23 December 2023: Articles 
Hypopharyngeal Diffuse Large B-Cell Lymphoma in a 74-Year-Old Man Presenting with Dysphagia: A Case Report
Unusual clinical course, Challenging differential diagnosis, Rare disease
Hisataka OminatoDOI: 10.12659/AJCR.942070
Am J Case Rep 2023; 24:e942070






Abstract
BACKGROUND: Malignant lymphomas can occur at various sites. Hypopharyngeal tumors are at risk for airway obstruction and require rapid diagnosis and treatment. Most hypopharyngeal malignancies are squamous cell carcinomas; other tumors are rare. To date, only a few cases of malignant hypopharyngeal lymphoma have been reported, and its specific characteristics are unknown. Herein, we report a case of right hypopharyngeal diffuse large B-cell lymphoma (DLBCL) in a 74-year-old man with dysphagia.
CASE REPORT: A 74-year-old man presented to our hospital with dysphagia. He had no relevant medical history. Endoscopic examination revealed a right hypopharyngeal tumor. The surface of the tumor was smooth, with no evidence of hemorrhage. Computed tomography revealed a 40-mm mass located in the hypopharynx. We performed a tracheotomy and biopsy of the tumor. Histopathological examination revealed a diffuse proliferation of large atypical B cells with negative staining for Epstein-Barr virus by in situ hybridization. Immunohistochemical staining was positive for CD20 but negative for CD3 and CD10. The patient was administered chemotherapy. The tumor reduced in size, and the patient recovered completely. During the two-year follow up, no recurrence of cancer was observed.
CONCLUSIONS: Although most hypopharyngeal tumors are squamous cell carcinomas (SCCs), the possibility of other types of tumors should also be considered. Malignant lymphoma of the hypopharynx is rare, and more cases need to be studied and reported in the future.
Keywords: Airway Obstruction, Hypopharynx, Lymphoma, Non-Hodgkin, Male, Humans, Aged, Epstein-Barr Virus Infections, Herpesvirus 4, Human, Hypopharyngeal Neoplasms, Deglutition Disorders, Lymphoma, Large B-Cell, Diffuse, Carcinoma, Squamous Cell
Background
Malignant lymphomas can occur at various sites. In malignant head and neck lymphomas, the lymph nodes, tonsils, and salivary glands are the most common sites [1]. Approximately 95% of hypopharyngeal malignancies are SCC [2]. Hypopharyngeal tumors other than SCC and malignant lymphomas of the hypopharynx are rare. Hypopharyngeal tumors pose a risk of airway obstruction and should be diagnosed and treated at an early stage. Few cases of hypopharyngeal malignant lymphoma have been reported, and its specific characteristics are unknown. Although the site was different, a similar case of B-cell lymphoma in the epiglottis has been reported previously [3]. Therefore, more cases should be reported. This report presents a case of right hypopharyngeal diffuse large B-cell lymphoma (DLBCL) in a 74-year-old man presenting with dysphagia.
Case Report
A 74-year-old man presented to our hospital with dysphagia but no pain. The patient had no relevant medical history. Endoscopic examination revealed a right hypopharyngeal tumor occupying the glottis (Figure 1). The surface of the tumor was smooth, with no signs of hemorrhage. Computed tomography revealed a 40-mm mass located in the hypopharynx (Figure 2). Lymph nodes were not enlarged. Hematology findings showed a peripheral blood white blood cell count of 7460/μl; C-reactive protein was 0.75 mg/dl, lactate dehydrogenase was 218 IU, squamous cell carcinoma-associated antigen was 0.6 ng/ml, and soluble interleukin-2 receptor was 328 U/ml. We performed a tracheotomy and biopsy of the tumor. Histopathological examination revealed a diffuse proliferation of large atypical B cells with negative staining for Epstein-Barr virus by in situ hybridization. Immunohistochemical staining was positive for CD20 and negative for CD3, CD10, and p16. A high proliferation index of lymphoid cells highlighted by Ki67 was noted (Figure 3). The patient was diagnosed with DLBCL, stage IE, with an R-IPI score of 1 (age >60, performance status 0, normal LDH of 218 IU, 0-1 extranodal sites, and stage I/II disease).
He was referred to the hematology department of another hospital for chemotherapy and treated with 6 courses of rituximab, cyclophosphamide, adriamycin, vincristine, and prednisone (R-CHOP). The tumor size reduced, and the patient showed a complete recovery (Figure 4). During the 2-year follow up, there was no recurrence of the tumor.
Discussion
Head and neck cancers are more frequently squamous cell carcinomas, while tumors of other histological types are less frequent [4]. Hypopharyngeal cancer is relatively rare, accounting for approximately 3% of all head and neck cancers [5]. Patients with hypopharyngeal tumors have an average age of 63 years, and 75% are males [2]. Most malignant hypopharyngeal tumors are squamous cell carcinomas [2].
Malignant lymphomas often arise in the lymph nodes; however, approximately 40% of non-Hodgkin lymphomas occur as extranodal lesions[6]. Head and neck lymphomas occur frequently in Waldeyer’s pharyngeal ring, accounting for 40–50% of cases [7]. DLBCL is estimated to account for 32% of B-cell lymphomas [8], while extranodal head and neck DLBCL account for 13.6% [9]. To date, only a few cases of malignant hypopharyngeal lymphoma have been reported. Among malignant lymphomas of the head and neck, malignant lymphoma of the hypopharynx/larynx is very rare, accounting for approximately 3% of the cases [1]. Hypopharyngeal DLBCL is rare; hence, it is important to accumulate more data on its symptoms and findings. Hypopharyngeal tumors involve risk for airway obstruction and require rapid diagnosis and treatment. Although at a different site, a similar case of B-cell lymphoma in the epiglottis was reported [3,10]. Malignant lymphoma of the larynx is also unusual. Hypopharyngeal and laryngeal malignant lymphomas are rare and hypothesized to have a similar pathogenesis. This case is similar to the present case and is expected to be studied and accumulated in the future.
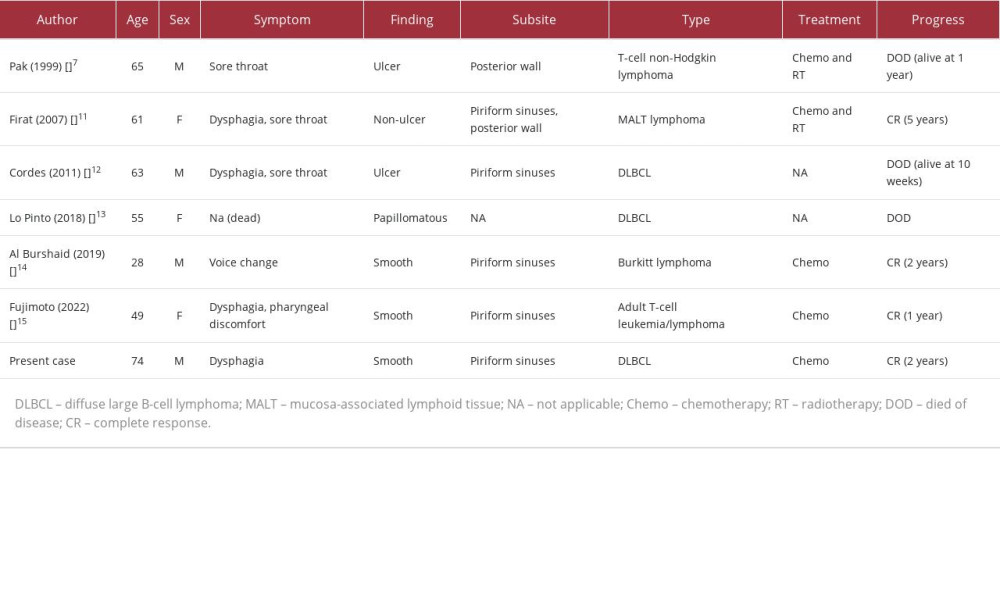
PubMed was searched for the period through April 2023 for studies published in English using the keywords “hypopharynx” or “lymphoma” for both abstracts and full texts. A few cases of hypopharyngeal malignant lymphoma have been reported and are summarized in Table 1 [7,11–15]. There were 7 cases of hypopharyngeal malignant lymphoma. The median age of the patients was 61 years (range, 28–74 years). Four patients were males and 3 were females. The patients presented with symptoms such as dysphagia (4 patients); sore throat (3 patients); and voice change and pharyngeal discomfort (1 patient each). There were 3 cases of smooth, 2 cases of ulcerous, and 1 each of non-ulcerous and papillomatous tumors. Regarding tumor location, 5 tumors were located in the piri-form sinuses and 2 in the posterior wall. The histological types of malignant lymphomas reported were 3 cases of DLBCL and 1 case each of mucosa-associated lymphoid tissue lymphoma, Burkitt’s lymphoma, adult T-cell leukemia/lymphoma, and T-cell non-Hodgkin lymphoma. Treatment included chemotherapy in 3 cases, chemoradiotherapy in 2 cases, and no treatment in the other 2 cases. The age of patients with hypopharyngeal malignant lymphoma was similar to that of patients with hypopharyngeal tumors. Additionally, the male-to-female ratio was nearly equal in the cases of hypopharyngeal malignant lymphoma.
Conclusions
Although most hypopharyngeal tumors are SCCs, the possibility of other types of tumors should be considered. Malignant lymphoma of the hypopharynx is rare, and more cases need to be studied in detail and reported in the future.
Figures
References:
1.. Storck K, Brandstetter M, Keller U, Knopf A, Clinical presentation and characteristics of lymphoma in the head and neck region: Head Face Med, 2019; 15(1); 1
2.. Hoffman HT, Karnell LH, Funk GF, The National Cancer Data Base report on cancer of the head and neck: Arch Otolaryngol Head Neck Surg, 1998; 124(9); 951-62
3.. Liu C, Delaney S, Brown TN, An unusual presentation of B-cell lymphoma as a large isolated epiglottic mass: Case report and literature review: Case Rep Otolaryngol, 2016; 2016; 9787432
4.. Bhat GR, Hyole RG, Li J, Head and neck cancer: Current challenges and future perspectives: Adv Cancer Res, 2021; 152; 67-102
5.. Garneau JC, Bakst RL, Miles BA, Hypopharyngeal cancer: A state of the art review: Oral Oncol, 2018; 86; 244-50
6.. Vitolo U, Seymour JF, Martelli M, Extranodal diffuse large B-cell lymphoma (DLBCL) and primary mediastinal B-cell lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up: Ann Oncol, 2016; 27(Suppl. 5); v91-v102
7.. Pak MW, Woo JK, Van hasselt CA, T-cell non-Hodgkin’s lymphoma of the larynx and hypopharynx: Otolaryngol Head Neck Surg, 1999; 121(3); 335-36
8.. Zelenetz AD, Gordon LI, Chang JE, NCCN Guidelines(R) Insights: B-cell lymphomas, Version 5.2021: J Natl Compr Canc Netw, 2021; 19(11); 1218-30
9.. Castillo JJ, Winer ES, Olszewski AJ, Sites of extranodal involvement are prognostic in patients with diffuse large B-cell lymphoma in the rituximab era: An analysis of the Surveillance, Epidemiology and End Results database: Am J Hematol, 2014; 89(3); 310-14
10.. Chang HM, Li CC, Tsai SC, Tsao TY, Epiglottic diffuse B-cell malignant lymphoma: A case report: Mol Clin Oncol, 2016; 4(1); 58-60
11.. Firat Y, Kizilay A, Sogutlu G, Mizrak B, Primary mucosa-associated lymphoid tissue lymphoma of hypopharynx: J Craniofac Surg, 2007; 18(5); 1189-93
12.. Cordes C, Tiemann M, Tiemann K, Epstein-Barr virus-associated diffuse large B-cell lymphoma of the hypopharynx: B-ENT, 2011; 7(1); 43-46
13.. Lo Pinto S, Barranco R, Cucci M, Sudden death secondary to an undiagnosed B-cell lymphoma of the hypopharynx and infiltration of the inferior constrictor muscle: J Forensic Sci, 2018; 63(4); 1303-6
14.. Al Burshaid DI, Nasser MA, Nagaraj V, Al Shehabi MH, Sporadic Burkitt’s lymphoma of the hypopharynx: A case report: Saudi J Med Med Sci, 2019; 7(2); 114-17
15.. Fujimoto S, Matsuura K, Nakamura H, Adult T-cell leukemia/lymphoma with extranodal involvement of the hypopharynx: Cureus, 2022; 14(2); e22723
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133