21 September 2023: Articles 
Prion Disease After COVID-19: A Case Report
Unknown etiology, Challenging differential diagnosis, Rare disease
Karim Makhoul1ABDEF, Tova Beeber1ABCEF, Ryan Cordero1ABE, Areej Khan1ABDEF, Merjona Saliaj1ABDEF*DOI: 10.12659/AJCR.940564
Am J Case Rep 2023; 24:e940564






Abstract
BACKGROUND: Prion disease (PrD) is one of the rapidly progressive dementias. It typically requires several diagnostic criteria to fulfill a probable diagnosis, as definite diagnosis is based on isolated brain biopsy. There has been much debate on a possible infectious etiology of PrD. Viral infections are commonly pathologic in most neurodegenerative conditions. In PrD, misfolded proteins can be contagious and act as infective proteins, regardless of the pathologic agent. There is evidence that COVID-19 can result in neurologic manifestations, and neurodegeneration has been reported in the literature. There are several case reports describing parkinsonism after COVID-19, with Parkinson’s disease in particular noted in COVID-19. Few cases of PrD were reported after COVID-19 infection. We identified 1 case of PrD in the setting of COVID-19 at our hospital.
CASE REPORT: We report the case of a 62-year-old man admitted to Mount Sinai Queens Hospital Center, who presented with rapidly progressive dementia along with difficulty walking and myoclonus. All workup results were negative. He underwent MRI brain, but results were not revealing. Due to the high clinical suspicion, CSF protein 14-3-3 testing was ordered and was positive. Clinically, he experienced worsening neurological function after having been COVID-19-positive on admission. The case fulfilled the probable diagnostic criteria for diagnosing PrD. The patient continued to deteriorate and died due to the rapid progression of his condition.
CONCLUSIONS: Our case demonstrates the potential correlation of COVID with neurodegenerative conditions, especially prion disorders. While such cases are highly likely to be due to COVID-19, there is no definite evidence beyond coincidental findings. Future studies might be required to establish this correlation.
Keywords: COVID-19, Prion Diseases, Spongiform Encephalopathy with Neuropsychiatric Features, Male, Humans, Middle Aged, COVID-19, Dementia, Biopsy, Hospitalization
Background
PrD are transmissible spongiform encephalopathies manifesting after misfolding prion proteins accumulate within brain cells, resulting in ballooned neurons. Variable types of PrD exist, including Creutzfeldt-Jacob, kuru, iatrogenic, and genetic diseases such as fatal familial insomnia and genetic Creutzfeldt-Jacob and Gerstmann-Sträussler Scheinker syndrome [1,2]. Regardless of the etiology, clinical findings typically involve myoclonus, parkinsonian features, and rapidly progressive dementia. It can be challenging to diagnose PrD due to lack of specific tests. Therefore, diagnostic criteria have been developed to facilitate clinical diagnosis for clinicians [3].
Our literature search found a few cases of PrD after COVID-19 [4–7]. Remarkably, various neurological complications have been recognized in people after contracting COVID-19. While anosmia is considered a regular consequence of COVID, it is typically underrecognized as cranial nerve I dysfunction, a common neurological complication. Other serious post-COVID-19 complications include encephalopathy, meningitis, encephalitis, peripheral neuropathies, and increased risk of cerebrovascular insults and cranial neuropathies, which suggest a neuroinflammatory component of the viral illness [8]. Our case report is unique by highlighting the potential contribution of COVID-19 to PrD.
Case Report
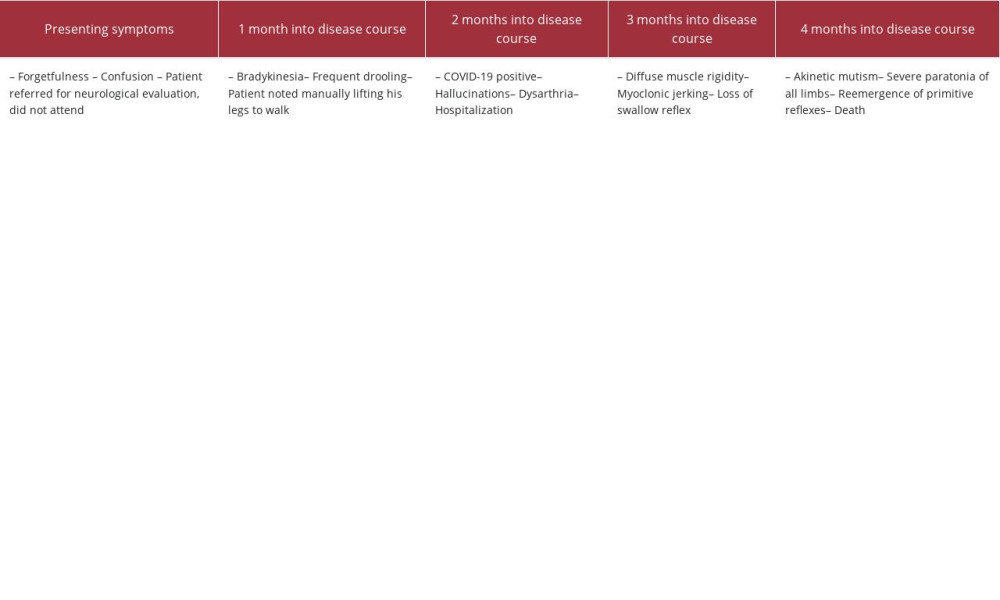
A 62-year-old man developed diffuse bradykinesia, drooling, and dementia 2 months prior to presenting to our hospital. He was noted to have difficulty walking. He was still highly functioning in terms of work until he was found at home on the floor after a fall, unable to walk and confabulating, with intermittent brief rapid involuntary jerks involving 1 limb at a time, suggestive of myoclonic jerks. On admission, he was found to be COVID-19 positive, but was afebrile and asymptomatic aside from the typical COVID respiratory manifestations. He was also diagnosed with rhabdomyolysis based on a CPK value of 3542. Levels of magnesium, ethanol, troponin, acetaminophen, salicylate, ammonia, mushroom Rf212, fentanyl, and 10 panel drug screen panel were normal negative. On the second day of hospitalization, he underwent thyroid function testing (normal), hepatic function testing (mild AST elevations), and initial lumbar puncture, which was remarkable only for protein elevated to 61. Cerebral spinal fluid (CSF) from this lumbar puncture was negative for Escherichia coli K1, Haemophilus influenzae, Listeria monocytogenes, Neisseria meningitidis, Streptococcus agalactiae, Streptococcus pneumoniae, Cytomegalovirus (CMV), Cryptococcus neoformans gattii, Enterovirus, Herpes simplex virus 1 (HSV-1), Herpes simplex virus 2 (HSV-2), Human herpesvirus 6 (HHV-6), Human parechovirus, and Varicella zoster virus (VZV). Testing for HIV, syphilis, B12, TSH, NDMA AB IgG, Glutamic Acid Decarboxylase, and Lyme antibodies were all negative. He had 2 indeterminate QuantiFERON tests, with no findings suggestive of active tuberculosis on chest X-ray. He also underwent CT brain and MRI brain, both of which were repeated twice and were normal without any diffusion restriction. EEG was repeated twice and revealed findings of mild encephalopathy with no sharp-wave complexes. On week 2 of hospitalization, he underwent a second lumbar puncture, which was sent for autoimmune encephalitis panel, TAU protein quantification, 14-3-3 protein levels, and paraneoplastic markers. Of these, 14-3-3 protein was found to be elevated to 3902 (ref. range <30–1999 Au/mL). A diagnosis of probable PrD was established based on the positive result of 14-3-3 protein detection in CSF along with a clinical picture of rapidly progressive dementia with bradykinesia and myoclonus.
Approximately 3 weeks into hospitalization, the patient became progressively mute and had difficulty swallowing soft foods, requiring PEG tube placement. He subsequently became spastic with severe pain on passive flexion extension. Six weeks after admission, the patient was declared dead (Table 1).
Discussion
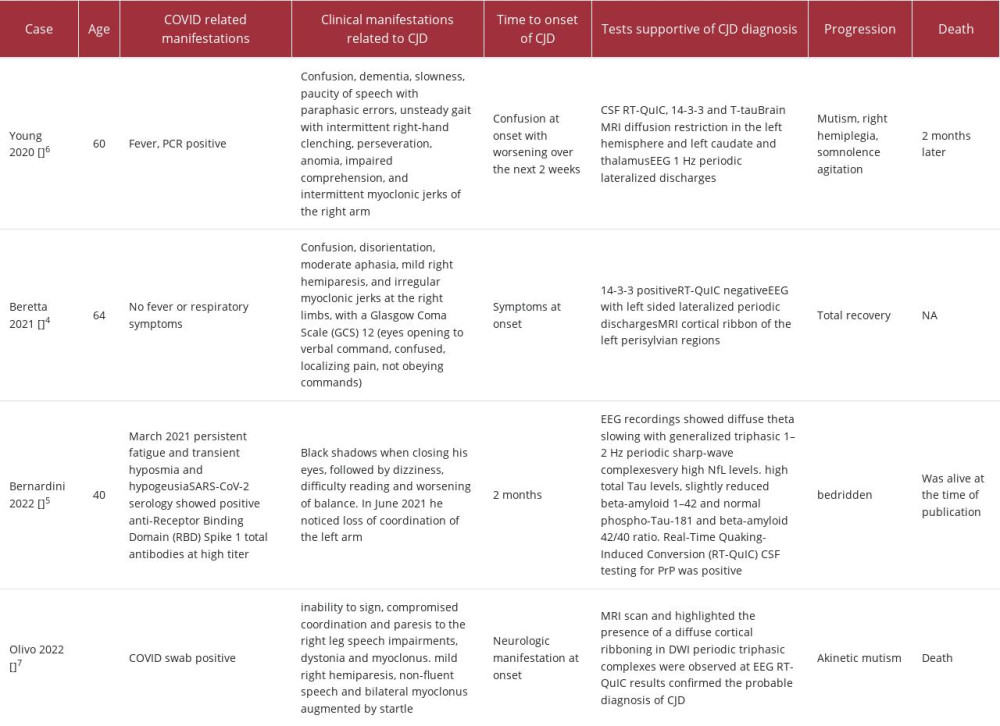
We were able to identify 4 cases in the literature (Table 2) comparable to our case with prion disorder happening after COVID-19 infection [4–7]. While 2 cases had neurologic manifestations at onset [4,7], the 2 other cases had CJD-related symptoms at 2 weeks [6] or 2 months [5] after upper-respiratory symptoms. Indeed, 2 cases had COVID-19-related manifestations, with 1 manifesting as fever [6] and the other manifesting as fatigue, hyposmia, and hypogeusia [5]. Counter-intuitively, 2 cases did not have any COVID-19-related manifestations prior to neurologic symptoms [4,7]. However, they tested positive on COVID-19 PCR testing. Most of the cases had CJD-related diagnostic features, including clinical evidence such as rapidly progressing dementia and myoclonus, radiologic features such as cortical ribboning, neurophysiological signs such as periodic lateralized discharges on EEG, and laboratory findings with protein positive 14-3-3 and RT-QuIC, but not all the cases fulfilled most of the criteria.
Our patient had a clinical picture that fit with PrD, including a rapidly progressive course along with generalized full-body myoclonus. Despite not fulfilling the radiologic and neurophysiological criteria, our patient had a positive 14-3-3 protein in the CSF. As such, he fulfilled the probable diagnostic criteria for CJD, with rapidly progressive dementia along with bradykinesia and myoclonus associated with a positive protein 14-3-3, which fits with the probable diagnostic criteria [3].
The diagnosis of prion disorders is challenging by itself, as definitive diagnosis relies on clinical neurodegeneration along with a histopathological evidence of disease activity within brain parenchyma. While brain biopsy is theoretically the method for a definitive diagnosis, it is invasive and associated with adverse effects, including hemorrhage. The other potential drawback is false-negative results in light of sampling errors as proven by a meta-analysis of brain biopsies with an average diagnostic success rate of 54% [9].
It can be difficult to establish a correlation between PrD and COVID-19 based on laboratory workup. However, this was clinically evident through the timeline of event development, since symptom onset was associated with COVID-19-positivity. It remains difficult to establish a clear correlation because the patient was admitted after a fall but had been developing undefined symptoms reported by coworkers and family members. Whether COVID-19 contributed to his PrD or resulted in the clinical correlation cannot be determined. It is worth noting that in most instances patients with COVID-19 acquire a hyperinflammatory state typically known as cytokine storm, in which excessive inflammatory markers are released within the area of infection. Whether cytokine storm contributes to development of prion disease is yet to be determined. However, excessive protein secretions might also contribute to protein misfolding [10]. SARS-CoV-2 cell entry is facilitated by a viral glycoprotein termed S glycoprotein or S1 spike proteins [11], which plays a role in viral recognition by ACE2R cell membrane receptors [12]. S1 spike proteins were hypothesized to possess prion-like properties with potential contribution to neurodegenerative conditions [13]. This could be the culprit protein playing a role in prion formation. COVID-19 by itself has been described to result in neurodegeneration. However, the exact correlation was not established despite a few reports of Parkinson’s disease [14]. There are definite hypotheses that variable pathogen related-illnesses can result in neurodegenerative conditions, most prominently the Braak hypothesis, wherein gut microbiota provoke protein misfolding and alpha synuclein accumulation, traveling through the vagal nerve to the CNS [15]. It remains difficult to establish such theoretical hypotheses, and the correlation between COVID-19, and in our case it remains hypothetical. While our patient was found to be positive for COVID-19 later in the disease course, our case is important as it suggests a potential correlation between PrD and COVID-19, but this is unproven. The Spanish Flu was followed by an epidemic of Von Economo’s encephalitis [16], and early recognition of potential neurodegenerative conditions after COVID-19 might provide clinical evidence of an association between COVID-19 and these neurologic diseases.
Conclusions
Evidence in the literature about an association between COVID-19 and neurodegeneration is unclear. For the most part, at least clinically, cases were confirmed from the standpoint of acuity to have been the result of COVID-19, but there is no definite biochemical evidence of such a correlation. Nonetheless, it is evident that multiple neurodegenerative conditions might be a result of pathogenic illnesses, most commonly prion disorders. Despite an unclear correlation, it is important that sequala of COVID-19 infection be examined with caution.
References:
1.. Wang H, Rhoads DD, Appleby BS, Human prion diseases: Curr Opin Infect Dis, 2019; 32(3); 272-76
2.. Appleby BS, Shetty S, Elkasaby M, Genetic aspects of human prion diseases.: Front Neurol., 2022; 13; 1003056
3.. Hermann P, Appleby B, Brandel JP, Biomarkers and diagnostic guidelines for sporadic Creutzfeldt-Jakob disease.: Lancet Neurol, 2021; 20(3); 235-46
4.. Beretta S, Stabile A, Balducci C, COVID-19-associated immune-mediated encephalitis mimicking acute-onset Creutzfeldt-Jakob disease: Ann Clin Transl Neurol, 2021; 8(12); 2314-18
5.. Bernardini A, Gigli GL, Janes F, Creutzfeldt-Jakob disease after COVID-19: infection-induced prion protein misfolding? A case report: Prion, 2022; 16(1); 78-83
6.. Young MJ, O’Hare M, Matiello M, Schmahmann JD, Creutzfeldt-Jakob disease in a man with COVID-19: SARS-CoV-2-accelerated neurodegeneration?: Brain Behav Immun, 2020; 89; 601-3
7.. Olivo S, Furlanis G, Buoite Stella A, Rapidly evolving Creutzfeldt-Jakob disease in COVID-19: From early status epilepticus to fatal outcome: Acta Neurol Belg, 2023; 123(4); 1553-56
8.. Pavel B, Moroti R, Spataru A, Neurological manifestations of SARSCoV2 infection: A narrative review: Brain Sci, 2022; 12(11); 1531
9.. Bai HX, Zou Y, Lee AM, Diagnostic value and safety of brain biopsy in patients with cryptogenic neurological disease: A systematic review and meta-analysis of 831 cases: Neurosurgery, 2015; 77(2); 283-95 discussion 295
10.. Burwinkel M, Riemer C, Schwarz A, Role of cytokines and chemokines in prion infections of the central nervous system: Int J Dev Neurosci, 2004; 22(7); 497-505
11.. Duan L, Zheng Q, Zhang H, The SARS-CoV-2 spike glycoprotein biosynthesis, structure, function, and antigenicity: implications for the design of spike-based vaccine immunogens: Front Immunol, 2020; 11; 576622
12.. Letko M, Marzi A, Munster V, Functional assessment of cell entry and receptor usage for SARS-CoV-2 and other lineage B betacoronaviruses: Nat Microbiol, 2020; 5(4); 562-69
13.. Lukiw WJ, Jaber VR, Pogue AI, Zhao Y, SARS-CoV-2 invasion and pathological links to prion disease: Biomolecules, 2022; 12(9); 1253
14.. Makhoul K, Jankovic J, Parkinson’s disease after COVID-19: J Neurol Sci, 2021; 422; 117331
15.. Claudino Dos Santos JC, Lima MPP, Role of enteric glia and micro-biota-gut-brain axis in parkinson disease pathogenesis: Ageing Res Rev, 2023; 84; 101812
16.. Lutters B, Foley P, Koehler PJ, The centennial lesson of encephalitis lethargica: Neurology, 2018; 90(12); 563-67
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953136
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953129
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952791

Most Viewed Current Articles
07 Dec 2021 : Case report
22,758,880
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,727
175,727
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,401
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,411
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133