06 October 2020: Articles ")
Successful Treatment of a Patient with Chronic Myelogenous Leukemia with Concurrent Janus Kinase 2 (JAK2) R795S Mutation and Breakpoint Cluster Region-ABL1 (BCR-ABL1) Fusion: A Case Report and Literature Review
Unusual clinical course
Yanhua Yue1ABCDEFG, Wei Wei1ABCDEF, Yanting Guo1B, Fei Wang1C, Weimin Dong1D, Yue Liu1B, Yan Lin1G, Yang Cao1G, Weiying Gu1ABCDEFG*DOI: 10.12659/AJCR.925151
Am J Case Rep 2020; 21:e925151






Abstract
BACKGROUND: Although the V617F mutation in the Janus kinase 2 (JAK2) gene and the breakpoint cluster region-abl1 (BCR-ABL1) oncogene fusion have been considered mutually exclusive in most myeloproliferative neoplasms (MPNs), many recent studies have described patients with both. This report describes a patient with chronic myelogenous leukemia (CML) and the unusual JAK2 R795S mutation and reviews 23 additional patients with JAK2 gene mutations coexisting with myelofibrosis (MF) and CML.
CASE REPORT: A 50-year-old woman with MF experienced rapid disease progression 3 weeks later, accompanied by severe abdominal pain and a white blood cell count of 257.45×10⁹/l. Karyotype analysis indicated that she was 46, XY, Philadelphia (Ph) (+) and BCR-ABL1 positive. Bone marrow aspiration after 1 cycle of chemotherapy and treatment with dasatinib showed that her marrow was hypercellular, with an increased number of megakaryocytes and 48.5% myeloblasts expressing the myeloid antigens CD33, CD13, CD34, CD117, and CD71. Next-generation sequencing identified a rare JAK2 R795S mutation. She was diagnosed with CML in blast phase, and was successfully treated with allogeneic hematopoietic stem cell transplantation (allo-HSCT).
CONCLUSIONS: JAK2 gene mutations, including the rare JAK2 R795S mutation, can coexist with BCR-ABL1 in patients with MPNs. The clinical course of MPN in patients with both BCR-ABL1 and JAK2 mutations may be different from that in patients with classical MPNs.
Keywords: Janus Kinase 2, Leukemia, Myelogenous, Chronic, BCR-ABL Positive, myelofibrosis, Mutation, myeloproliferative disorders, primary myelofibrosis
Background
Myeloproliferative neoplasms (MPNs) are clonal disorders characterized by proliferation of hematopoietic stem cells. Major genetic aberrations include the breakpoint cluster region-abl 1 (BCR-ABL1) fusion gene in patients with Philadelphia (Ph) chromosome-positive chronic myelogenous leukemia (CML) and mutations in the Janus kinase 2 (JAK2), thrombopoietin receptor MPL (MPL), and calreticulin (CALR) genes in patients with Ph chromosome-negative MPN. Since the first report of the absence of JAK2 V617F in patients with Ph+ CML [1], BCR-ABL1 and JAK2 gene mutation were thought to be mutually exclusive. To date, however, more than 20 BCR-ABL1-positive patients with myelofibrosis (MF) and CML have been reported to have JAK2 gene mutations, with the majority having JAK2 V617F mutations. It is not clear whether the characteristics of patients with concurrent JAK2 gene mutations and BCR-ABL1 differ from those of other patients with MPNs.
This report describes a patient in CML blast phase (CML-BP) who originally presented with MF and was positive for both the BCR-ABL1 oncogene and a rare JAK2 R795S mutation. This patient was effectively treated with allogeneic hematopoietic stem cell transplantation (allo-HSCT). To our knowledge, this is the first such CML patient positive for BCR-ABL1 with a JAK2 R795S mutation. This study also summarized the clinical and laboratory features of an additional 23 patients with concurrent BCR-ABL1-positive CML and JAK2 gene mutations positive MF.
Case Report
LITERATURE REVIEW RESULTS:
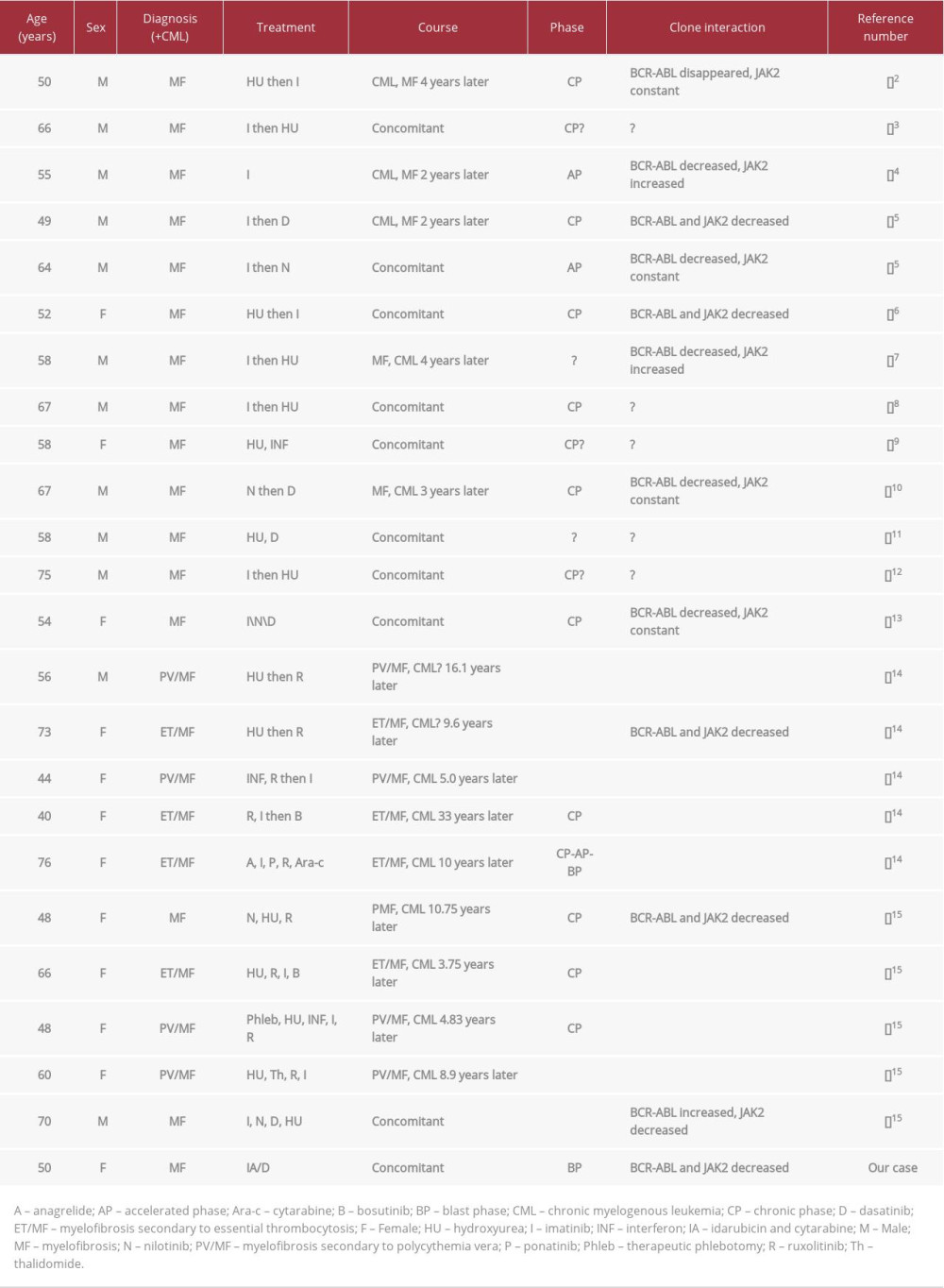
To date, JAK2 R795S has not yet been reported in patients with MF, polycythemia vera (PV), or any other hematologic or other diseases. A single-nucleotide polymorphism (SNP) was ruled out. A literature review identified 23 other patients with MF and CML who were found to have both BCR-ABL1 trans-locations and concomitant JAK2 gene mutations since 2005. The characteristics of these 24 patients, including ours, are shown in Table 1 [2–15]. The other 23 patients all had the JAK2 V617F mutation. MF preceded CML in 11 patients, CML preceded MF in 3, and both were diagnosed concomitantly in 10. Interestingly, when MF preceded CML, the mean time between the 2 entities was 9.9 years, but when CML preceded MF, the mean time was 2.67 years. The changes in JAK2 gene mutation and BCR-ABL1 transcript levels varied. JAK2 gene mutation and BCR-ABL1 levels moved in opposite directions in 3 patients. JAK2 gene mutation level decreased or remained constant while BCR-ABL1 levels declined in another 9 patients. Our patient remained positive for BCR-ABL1 after the JAK2 gene mutation disappeared. Changes in JAK2 gene mutations and BCR-ABL1 levels were not reported for the other patients. Twenty-one patients were administered tyrosine kinase inhibitor (TKI) therapy, with most showing reductions in BCR-ABL1 levels. JAK2 gene mutation levels were reduced in 2 patients treated with ruxolitinib. At the outset, most of the 24 patients were in CML chronic phase, with only 2 in CML accelerated phase. Our patient was in CML-BP and was the only patient among the 24 to undergo allo-HSCT.
Discussion
To date, dozens of patients have been reported with concomitant JAK2 gene mutations and BCR-ABL1 translocation, accounting for 2.55% of patients with CML and 0.2–0.4% of those with MPNs [15–17]. Because of their relative rarity, management of this patient subgroup remains challenging. This report describes a patient with CML-BP who had a rare JAK2 R795S mutation and was BCR-ABL1 positive. The findings in this patient, along with findings in previous patients, may increase understanding of the clinical presentation, method of diagnosis, and treatments of this unusual condition.
Within 1 year, the mild anemia and normal spleen in our patient progressed to CML-BP with conspicuous fibrosis. Although a subgroup of Ph+-CML mimics ET or primary MF by presenting with marked thrombocytosis or myelofibrosis, concomitant JAK2 gene mutations and BCR-ABL1 are rare. Although results suggested that the presence of the JAK2V617F mutation in CML may be associated with early disease progression [18], that study included few patients. The JAK2 R795S mutation disappeared when our patient achieved CR based on bone marrow cell morphology, suggesting that this mutation may be associated with the early presentation of myelofibrosis and may have contributed to the rapid progression to CML-BP.
JAK2 V617F is the most common mutation site in MPNs. The JAK2 R795S mutation results in the replacement of argi-nine by serine. Whole-exome sequencing showed that this patient was negative for the JAK2 R795S mutation after 2 cycles of the IA regimen and dasatinib, whereas quantitative RT-PCR showed that this patient was positive for BCR-ABL1. These 2 gene abnormalities may have derived from different progenitor cell clones or the JAK2 clone may have been a subclone of the BCR-ABL1 clone. Alternatively, the JAK2 R795S mutation may have been below the analytical sensitivity of whole-exome sequencing. The review of the 24 patients with concomitant JAK2 gene mutations and BCR-ABL1 translocations found no common pattern for their origin, with some studies reporting that these anomalies originated from 2 independent clones and others reporting that one was a subclone of the other.
Currently, there is no uniform standard on the treatment of MPN patients with both JAK2 gene mutations and BCR-ABL1 translocation. TKIs are the major treatment options for these patients. If TKIs alone are not sufficiently effective, they can be combined with other regimens, such as Hu, INF, ruxolitinib, and chemotherapy. The combination of ruxolitinib and dasatinib was reported safe and effective in the treatment of a patient with concomitant PV and CML [19]. A multi-institutional study of a JAK2 V617F+ BCR–ABL1+ CML accelerated phase patient found that both JAK2 V617F and BCR–ABL1 were negative after allo-HSCT [15]. Similarly, JAK2 R795S and BCR-ABL1 disappeared in our patient after allo-HSCT. At present, our patient is still in CR. Most of the 24 patients were diagnosed in chronic stage and could be controlled with TKI or combination therapy. Allo-HSCT was feasible if the disease progressed.
Conclusions
JAK2 gene mutations, including JAK2 R795S, can coexist with the BCR-ABL1 translocation in MPNs. The clinical course of MPN patients with both anomalies may differ from that in patients with classic MPNs.
Figures
References:
1.. Jelinek J, Oki Y, Gharibyan V, JAK2 mutation 1849G>T is rare in acute leukemias but can be found in CMML, Philadelphia chromosome-negative CML, and megakaryocytic leukemia: Blood, 2005; 106(10); 3370-73
2.. Krämer A, Reiter A, Kruth J, JAK2-V617F mutation in a patient with Philadelphia-chromosome-positive chronic myeloid leukaemia: Lancet Oncol, 2007; 8(7); 658-60
3.. Bornhäuser M, Mohr B, Oelschlaegel U, Concurrent JAK2(V617F) mutation and BCR-ABL translocation within committed myeloid progenitors in myelofibrosis: Leukemia, 2007; 21(8); 1824-26
4.. Hussein K, Bock O, Seegers A, Myelofibrosis evolving during imatinib treatment of a chronic myeloproliferative disease with coexisting BCR-ABL translocation and JAK2V617F mutation: Blood, 2007; 109(9); 4106-7
5.. Kim YK, Shin MG, Kim HR, Simultaneous occurrence of the JAK2V617F mutation and BCR-ABL gene rearrangement in patients with chronic myeloproliferative disorders: Leuk Res, 2008; 32(6); 993-95
6.. de Conchon MRM, Costa JL, Novaes MMY, Simultaneous detection of JAK2 V617F mutation and Bcr-Abl translocation in a patient with chronic myelogenous leukemia: Int J Hematol, 2008; 88(2); 243-45
7.. Jallades L, Hayette S, Tigaud I, Emergence of therapy-unrelated CML on a background of BCR-ABL-negative JAK2V617F-positive chronic idiopathic myelofibrosis: Leuk Res, 2008; 32(1); 1608-10
8.. Pardini S, Fozza C, Contini S, A case of coexistence between JAK2V617F and BCR/ABL: Eur J Haematol, 2008; 81(1); 75-76
9.. Hussein K, Bock O, Theophile K, Chronic myeloproliferative diseases with concurrent BCR-ABL junction and JAK2V617F mutation: Leukemia, 2008; 22(5); 1059-62
10.. Yamada O, Mahfoudhi E, Plo I, Emergence of a BCR-ABL translocation in a patient with the JAK2V617F mutation: Evidence for secondary acquisition of BCR-ABL in the JAK2V617F clone: J Clin Oncol, 2014; 32(21); e76-79
11.. Park SH, Chi HS, Cho YU, Two cases of myeloproliferative neoplasm with a concurrent JAK2 (V617F) mutation and BCR/ABL translocation without chronic myelogenous leukemia phenotype acquisition during hydroxyurea treatment: Ann Lab Med, 2013; 33(3); 229-32
12.. Bader G, Dreiling B, Concurrent JAK2-positive myeloproliferative disorder and chronic myelogenous leukemia: A novel entity? A case report with review of the literature: J Investig Med High Impact Case Rep, 2019; 7; 2324709619832322
13.. Cheng HC, Zhao X, Li W, [JAK2 positive chronic myeloid leukemia complicated with suspected BCR-ABL variant: One case report]: Zhonghua Xue Ye Xue Za Zhi, 2018; 39(3); 254 [in Chinese]
14.. Boddu P, Chihara D, Masarova L, The co-occurrence of driver mutations in chronic myeloproliferative neoplasms: Ann Hematol, 2018; 97(11); 2071-80
15.. Soderquist CR, Ewalt MD, Czuchlewski DR, Myeloproliferative neoplasms with concurrent BCR-ABL1 translocation and JAK2 V617F mutation: A multi-institutional study from the bone marrow pathology group: Mod Pathol, 2018; 31(5); 690-704
16.. Pieri L, Spolverini A, Scappini B, Concomitant occurrence of BCR-ABL and JAK2V617F mutation: Blood, 2011; 118(12); 3445-46
17.. Martin-Cabrera P, Haferlach C, Kern W, BCR-ABL1-positive and JAK2 V617F-positive clones in 23 patients with both aberrations reveal biologic and clinical importance: Br J Haematol, 2016; 176(1); 135-39
18.. Pahore ZA, Shamsi TS, Taj M, JAK2V617F mutation in chronic myeloid leukemia predicts early disease progression: J Coll Physicians Surg Pak, 2011; 21(8); 472-75
19.. Zhou A, Knoche EM, Engle EK, Concomitant JAK2 V617F-positive polycythemia vera and BCR-ABL-positive chronic myelogenous leukemia treated with ruxolitinib and dasatinib: Blood Cancer J, 2015; 5(10); e351
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133