25 October 2020: Articles 
A Case of a Newborn Baby Girl Infected with SARS-CoV-2 Due to Transplacental Viral Transmission
Unusual clinical course
Nicole Majachani1E*, Jean Luc M. Francois1E, Ashen K. Fernando1E, Jamshed Zuberi2EDOI: 10.12659/AJCR.925766
Am J Case Rep 2020; 21:e925766






Abstract
BACKGROUND: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a highly infectious virus and is responsible for the current pandemic. It mainly infects cells of the lower respiratory tract and has been linked to severe respiratory complications. Although multiple routes of transmission have been reported in the literature, there is no definitive evidence for transplacental transmission. We present a case of neonatal SARS-CoV-2 likely due to transplacental transmission.
CASE REPORT: 31-year-old Hispanic woman in the final week of pregnancy developed mild respiratory symptoms of COVID-19 pneumonia and tested positive for SARS-CoV-2 infection. She had a history of Human immunodeficiency virus (HIV) infection and gestational diabetes. Two days later, she gave birth to a baby girl who tested positive for SARS-CoV-2 on the first day after birth. She was delivered via elective cesarean section adhering to a strict infection control protocol.
CONCLUSIONS: This report presents a case of a 31-year-old mother with mild symptoms of COVID-19 pneumonia who was positive for SARS-CoV-2 infection and who gave birth to a baby girl who was also positive for SARS-CoV-2. This case supports the possibility of transplacental transmission of SARS-CoV-2.
Keywords: Neonatology, Pediatrics, SARS Virus, Pregnancy, Virus Diseases, COVID-19, Coronavirus Infections, Betacoronavirus, COVID-19, Cesarean Section, Disease Transmission, Infectious, Infant, Newborn, Pandemics, Pneumonia, Viral, Pregnancy Complications, Infectious, SARS-CoV-2
Background
Systemic acute respiratory syndrome coronavirus 2 (SARSCoV-2) is a highly infectious virus from the
In response to the potential risks to both the mother and fetus, the American College of Obstetricians and Gynecologists, the American Academy of Pediatrics, and the Centers for Disease Control have developed guidelines which provide a framework for detecting infections early and preventing potential transmission of SARS-CoV-2. Pregnant women admitted for suspected SARS-CoV-2 or who develop symptoms during admission are isolated and should be prioritized for testing [4,5]. Furthermore, delivery should be performed in a negative-pressure isolation ward whenever possible, with strict precautionary measures to reduce the risk of droplet transmission [6,7]. Neonates born to mothers infected with SARS-CoV-2 should be screened at 24 and 48 h of age using nasopharyngeal swabs for polymerase chain reaction (PCR) analysis. Any positive result requires repeated testing at 48- to 72-h intervals until there are 2 consecutive negative results [6]. Furthermore, asymptomatic infants with positive or pending SARS-CoV-2 tests may be discharged home with plans of outpatient observation through 14 days after birth [6]. Clinical staff caring for the mother and infant should use droplet and contact precautions, including the use of personal protective equipment such as gown, gloves, eye protection, and standard surgical mask [4–7] in addition to separating the mother and newborn to minimize the risk of postnatal infection [6,7].
Case Report
A 1-day-old Hispanic girl was born via elective cesarean section at 34 weeks due to oligohydramnios and maternal history of eclampsia. Her mother was a 31-year-old G2P2 woman with a past medical history of HIV and type A2 gestational diabetes. Two days prior to giving birth, her mother tested positive for SARS-COV-2 via nasopharyngeal swab PCR after experiencing shortness of breath and myalgia. Upon admission to the hospital, initial laboratory studies revealed a white blood cell count (WBC) of 10 000 cells/mm3 (Table 1) and a chest X-ray showed bibasilar opacities, supporting her diagnosis of SARS-CoV-2 (Figure 1).
Initial examination of the neonate was normal and the Apgar score was 9/10 at 1 and 5 mins. Vital signs were within normal limits and a complete blood count revealed a normal WBC of 9000 cells/mm3 (Table 2). Due to the above circumstances, the patient was admitted to the Neonatal Intensive Care Unit (NICU) for hypoglycemia monitoring and continuous cardiac, respiratory, and pulse oximetry monitoring. The patient was also started on prophylactic oral zidovudine.
As per guidelines, the neonate was tested for SARS-COV-2 at 24 h of age via nasopharyngeal swab with the Becton-Dickinson (BD MAX) automated polymerase chain reaction system (Becton-Dickinson, Franklin Lakes, NJ, USA), which yielded a positive result. At the time, the patient’s lungs were clear to auscultation bilaterally with no signs of respiratory distress and 95% oxygen saturation on room air. She continued to be monitored for any signs of respiratory deterioration.
Over the next 10 days, the patient continued to be monitored and remained asymptomatic. Laboratory results remained within normal limits, and testing for SARS-CoV-2 remained positive when repeated at 48 h and at 7 days of age.
She continued to feed well and grow appropriately during her stay. No imaging studies were required and she was subsequently discharged from the NICU on day 10 with instructions for follow-up in 2 weeks.
Discussion
Vertical transmission is the passage of infectious agents from an infected mother to her offspring. This may occur across the placenta, through breastmilk, or from direct contact during or after birth [8]. Concerning transplacental vertical transmission, disease-causing organisms overcome the protective barrier to infect the offspring during the antenatal, perinatal, or postnatal periods of gestation [8]. The result often increases fetal morbidity and mortality from complications like organ injury, morphological abnormalities, intrauterine growth restriction, and intrauterine fetal demise [9]. As a result, trimester-specific pregnancy screenings are done for infections with known vertical transmission. These include Parvovirus, Human immunodeficiency virus, Zika, Varicella-zoster, Rubella, Cytomegalovirus, and Toxoplasmosis [8,9]. Due to the novelty of SARS-CoV-2, there is insufficient evidence on transplacental transmission of this virus. Nonetheless, there are proposed mechanisms by which it may take place.
Understanding the structure and function of the placenta is essential when considering mechanisms of transplacental transmission. The placenta is the interface between the maternal and fetal circulatory systems and is composed of fetal-derived progenitor cells which differentiate into cytotrophoblasts and syncytiotrophoblasts [8]. It is needed for fetal nourishment and protection against pathogens that may be present in the maternal circulation. It is believed that the syncytiotropho-blast layer confers a broad non-specific resistance to microbial infections [8]. However, some pathogens are able to overcome this barrier through unique mechanisms. For instance, the Zika virus, which causes congenital microcephaly, may be able to penetrate the placenta due to its ability to infect different cells of the placenta as well as cells of the maternal immune system [8].
With regards to transplacental transmission of SARS-CoV-2, it is essential to understand how the virus infects cells of the body. SARS-CoV-2 infects host cells by binding to angiotensin-converting enzyme 2 (ACE2), a membrane-bound aminopeptidase [10,11]. This leads to receptor-mediated endocytosis of the virus, which is necessary for replication [11]. While ACE2 is predominantly expressed in the heart, lungs, kidneys, and gastrointestinal tract, recent studies uncovered ACE2 expression in various placental tissues and fetal organs [10–12]. While this expression is low in early gestational ages, it increases significantly in later stages of pregnancy [11], thereby increasing the risk of fetal infection. Although similar viruses like severe acute respiratory syndrome coronavirus 1 have not demonstrated the ability to cause fetal infection, SARS-CoV-2 is able to bind ACE2 with much higher affinity [11], thus increasing the probability of transplacental transmission.
While the presence of ACE2 in the placenta provides a plausible mechanism for transplacental transmission, only 3 studies have found evidence in support of its occurrence. Dong et al. described a case of a newborn that tested positive for anti-SARS-CoV-2 immunoglobulin M (IgM) 2 h after birth [13]. This class of antibody dominates the early phase of infection and is unable to cross the placenta. Although this neonate tested negative for SARS-CoV-2, the positive IgM antibodies suggest an immune response of fetal origin. Furthermore, intrapartum exposure was unlikely to be the cause since IgM may take up to 3 to 7 days to be detectable [13]. Additionally, other studies detected SARS-CoV-2 in placental tissue using electron microscopy and PCR [14,15]. This provides evidence that SARS-CoV-2 is able to infect the placenta and possibly cause fetal infection.
However, in a recent study, researchers were unable to detect viral particles in products of conception from infected mothers [16]. Furthermore, all babies born to these mothers tested negative for SARS-CoV-2. These findings suggest that, in most cases, the placenta is able to protect the fetus from SARS-CoV-2 infection. This also explains the paucity of reported cases suspicious for transplacental transmission of SARSCoV-2. At this time, the literature identifies 3 other cases of neonates testing positive for SARS-CoV-2 as early as 16 h after birth from infected mothers [17]. Similar to our case, a strict infection control protocol was followed and the babies were delivered via cesarean section. Although no products of conception in these cases were tested for viral particles, the positive PCR results within the first 24 h and strict infection control protocol make transplacental transmission more likely than peripartum transmission.
Conclusions
We presented the case of a 31-year-old mother with mild symptoms of COVID-19 pneumonia who was positive for SARS-CoV-2 infection and who gave birth to a baby girl who was also positive for SARS-CoV-2. This case supports the possibility of trans-placental transmission of SARS-CoV-2. SARS-CoV-2 can likely overcome the placental barrier though its high affinity for ACE-2 expressed in the placenta and fetal organs. This is supported by the detection of SARS-CoV-2 in placental tissue and fetal IgM titers. However, there are few cases suspicious for transplacental SARS-COV-2 transmission, suggesting that the placenta can protect the fetus of an infected mother in most cases. Despite limited evidence, when a strict infection control protocol is followed during delivery, a positive SARS-CoV-2 test in a neonate is likely due to transplacental transmission.
References:
1. Wang S, Guo L, Chen L, A case report of neonatal COVID-19 infection in China.: Clin Infect Dis, 2020; 71(15); 853-57
2. Di Mascio D, Khalil A, Saccone G, Outcome of Coronavirus spectrum infections (SARS, MERS, COVID 1–19) during pregnancy: A systematic review and meta-analysis: Am J Obstet Gynecol MFM, 2020; 2(2); 100107
3. Jayaweera M, Perera H, Gunawardana B, Manatunge J, Transmission of COVID-19 virus by droplets and aerosols: A critical review on the unresolved dichotomy: Environ Res, 2020; 188; 109819
4. , Practice advisory: novel coronavirus 2019 (COVID-19);, 2020
5. , Interim considerations for infection prevention and control of coronavirus disease 2019 (COVID-19) in inpatient obstetrics healthcare settings., 2020, Centers of Disease Control
6. Puopolo KM, Hudak ML, Kimberlin DW, Cumming J, Initial guidance: Management of infants born to mothers with COVID-19, 2020
7. Chen D, Yang H, Cao Y, Expert consensus for managing pregnant women and neonates born to mothers with suspected or confirmed novel coronavirus (COVID-19) infection [Corrected and republished in: Int J Gynaecol Obstet. 2020 Jul;150(1): 136]: Int J Gynaecol Obstet, 2020; 149(2); 130-36
8. Arora N, Sadovsky Y, Dermody TS, Coyne CB, Microbial vertical transmission during human pregnancy: Cell Host Microbe, 2017; 21; 561-67
9. Longo S, Borghesi A, Tzialla C, Stronati M, IUGR and infections: Early Hum Dev, 2014; 90(Suppl. 1); S42-44
10. Dashraath P, Wong JLJ, Lim MXK, Coronavirus disease 2019 (COVID-19) pandemic and pregnancy: Am J Obstet Gynecol, 2020; 222; 521-31
11. Li M, Chen L, Zhang J, The SARS-CoV-2 receptor ACE2 expression of maternal-fetal interface and fetal organs by single-cell transcriptome study: PLoS One, 2020; 15; e0230295
12. Egloff C, Vauloup-Fellous C, Picone O, Evidence and possible mechanisms of rare maternal-fetal transmission of SARS-CoV-2: J Clin Virol, 2020; 128; 104447
13. Dong L, Tian J, He S, Possible vertical transmission of SARS-CoV-2 from an infected mother to her newborn: JAMA, 2020; 323(18); 1846-48
14. Algarroba GN, Rekawek P, Vahanian SA, Visualization of severe acute respiratory syndrome coronavirus 2 invading the human placenta using electron microscopy: Am J Obstet Gynecol, 2020; 223(2); 275-78
15. Penfield CA, Brubaker SG, Limaye MA, Detection of SARS-COV-2 in placental and fetal membrane samples: Am J Obstet Gynecol MFM, 2020; 2(3); 100133
16. Chen H, Guo J, Wang C, Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: A retrospective review of medical records [Corrected and republished from: Lancet. 2020; 395(10226): 809–15].: Lancet, 2020; 395(10229); 1038
17. Zeng L, Xia S, Yuan W, Neonatal early-onset infection with SARS-CoV-2 in 33 neonates born to mothers with COVID-19 in Wuhan, China: JAMA Pediatr, 2020; 174(7); 722-25
Tables
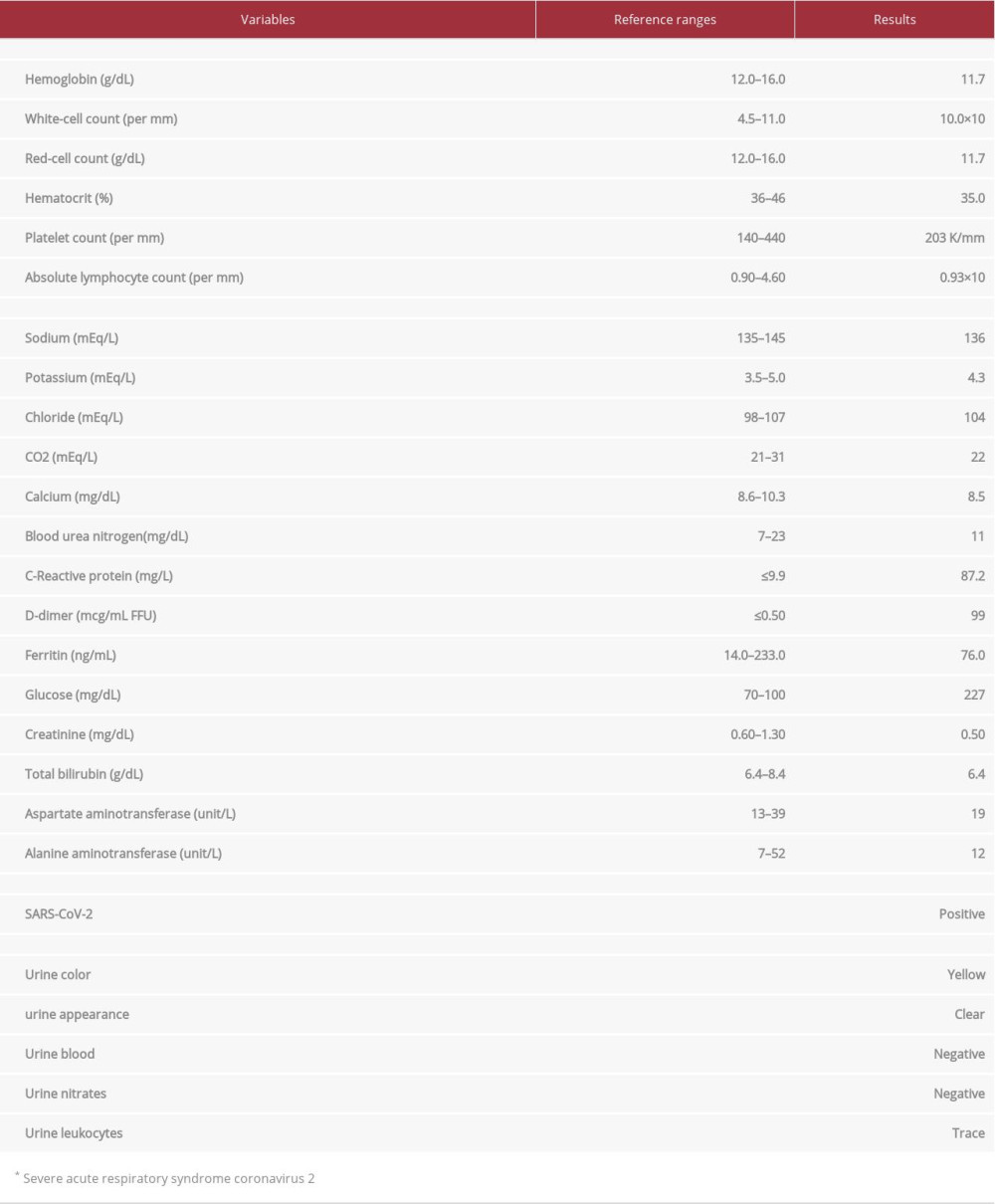 Table 1.. The results of the laboratory investigations of a 31-year-old woman 2 days before giving birth.
Table 1.. The results of the laboratory investigations of a 31-year-old woman 2 days before giving birth.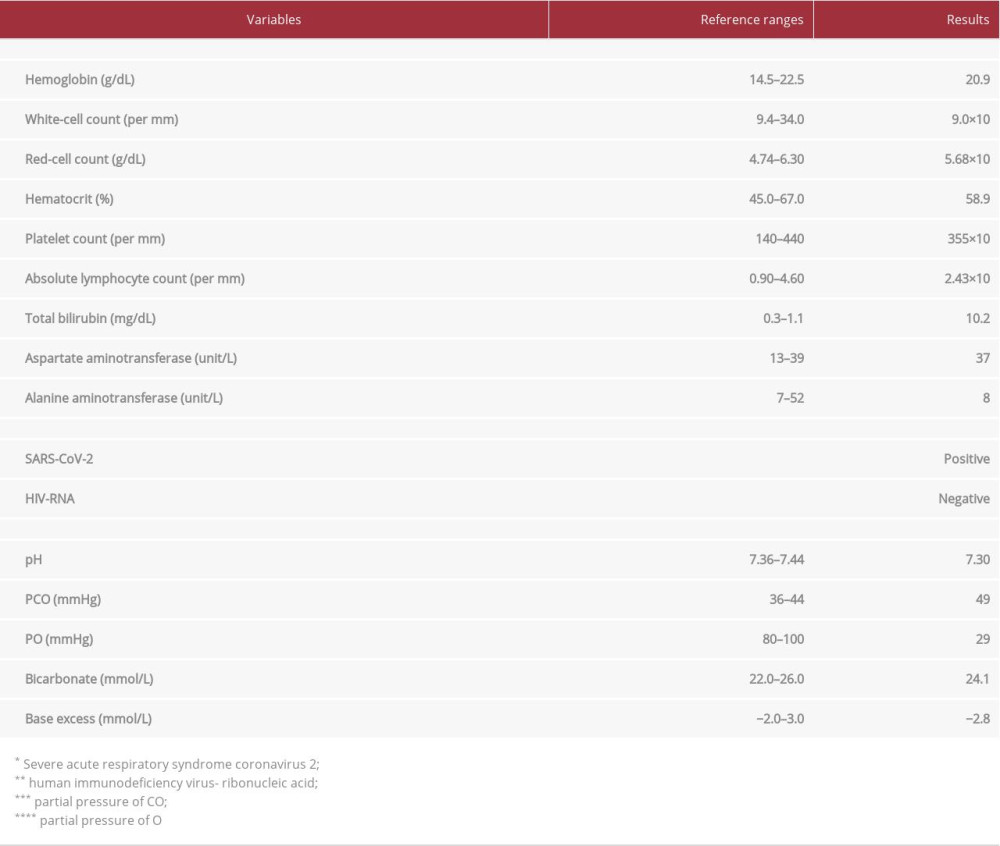 Table 2.. The results of the laboratory investigations of a baby girl on the first day of birth.Table 1.. The results of the laboratory investigations of a 31-year-old woman 2 days before giving birth.Table 2.. The results of the laboratory investigations of a baby girl on the first day of birth.
Table 2.. The results of the laboratory investigations of a baby girl on the first day of birth.Table 1.. The results of the laboratory investigations of a 31-year-old woman 2 days before giving birth.Table 2.. The results of the laboratory investigations of a baby girl on the first day of birth. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133