31 August 2020: Articles 
Horizontal Transmission of Hepatitis B Virus Genotype C Among Members of a Wrestling Club in Japan
Rare coexistence of disease or pathology
Kazuhide Takata1E*, Eri Yamauchi1C, Satoshi Shakado1E, Yoshinari Uehara23E, Hiromi Fukuda1E, Ryo Yamauchi1E, Naoaki Tsuchiya1B, Hideo Kunimoto1E, Takashi Tanaka1E, Keiji Yokoyama1E, Daisuke Morihara1E, Yasuaki Takeyama1E, Shotaro Sakisaka1E, Fumihito Hirai1EDOI: 10.12659/AJCR.925044
Am J Case Rep 2020; 21:e925044






Abstract
BACKGROUND: In adulthood, most cases of acute hepatitis B virus (HBV) infection are transmitted either by sexual contact or by contaminated needles, but there are other modes of transmission. We report on three cases of HBV infection among members of a wrestling club.
CASE REPORT: A 19-year-old male wrestling athlete was admitted with acute hepatitis B. Five months later, 2 other men, who were members of the same wrestling club, were diagnosed with HBV infection. The full-length sequences of the HBV DNA were identical in all three cases and classified as subgenotype C2 on phylogenetic analysis. This is the most common genotype found in Japan. No history of sexual or bleeding contact with acquaintances outside the club was noted in any of these cases. This suggests horizontal transmission within the wrestling club.
CONCLUSIONS: The possibility of HBV transmission through bleeding wounds and sweat is a concern in contact sports such as wrestling. Hence, hepatitis B vaccination is recommended for unvaccinated contact-sports players.
Keywords: Hepatitis B virus, Sports Medicine, Wrestling, DNA, Viral, Genotype, Hepatitis B, Japan, Phylogeny, young adult
Background
Hepatitis B virus (HBV) is a major global health concern. According to the World Health Organization (WHO), an estimated 257 million people are currently living with HBV infection [1]. The estimated prevalence of HBV is 0.20% in Japan [2]. HBV is spread through percutaneous or mucosal exposure to infected blood and various body fluids, sexual contact, contaminated needles, and vertical transmission from mother to child during delivery. To the best of our knowledge, there are no epidemiological reports of an increased prevalence of HBV infection among athletes who take part in contact sports. One study, conducted in South Australia, found no difference in the prevalence of HBV infection in soccer players when compared with a group of blood donors of the same age [3]. Similarly, in another study, no evidence of increased HBV or HCV transmission was noted among participants of Tehranian wrestling when compared with those participating in low- to moderate-contact sports [4].
The spread of hepatitis B vaccination has been slower in Japan than in other countries. Three cases of horizontal transmission of HBV in contact sports have been previously reported in Japan [5–7]. The American Medical Society for Sports Medicine (AMSSM) has issued an advisory to alert clinicians regarding the risk of transmission of blood-borne pathogens such as HBV by contact sports [8]. Here, we report 3 cases of horizontal HBV transmission among members of a wrestling club in Japan.
Case Reports
CASE 1:
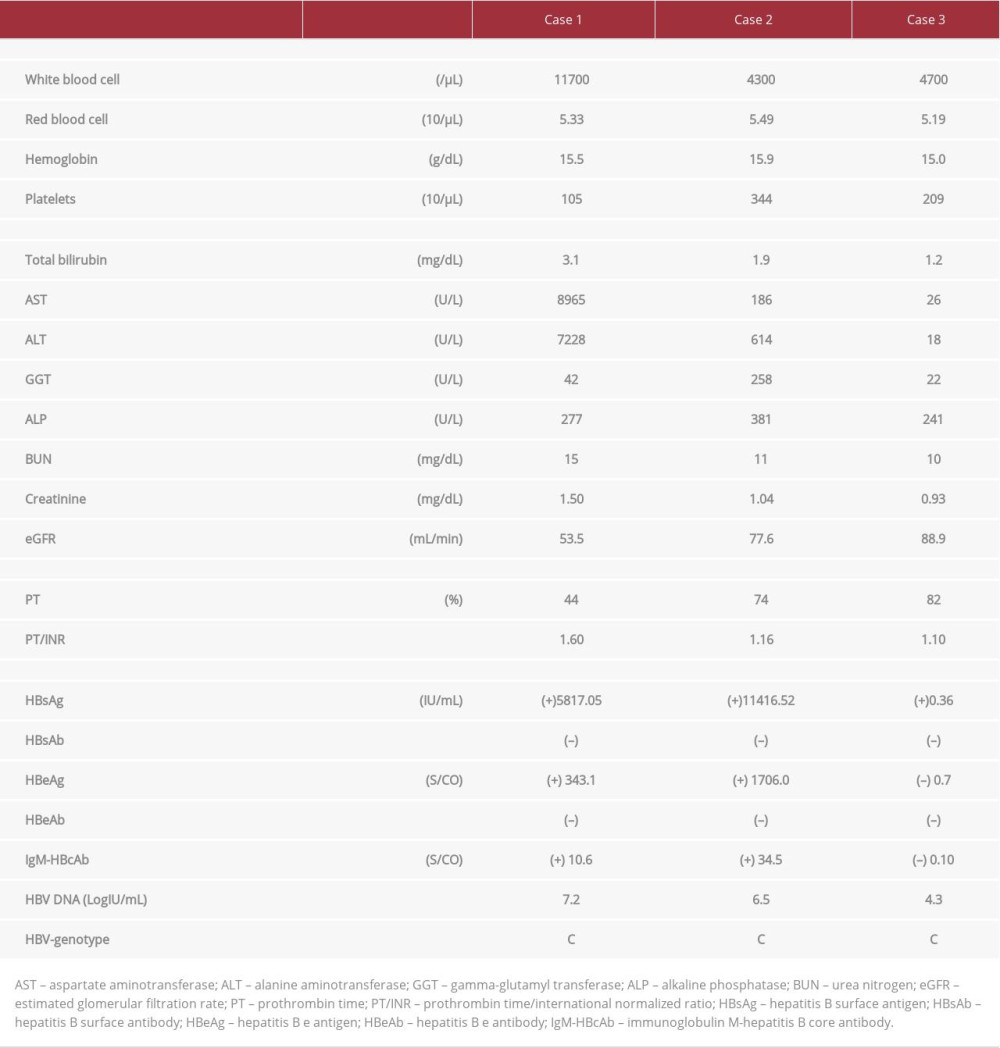
A 19-year-old male member of a wrestling club presented to our hospital with a fever of 38°C and malaise that had started a few days previously. He had no other significant medical history and no history of alcohol intake, injection drug use, or sexual activity with either men or women. In addition, neither he nor his family members had a history of HBV infection or were vaccinated against HBV. His physical findings were normal, except for his fever. Laboratory tests revealed elevated serum liver enzyme levels and an increased prothrombin time/international normalized ratio (PT/INR) (Table 1). The results were positive for both hepatitis B surface antigen (HBsAg) and HBV DNA (Table 1), and negative for serologic markers for hepatitis A, C, and E viruses, human immunodeficiency virus (HIV), syphilis, Epstein-Barr virus, and cytomegalovirus. Ultrasonography and contrast-enhanced computed tomography revealed no significant biliary tract disease that could have led to liver damage. The patient was therefore diagnosed with acute hepatitis B. Additional laboratory tests revealed the following: antibody to HBsAg (HBsAb) negative; hepatitis B e antigen (HBeAg) positive; antibody to HBeAg (HBeAb) negative; IgM-HBcAb positive; and HBV-genotype-C positive (Table 1). These additional test results supported our diagnosis. To prevent the spread of HBV infection, the patient was prohibited from participating at the wrestling club until after the disappearance of HBV DNA from his blood. His treatment was initiated on confirmation of HBV infection. Nucleotide analogue (NA) therapy for HBV with lamivudine and prednisolone (PSL), 50 mg/day (0.8 mg/kg/day); an intravenous glycyrrhizin-containing herbal medicine, Stronger Neo-Minophagen C (SNMC; Minophagen Pharmaceutical, Tokyo, Japan), 100 ml/day; and ursodeoxycho-late, 300 mg/day, were prescribed. Lamivudine was replaced with entecavir 4 weeks later to prevent tolerance. The patient demonstrated a good response, with restored liver enzyme levels and decreasing HBV DNA. Therefore, these drugs were gradually discontinued. He was discharged 17 days after hospital admission and was considered cured 19 weeks after the onset of symptoms. Because clearance of HBV DNA and HBsAb positivity was confirmed, he was permitted to resume training (Figure 1).
CASE 2:
A 21-year-old man, from the same wrestling club as the first patient, was referred to our hospital because of an incidental diagnosis of HBV infection on a screening test, five months after patient 1 was initially seen at our hospital. Nothing significant was noted in his past medical history. He was non-alcoholic, with no history of intravenous drug use or sexual activity with either men or women. In addition, neither he nor his family members had a history of HBV infection and they were not vaccinated against HBV. The clinical history revealed that he was a wrestling training partner of patient 1. In the practice of wrestling, abrasions accompanied by bleeding are common occurrences. In addition, there was no history of sexual contact with the other athlete. He was asymptomatic, and his physical findings were normal, but laboratory tests revealed elevated serum liver enzyme levels (Table 1). Serological markers were positive for HBsAg, HBeAg, IgM-HBcAb, and HBV DNA; and negative for hepatitis C virus, HIV, and syphilis (Table 1).
On follow-up, although his liver enzymes decreased, they did not normalize, and HBV DNA remained at a high level; therefore, we diagnosed the patient with chronic hepatitis B (Figure 1). He was transferred to another hospital; thus, no further follow-up information was available.
CASE 3:
A 20-year-old man from the same wrestling club as the first two athletes was referred to our hospital at the same time as patient 2, for an incidentally diagnosed HBV infection on a screening test. There was no other significant past history and he denied any alcohol intake, drug abuse, or sexual activity with other wrestling members. No family history of HBV infection was noted. Moreover, he had not been vaccinated against hepatitis B infection. He was asymptomatic, and his physical findings were normal. Laboratory tests showed normal serum liver enzyme levels, but his serologic markers were positive for HBsAg, HBV DNA, and negative for hepatitis C virus, HIV, and syphilis (Table 1).
On follow-up 3 weeks later, he was HBsAg negative and HBsAb positive and after 6 weeks he was HBV DNA negative, indicating that his acute HBV infection had resolved (Figure 1).
All three cases were HBV of genotype C, and the direct-sequence HBV DNA-based genetic test showed a 100% match for all 3215 bases of sequenced HBV DNA. Phylogenetic analysis of the DNA sequences classified all three isolates as subgeno-type C2, which is the most common HBV genotype reported in Japan (Figure 2). Subsequently, all members of the wrestling club, including 15 players, 2 equipment managers, and 4 coaches, were screened for HBV (HBsAg, HBsAb, HBcAb). None of them had evidence of current or past HBV infection. All of them got vaccinated against HBV immediately after the diagnosis of cases 2 and 3. After this, no further cases of HBV infection were observed.
Discussion
We have reported three cases of HBV infection among members of a wrestling club. Genetic testing revealed all three athletes to have an identical strain of HBV. Although they had contact with each other while practicing wrestling, no contact with a common partner outside the club was reported; therefore, we thought that this series of HBV infections could be caused by horizontal transmission within the wrestling club.
In adulthood, HBV is transmitted mainly by sexual contact or contaminated needles. These patients denied having any sexual contact with one another, any injection drug use, or any reuse of needles for procedures such as tattooing. Although it is not possible to rule-out the possibility that HBV was transmitted by one of these means, we consider it unlikely and consider it more likely that HBV was transmitted between these three men by another form of close contact. HBV can be detected not only in blood but also in body fluids such as sweat; therefore, people taking part in contact sports can be at risk of horizontal HBV transmission [8–12].
Although no epidemiological reports have indicated that athletes who take part in contact sports have a significantly higher prevalence of HBV infection [3,4], 3 previous case reports have shown HBV outbreaks among athletes who engage in contact sports, such as sumo wrestling and American football [5–7]. In all studies, the infections were presumed to have been transmitted horizontally from an index case to contacts via skin abrasions.
Wrestling has been classified as a high-contact sport, and previous reports have expressed concerns about the possibility of HBV transmission through bleeding wounds and sweating, similar to our cases [4,8]. No history of sexual or bleeding contact with acquaintances outside the club was noted. Therefore, each of these patients probably got infected through horizontal transmission within the wrestling club; however, it is difficult to identify the route of transmission. One possible explanation is that either the first or second athlete may have been infected by an HBV carrier who was not a member of the club; the athlete then likely spread HBV to his training partner. Subsequently, the second athlete then likely transmitted HBV to the third wrestler. The source of the infection is presumed to be from someone outside of the club for the following reasons: i) No members of the wrestling club had a history of HBV infection and ii) IgM-HBcAb was positive in Cases 1 and 2, suggesting acute HBV infection rather than acute-on-chronic infection [13]. The first patient was barred from training during the HBV incubation period experienced by patient 3, which is approximately 75 days on average, suggesting that patient 3 was infected by patient 2, and not patient 1. Alternatively, the possibility that patient 2 had chronic hepatitis and infected both patient 1 and patient 3 cannot be ruled out.
Despite the isolation of patient 1 from other members of the wrestling club, the other two athletes were infected. This suggests the importance of immediate HBV screening after an athlete has been diagnosed with HBV infection. Patient 2, the training partner of patient 1, would have already been infected before patient 1 was quarantined. Transmission of HBV from athlete 2 to athlete 3 could probably have been prevented if HBV screening had been performed immediately among the members of the wrestling club when athlete 1 was diagnosed.
HBV vaccination is highly effective at preventing HBV infection, and universal HBV immunization at birth and during infancy is the key strategy for global elimination of HBV infection. In 1992, the WHO recommended that all countries introduce HBV vaccination into national routine infant immunization programs [14]. However, in Japan, routine hepatitis B immunization during infancy was only introduced in 2016. None of the members of the wrestling club, including the 3 infected wrestlers, had been vaccinated against HBV during infancy. To prevent further spread of the infection, all members of the club were vaccinated.
Conclusions
HBV could be transmitted in contact sports through bleeding wounds and sweat. Therefore, vaccination against HBV is recommended for all unvaccinated contact sports players and players with low titers of HBsAb. In Japan, where the introduction of routine HBV vaccination has been delayed, voluntary vaccination should be recommended, especially to those at high risk of infection. If an athlete is diagnosed with HBV infection in an unvaccinated population, HBV screening of the whole population is advocated.
References:
1.. : World Health Organization Factsheets for Chronic Hepatitis B, 2019 https://www.who.int/news-room/fact-sheets/detail/hepatitis-b
2.. Tanaka J, Akita T, Ko K, Epidemiological Research Group on Viral Hepatitis and its Long-term Course, Ministry of Health, Labour and Welfare of Japan: Countermeasures against viral hepatitis B and C in Japan: An epidemiological point of view: Hepatol Res, 2019; 49(9); 990-1002
3.. Siebert DJ, Lindschau PB, Burrell CJ, Lack of evidence for significant hepatitis B transmission in Australian Rules Footballers: Med J Aust, 1995; 162(6); 312-13
4.. Kordi R, Neal K, Pourfathollah AA, Risk of hepatitis B and C infections in Tehranian wrestlers: J Athletic Training, 2011; 46(4); 445-50
5.. Kashiwagi S, Hayashi J, Ikematsu H, An outbreak of hepatitis B in members of a high school Sumo wrestling club: JAMA, 1982; 248(2); 213-14
6.. Tobe K, Matsuura K, Ogura T, Horizontal transmission of hepatitis B virus among players of an American football team: Arch Intern Med, 2000; 160(16); 2541-45
7.. Bae SK, Yatsuhashi H, Takahara I, Sequential occurrence of acute hepatitis B among members of a high school Sumo wrestling club: Hepatol Res, 2014; 44(10); 267-72
8.. McGrew C, MacCallum DS, Narducci D, AMSSM position statement update: Blood-borne pathogens in the context of sports participation: Clin J Sport Med, 2020; 54(4); 200-7
9.. Kidd-Ljunggren K, Holmberg A, Bläckberg J, Lindqvist B, High levels of hepatitis B virus DNA in body fluids from chronic carriers: J Hosp Infect, 2006; 64(4); 352-57
10.. Bereket-Yücel S, Risk of hepatitis B infections in Olympic wrestling: Br J Sports Med, 2007; 41(5); 306-10
11.. Komatsu H, Inui A, Sogo T, Tears from children with chronic hepatitis B virus (HBV) infection are infectious vehicles of HBV transmission: Experimental transmission of HBV by tears, using mice with chimeric human livers: J Infect Dis, 2012; 206(4); 478-85
12.. Sonderup MW, Suter J, Spearman CW, Hepatitis B in rugby: Is it time to revisit policy?: Br J Sports Med, 2016; 50(11); 645-46
13.. Park JW, Kwak KM, Kim SE, Differentiation of acute and chronic hepatitis B in IgM anti-HBc positive patients: World J Gastroenterol, 2015; 21(13); 3953-59
14.. , Implementation of newborn hepatitis B vaccination – worldwide, 2006: Morb Mortal Wkly Rep, 2008; 57(46); 1249-52
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133