21 June 2020: Articles 
An Unusual Intraoral Lipoma: A Case Report and Literature Review
Unusual clinical course, Rare disease, Educational Purpose (only if useful for a systematic review or synthesis)
Claudio Maria De Sanctis1BEF*, Francesca Zara1BEF, Gian Luca Sfasciotti1BEFDOI: 10.12659/AJCR.923503
Am J Case Rep 2020; 21:e923503






Abstract
BACKGROUND: Lipoma is a painless tumor derived from mesenchymal connective tissue. It manifests itself on soft tissue and is characterized by a slow and circumscribed growth. Its incidence in the oral cavity is relatively low (1–4%). Despite the fact that it poses very little threat, as it is a benign form, as opposed to liposarcomas, its position in the oral cavity can create the prerequisite conditions for the buccal mucosa to be continuously traumatised by chewing and thus be altered. Given the fact that it is a painless lesion, patients can undergo years with an intraoral lipoma without ever recognizing it. There, we report a case of an unusual, large, intraoral lipoma that caused speech problems.
CASE REPORT: A 46-year-old man presented a large, soft mass in the buccal mucosa. No pain was described by the patient, but there was a slight impediment in chewing and talking. The patient underwent surgical excision of the lesion, which was then sent for histological examination. Results confirmed the initial hypothesis that the lesion was a lipoma.
CONCLUSIONS: Lipomas can be subtle lesions that may go unnoticed for several years until their size causes difficulties with normal masticatory movement and aesthetic problems. However, given the benignity of the mass, it rarely poses a serious threat to health. They are relatively sporadic lesions and, after being removed, relapse is rare.
Keywords: Lipoma, Pathology, Oral, Surgery, Oral, Mouth, Mouth Mucosa, Mouth Neoplasms
Background
Lipoma is a painless tumor derived from mesenchymal connective tissue, composed mainly of mature adipocytes. It manifests in soft tissue and has slow and circumscribed growth. In relation to the whole body, it is possible to differentiate between
Because it is a painless lesion, a patient can have an intra-oral lipoma for years without noticing it. In the present case, the main problem was initial trauma and speech difficulty due to the size of the tumefaction. One main problem, especially in this case, is the possibility of a continuous trauma from mastication, with possible keratosis and further complications. In the present case of a giant intraoral lipoma, the site of the lipoma was unusual and it grew to over 2 cm, making it an atypical clinical entity [10].
Case Report
A 46-year-old man was referred to the Department of Oral and Maxillo-Facial Sciences of “Sapienza”, University of Rome, with a complaint of a large mass impeding speech and causing discomfort when chewing. The patient presented with hypercholesterolemia during medical anamnesis, but no other systemic or medical condition was noted. He had no history of smoking or substance abuse. Extraoral examination revealed no alteration of vertical nor horizontal symmetry (Figure 1). Instead, oral examination revealed a large mobile mass in the left buccal mucosa (Figure 2). Measurements showed a 2.5×2 cm oval mass. The mass was soft and had a normal pink-colored mucosa overlay, and no pain was felt by the patient during examination. The treatment consisted of a vertical surgical incision with a Bard-Parker #15 C blade under local anaesthesia on the mucosa at the maximum height of the tumefaction (Figure 3). Peripherical dissection with Metzenbaum scissors (Figure 4) allowed separation of the lesion capsule from the surrounding tissue, and applying external pressure permitted the avulsion of the lesion from its site (Figure 5). The surgical incision (Figure 6) was then sutured with 3.0 Vicryl (Ethicon, polyglactin 910, braided absorbable suture, 3/8, cutting edge) along the line of the incision (Figure 7). The excised lesion was 2.5×2 cm (Figure 8).
Histological examination with hematoxylin and eosin staining revealed mature adipocytes without atypia, consistent with a lipoma. The suture points were removed on the 7th day after surgery (Figure 9). A further check was made on the 14th day to ensure proper healing (Figure 10).
Discussion
The buccal mucosa has abundant fatty tissue and thus is the most common site of intraoral lesions [4,5]. Areas such as the tongue and hard palate are less commonly affected because they have less fatty tissue. Studart-Soares et al. [11] reviewed 450 cases of intraoral lipomas and found that the most common site was the buccal mucosa (n=174; 38.7%), followed by the vestibule (n=35; 7.8%), retromolar area (n=21; 4.7%), and other sites (n=220; 48.8%). They found no significant difference between males and females with respect to lesion distribution: 256 were males (52.2%) and 234 were females (47.8%). A study by Taira et al. reviewed 207 cases and found that the buccal mucosa was the most common site (n=84, 40.6%), followed by the tongue (n=37, 17.9%), lips (n=26, 12.6%), and other areas (n=60, 28.9%), and found no significant sex distribution difference [12]. People in their 4th to 6th decades of life were most commonly affected [11–13]. The etiology and pathogenesis remain unclear, although endocrine, mechanical, inflammatory, hypercholesterolemia, and obesity factors are reported be associated with lipomas [13]. In the present case, the lipoma was located at the most common site but it was unusually large, and it is fortunate that it was removed before there was any important trauma to the overlaying mucosa. There were no surgical complications, but we had to suture the flaps tightly to avoid trauma because the slow-growing mass created a larger area of mucosa, which, if not tightly secured with the suture, could droop and be traumatised through chewing.
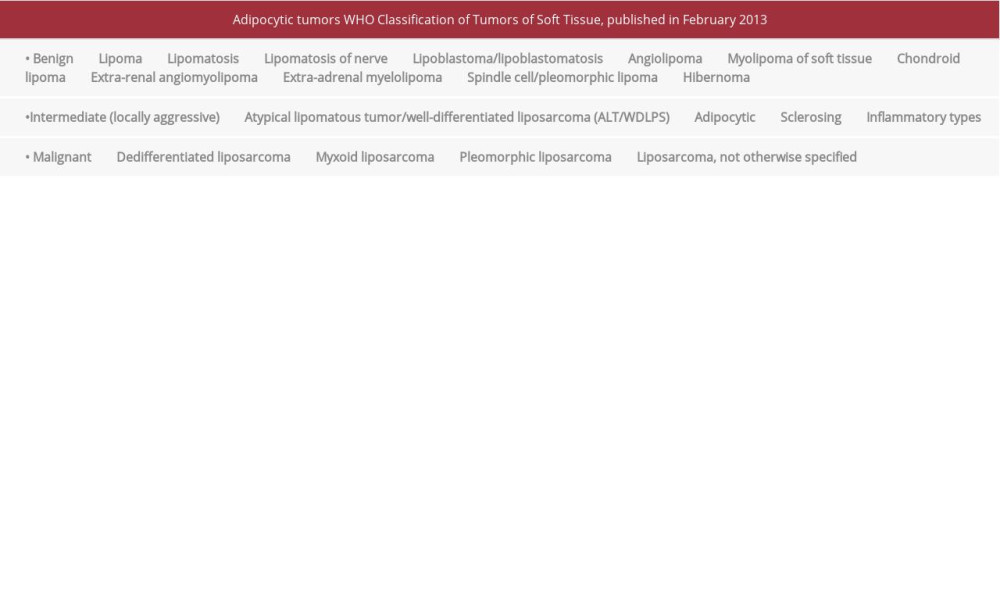
One possible risk in having such a large mass in the oral cavity and subjecting it to trauma is a possible degeneration of the histopathological features, leading to similar ALT-like characteristics. Differential diagnosis between other adipocytic tumors is through histologic examination and gene sequencing [14]. There are 4 types of histological variants of ALT/WDLPS, of which the adipocytic variant (lipoma-like) is the most common. ALT/WDLPS are a form of adipocytic tumor that uncommonly arises in the buccal cavity. Its danger lies in the possible dedifferentiation of the adipocytes, leading to malignancy. Histologic observation and immunohistochemistry help make the correct classification and diagnosis [15].
Conclusions
Lipomas are often unnoticed by the patient, and the main problems are self-inflicted trauma due to the bulge, which interferes with the normal chewing, and aesthetic problems. The only possible treatment is surgical excision of the lesion along with its capsule. Recurrence is rare, but an aggressive excision might perforate the encapsulating membrane and create a spill of cells, which might lead to recurrence. It is important to approach the lesion with a firm but non-aggressive incision and to perform the peripheral dissection with Metzenbaum scissors in order to free the lesion from the surrounding tissues. Due to its benign nature, the lesion does not generally need any further radiotherapy or chemotherapy [1].
Figures
References:
1.. McTighe S, Chernev I, Intramuscular lipoma: A review of the literature: Orthop Rev (Pavia), 2014; 6(4); 5618
2.. Shah VS, Harish M, Patel JR, Shah N, Infiltrating angiolipoma of the cheek: BMJ Case Rep, 2013; 2013; bcr2013200041 : pii:
3.. Paparo F, Massarelli M, Giuliani G, A rare case of parotid gland lipoma arising from the deep lobe of the parotid gland: Ann Maxillofac Surg, 2016; 6(2); 308-10
4.. Agarwal R, Kumar V, Kaushal A, Singh RK, Intraoral lipoma: A rare clinical entity: BMJ Case Rep, 2013; 2013; bcr2012007889 : pii:
5.. Manor E, Sion-Vardy N, Joshua BZ, Bodner L, Oral lipoma: Analysis of 58 new cases and review of the literature: Ann Diagn Pathol, 2011; 15(4); 257-61
6.. Cheng J, Yu H, Wang L, Primary oral and maxillofacial liposarcoma: A clinicopathological and immunohistochemical study of eleven cases: Arch Med Sci, 2012; 8(2); 316-23
7.. Kooby DA, Antonescu CR, Brennan MF, Singer S, Atypical lipomatous tumor/ well-differentiated liposarcoma of the extremity and trunk wall: Importance of histological subtype with treatment recommendations: Ann Surg Oncol, 2004; 11(1); 78-84
8.. Fletcher CDM, Bridge JA, Hogendoorn P, Mertens FF: WHO classification of tumors of soft tissue and bone, 2013; 321-24, Lyon, IARC Press
9.. Wong NACS, O’Mahony O, Intramucosal fat is uncommon in large bowel polyps but raises three differential diagnoses: J Clin Pathol, 2019; 72(8); 562-65
10.. Egido-Moreno S, Lozano-Porras AB, Mishra S, Intraoral lipomas: Review of literature and report of two clinical cases: J Clin Exp Dent, 2016; 8(5); e597-603
11.. Studart-Soares EC, Costa FW, Sousa FB, Oral lipomas in a Brazilian population: A 10-year study and analysis of 450 cases reported in the literature: Med Oral Patol Oral Cir Bucal, 2010; 15(5); e691-96
12.. Taira Y, Yasukawa K, Yamamori I, Iino M, Oral lipoma extending superiorly from mandibular gingivobuccal fold to gingiva: A case report and analysis of 207 patients with oral lipoma in Japan: Odontology, 2012; 100(1); 104-8
13.. Juliasse LE, Nonaka CF, Pinto LP, Lipomas of the oral cavity: Clinical and histopathologic study of 41 cases in a Brazilian population: Eur Arch Otorhinolaryngol, 2010; 267(3); 459-65
14.. Hameed M, Pathology and genetics of adipocytic tumors: Cytogenet Genome Res, 2007; 118(2–4); 138-47
15.. Stojanov IJ, Mariño-Enriquez A, Bahri N, Lipomas of the oral cavity: Utility of MDM2 and CDK4 in avoiding overdiagnosis as atypical lipomatous tumor: Head Neck Pathol, 2019; 13(2); 169-76
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133