reye syndrome is a rare, yet potentially life-threatening disease characterized by acute encephalopathy and hepatic failure. This report presents the case of an 8-year-old girl with Reye syndrome and seizures after the use of naproxen.
CASE REPORT: An 8-year-old girl experienced a 3-day episode of fever and abdominal pain. After receiving naproxen (375 mg twice daily) starting from day -3, she exhibited hypotension, tonic seizure, and loss of consciousness (day 1). Physical examination and laboratory test results revealed acute kidney injury, metabolic acidosis, and elevated levels of lactate dehydrogenase (LDH), liver enzymes, and ferritin. On day 2, the maximum values of aspartate aminotransferase, alanine aminotransferase, LDH, creatinine, and ferritin were 955 U/L, 132 U/L, 8040 U/L, 2 mg/dL, and >40000 ug/L, respectively. She was given supportive care and recovered after 11 days (day 12), with normalization of kidney function and metabolic abnormalities. To identify possible genetic polymorphisms associated with the patient’s symptoms, genotypes were tested using a drug metabolizing enzymes and transporters (DMET) gene chip. Among genes involved in the metabolism of naproxen, UGT1A6 (*1/*2) and UGT2B7 (*1/*2) resulted in possibly decreased function. Other results which may have had clinical significance included homozygote results for NAT2*6/*6 (rs1799930).
CONCLUSIONS: A rare case of Reye syndrome after administration of naproxen was presented in this case. A DMET gene chip was used to screen for possible genetic polymorphisms associated with Reye syndrome, but the result was inconclusive.
Keywords: hepatic encephalopathy, Pharmacogenetics, Reye Syndrome
Background
Reye syndrome is a rare, often life-threatening disease characterized by acute hepatic failure and metabolic encephalopathy and includes symptoms of vomiting, personality changes, confusion, seizures, and loss of consciousness [1]. It is commonly observed in children and adolescents and is known to manifest shortly after the recovery from a viral infection [2]. The underlying mechanism of disease is poorly studied but can be associated with inborn error of metabolism, most commonly diagnosed with medium-chain acyl coenzyme A dehydrogenase deficiency [3]. The use of aspirin, a non-steroidal anti-inflammatory drug (NSAID), has been established as the only statistically proven cause of Reye syndrome, with 90% of cases in children known to be associated with aspirin [1,2].
Naproxen is an orally taken NSAID commonly used to treat pain, inflammatory diseases, and fever [4]. Naproxen undergoes extensive metabolism to form 6-0-desmethyl naproxen, which is primarily excreted in the urine [4]. Naproxen is a generally well-tolerated drug, and common adverse reactions include stomach pain, constipation, diarrhea, gas, heartburn, nausea, vomiting, and dizziness [5]. In this report, we present the case of an 8-year-old girl exhibiting defining characteristics of Reye syndrome and seizures that occurred in conjunction with the use of naproxen.
Case Report
An 8-year-old girl (height, 142.5 cm; weight, 34.5 kg) who experienced a 3-day episode of fever and abdominal pain was administered naproxen (375 mg twice daily) starting from day -3. Her initial temperature before the administration of naproxen was 39.8°C, which reached a maximum of 40.0°C (day -3) and gradually decreased with the use of naproxen. In the morning of day 1 (third day of naproxen administration), she experienced generalized numbness and slurred speech but remained alert. At around 6 AM, with the presence of left-sided eyeball deviation, generalized stiffness was observed, and oxygen saturation dropped to 70% during a 30-s tonic seizure. Subsequently, the patient’s mental status returned to normal briefly, but she experienced irritability and abdominal pain. Right-sided eyeball deviation was noted, along with increased rigidity. Both right-sided eyeball deviation and upper-extremity eyeball deviation persisted. Lorazepam was promptly administered, leading to the cessation of upper-extremity eyeball deviation while the patient fell asleep.
Physical examination and laboratory test results revealed acute kidney injury, metabolic acidosis, and elevated levels of lactate dehydrogenase (LDH), liver enzymes, and ferritin (Table 1). After the development of neurologic symptoms, including tonic seizure and loss of consciousness on day 1, naproxen administration was discontinued. Serum levels of aspartate aminotransferase (AST), alanine aminotransferase (ALT), LDH, creatinine, and ferritin reached maximum values on day 2, with values of 955 U/L, 132 U/L, 8040 U/L, 2 mg/ dL, and >40000 ug/L, respectively. The patient also presented mild hyperammonemia, with a maximum value of 93 ug/dL ammonia on day 1, which gradually recovered over the course of 7 days (Table 1). Electroencephalography was conducted at days 1, 4, and 7, and results were indicative of diffuse cerebral dysfunction, with diffuse high-amplitude delta activity and intermittent diffuse attenuation of background activity. The result on day 1 was uninterpretable due to noise. The results from days 4 and 7 are shown in Figure 1. After the discontinuation of naproxen, she was given supportive care and recovered after 11 days (day 12), with normalization of kidney function and metabolic abnormalities.
Examination of the patient’s medical records indicated that she had experienced recurring influenza-like symptoms, including fever, abdominal pain, cough/sputum, and joint pain, 2 months prior to presentation (day -69). Fever often exceeded 38 °C, reaching a peak 2 to 3 times a day and continuing for 3 to 7 days. Along with influenza-like symptoms, the patient experienced an erythematous lesion spanning her entire body. A maculopapular lesion with pruritus originated on the thigh and arm, subsequently spreading to other parts of the body. During this time, she also experienced elevated levels of ferritin, liver enzymes, and LDH. The fever and skin lesions responded well to the over-the-counter medication.
One month prior to presentation (day -30), the patient experienced frequent vomiting and fever, resulting in her admission to the Emergency Department. Furthermore, hepatosplenomegaly, frequent bleeding, and cervical lymph node enlargement were noted. During the admission period, the patient presented influenza-like symptoms similar to her past history. Piperacillin/ tazobactam intravenous (i.v.) 4.5 g was administered from day -13 to day 1. After the presentation of neurologic symptoms on day 1, the following medications were started: meropenem 0.8 g every 12 h; lorazepam 4 mg i.v. once; levetiracetam 250 mg i.v. every 24 h; and vancomycin 400 mg i.v. every 12 h. The neurologic symptoms observed in the patient were unlikely caused by any co-administered drugs, and the only likely cause was the administration of naproxen.
The diagnosis of Reye syndrome requires combined acute non-inflammatory encephalopathy and hepatopathy documented by a 3-fold or greater increase in AST and ALT, and ruling out inborn error of metabolism [1,6]. In the present case, the patient met all the criteria of Reye syndrome. Tonic seizure and loss of consciousness was observed (day 1, Glasgow coma scale E1V2M5), as well as a more than 3-fold increase in AST and ALT. Additionally, despite extensive diagnostic evaluation, including screening for rare diseases and inborn errors of metabolism, no possible cause was found.
To identify possible predisposing genetic polymorphisms contributing to the etiology of Reye syndrome, the patient was tested using a drug metabolizing enzymes and transporters (DMET) gene chip approximately 2 months after the day of presentation. The DMET gene chip is a useful tool for simultaneous genotyping of a large number of genetic variants for genes that encode drug-metabolizing enzymes and transporters [7]. The DMET platform tests a total of 1936 single-nucleotide polymorphism, copy number variation, insertion, and deletion markers over 231 genes, and covers 76 phase I enzymes, 62 phase II enzymes, 51 transporters, and 41 other genes that regulate intracellular processes [7]. Among genes involved in the metabolism of naproxen, UGT1A6 (*1/*2) and UGT2B7 (*1/*2) resulted in a heterozygote result, and both genes may have had decreased function (Table 2). Other genes that may have had clinical significance included homozygote (*6/*6) results for N-acetyltransferase 2 gene *6 (NAT2*6/6) (rs1799930) (Table 3).
Discussion
This case report described an 8-year-old female patient who developed Reye syndrome after administration of naproxen. Possible genetic etiology of Reye syndrome was explored using a DMET gene chip.
Reye syndrome was first described in 1963 by Reye et al as an acute metabolic encephalopathy primarily affecting children and adolescents [8]. Reye syndrome often develops promptly after viral illness during which aspirin was administered, with hepatic and encephalopathic manifestation [2]. There has been a significant drop in incidence of Reye syndrome since 1986, when aspirin was contraindicated in children [9]. The sharp decline in the incidence of Reye syndrome is partly due to the improved diagnosis of inborn errors of metabolism, since the diagnosis of Reye syndrome requires ruling out other causes [6]. Today, many of the Reye or Reye-like syndromes are explained as inborn errors of metabolism, without association with the use of aspirin [10]. In the present case, while the patient met the criteria for the diagnosis of Reye syndrome, the only possible cause of the symptoms was the use of naproxen, and the case was not aspirin-related, like “classical” Reye syndrome [11].
The patient experienced influenza-like symptoms and skin lesions 2 months prior to the onset on Reye syndrome symptoms, likely a viral infection, which is consistent with the known course of Reye syndrome. Naproxen was administered for 3 days for the treatment of fever and abdominal pain, after which she developed severe neurologic symptoms, liver failure, and acute kidney injury. One unusual clinical laboratory result was an extremely high ferritin level, which exceeded 40000 ug/L at the maximum. High ferritin is related to inflammatory states such as malignancy, liver, renal, or autoimmune states, but its role in the pathogenesis of Reye syndrome is unclear [12,13]. In the present case, the patient rapidly recovered with supportive care, similar to the reported Reye syndrome cases in which organ functions were rapidly recovered within a few days after the manifestation of neurologic symptoms [14].
In the present case, despite extensive diagnostic evaluation, including ruling out a rare disease, no probable cause was found [15]. While the patient presented mild hyperammonemia, hypoglycemia was not observed, which are 2 presentation of systemic primary carnitine deficiency. Hyperammonemia was not observed again. Other inborn errors of metabolism were further ruled out by additional diagnostic workup. Since the incidence of Reye syndrome is known to be associated with the administered dose of aspirin, and similar symptoms (drowsiness, metabolic acidosis, seizure activity, renal impairment, and hepatotoxicity) were reported in naproxen intoxication cases, the possibility of naproxen overdose was investigated [16,17]. While the patient received a higher than usual recommended dose of naproxen (5 mg/kg/day) of 22 mg/kg/day, the difference was marginal. The possibility of naproxen intoxication by drug interaction was considered; however, among the co-administered drugs, none had any clinically significant drug interaction reported with naproxen.
The possibility of the patient being a poor metabolizer of the drug metabolizing enzyme of naproxen was investigated using a DMET gene chip. While some genes involved in the metabolism of naproxen showed decreased function results, the overall result was inconclusive, as naproxen has more than one metabolic pathway and decreased function of the respective enzymes would not be sufficient to explain the observed symptoms (Table 2) [18]. Among the other investigated genes,
Conclusions
This case report described an 8-year-old female patient who developed Reye syndrome after the administration of naproxen. The patient developed neurologic symptoms and acute hepatic failure, which are defining characteristics of Reye syndrome. Through extensive diagnostic efforts, including screening for rare diseases and genetic polymorphisms, several possible genetic variants that can be associated with the etiology of Reye syndrome were identified. However, the polymorphisms in drug metabolizing enzymes and transporters could not adequately explain the etiology of this case.
References:
1.. Chapman J, Arnold JK: Reye syndrome, 2022, Treasure Island (FL), StatPearls Available from: https://www.ncbi.nlm.nih.gov/books/NBK526101/
2.. Schror K, Aspirin and Reye syndrome: A review of the evidence: Paediatr Drugs, 2007; 9(3); 195-204
3.. Merritt JL, Adam MP, Mirzaa GM, Pagon RA: GeneReviews((R)), 1993, Seattle (WA)
4.. Davies NM, Anderson KE, Clinical pharmacokinetics of naproxen: Clin Pharmacokinet, 1997; 32(4); 268-93
5.. : LiverTox: Clinical research information on drug-induced liver injury, 2012, Bethesda (MD), National Institute of Diabetes and Digestive and Kidney Diseases
6.. Gosalakkal JA, Kamoji V, Reye syndrome and Reye-like syndrome: Pediatr Neurol, 2008; 39(3); 198-200
7.. Arbitrio M, Di Martino MT, Scionti F, DMET (Drug Metabolism Enzymes and Transporters): A pharmacogenomic platform for precision medicine: Oncotarget, 2016; 7(3); 54028-50
8.. Reye RD, Morgan G, Baral J, Encephalopathy and fatty degeneration of the viscera. A disease entity in childhood: Lancet, 1963; 2(7311); 749-52
9.. Tasker RC, Update on pediatric neurocritical care: Paediatr Anaesth, 2014; 24(7); 717-23
10.. Waller P, Suvarna R, Is aspirin a cause of Reye’s syndrome?: Drug Safety, 2004; 27(1); 71-73
11.. Glasgow JF, Middleton B, Reye syndrome – insights on causation and prognosis: Arch Dis Child, 2001; 85(5); 351-53
12.. Hagstrom H, Nasr P, Bottai M, Elevated serum ferritin is associated with increased mortality in non-alcoholic fatty liver disease after 16 years of follow-up: Liver Int, 2016; 36(11); 1688-95
13.. Dimitrijevic ZM, Salinger-Martinovic SS, Jankovic RJ, Mitic BP, Elevated serum ferritin levels are predictive of renal function recovery among patients with acute kidney injury: Tohoku J Exp Med, 2019; 248(2); 63-71
14.. Ninove L, Daniel L, Gallou J, Fatal case of Reye’s syndrome associated with H3N2 influenza virus infection and salicylate intake in a 12-year-old patient: Clin Microbiol Infec, 2011; 17(1); 95-97
15.. Jun JS, Lee EJ, Park HD, Kim HS, Systemic primary carnitine deficiency with hypoglycemic encephalopathy: Ann Pediatr Endocrinol Metab, 2016; 21(4); 226-29
16.. Ali S, Pimentel JD, Ma C, Naproxen-induced liver injury: Hepatobiliary Pancreat Dis Int, 2011; 10(5); 552-56
17.. Al-Abri SA, Anderson IB, Pedram F, Massive naproxen overdose with serial serum levels: J Med Toxicol, 2015; 11(1); 102-5
18.. Tracy TS, Marra C, Wrighton SA, Involvement of multiple cyto-chrome P450 isoforms in naproxen O-demethylation: Eur J Clin Pharmacol, 1997; 52(4); 293-98
19.. Husain A, Zhang X, Doll MA, Identification of N-acetyltransferase 2 (NAT2) transcription start sites and quantitation of NAT2-specific mRNA in human tissues: Drug Metab Dispos, 2007; 35(5); 721-27
20.. Adole PS, Kharbanda PS, Sharma S, N-acetyltransferase 2 (NAT2) gene polymorphism as a predisposing factor for phenytoin intoxication in tuberculous meningitis or tuberculoma patients having seizures – A pilot study: Indian J Med Res, 2016; 143(5); 581-90
21.. Lee SW, Chung LS, Huang HH, NAT2 and CYP2E1 polymorphisms and susceptibility to first-line anti-tuberculosis drug-induced hepatitis: Int J Tuberc Lung Dis, 2010; 14(5); 622-26
Tables
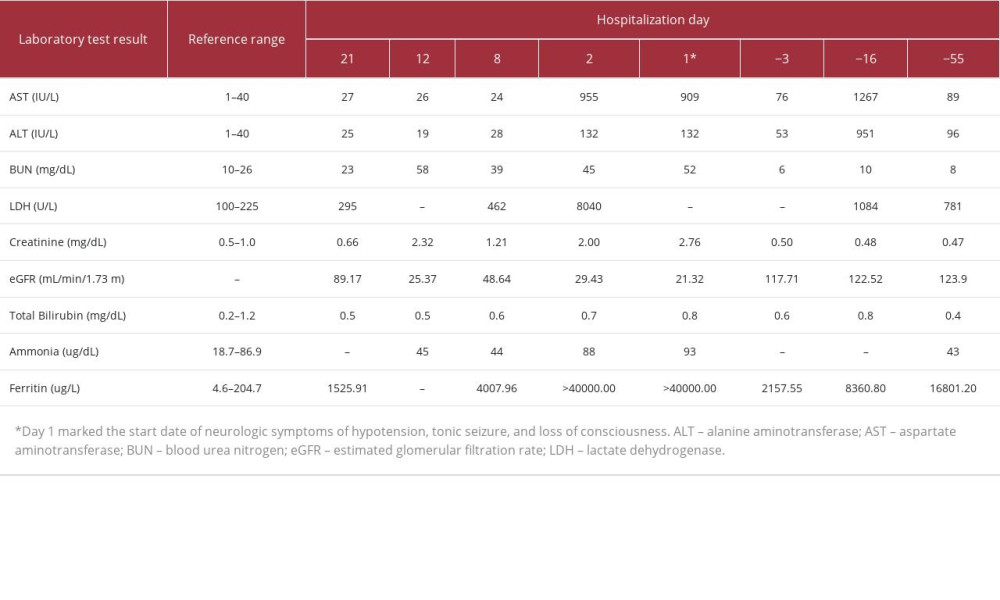 Table 1.. Clinical laboratory test results.
Table 1.. Clinical laboratory test results.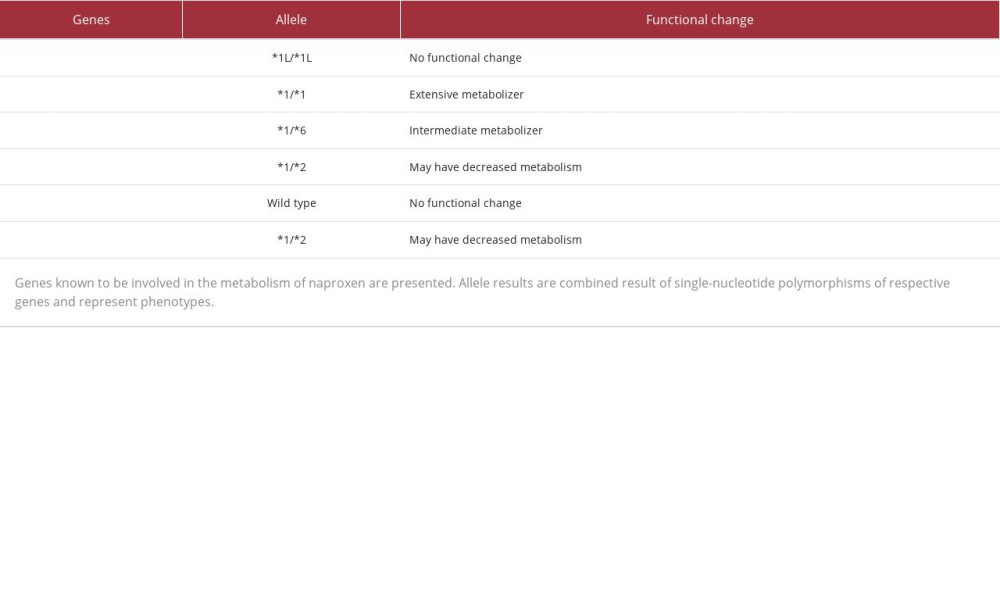 Table 2.. Pharmacogenetic test results for genes involved in the metabolism of naproxen.
Table 2.. Pharmacogenetic test results for genes involved in the metabolism of naproxen.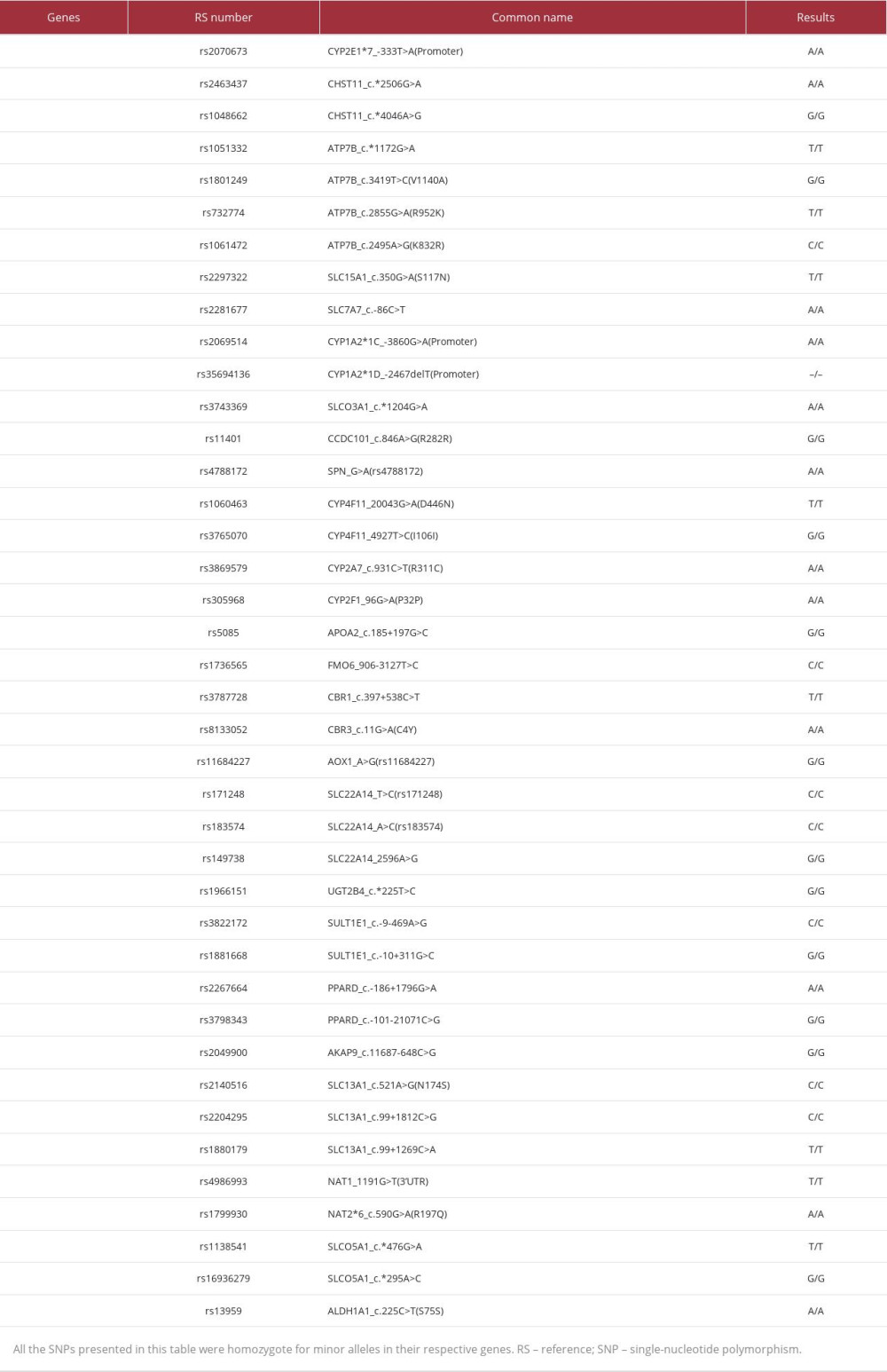 Table 3.. Drug metabolizing enzymes and transporters (DMET) test results for genes with homozygote variants.Table 1.. Clinical laboratory test results.Table 2.. Pharmacogenetic test results for genes involved in the metabolism of naproxen.Table 3.. Drug metabolizing enzymes and transporters (DMET) test results for genes with homozygote variants.
Table 3.. Drug metabolizing enzymes and transporters (DMET) test results for genes with homozygote variants.Table 1.. Clinical laboratory test results.Table 2.. Pharmacogenetic test results for genes involved in the metabolism of naproxen.Table 3.. Drug metabolizing enzymes and transporters (DMET) test results for genes with homozygote variants. In Press
17 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.943070
17 Mar 2024 : Case report ")
Am J Case Rep In Press; DOI: 10.12659/AJCR.943370
18 Mar 2024 : Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.943803
18 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.943467
Most Viewed Current Articles
07 Mar 2024 : Case report 
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133
10 Jan 2022 : Case report 
DOI :10.12659/AJCR.935263
Am J Case Rep 2022; 23:e935263
19 Jul 2022 : Case report 
DOI :10.12659/AJCR.936128
Am J Case Rep 2022; 23:e936128
23 Feb 2022 : Case report
DOI :10.12659/AJCR.935250
Am J Case Rep 2022; 23:e935250