05 October 2020: Articles 
Use of Nitrous Oxide to Facilitate Induction for Electroconvulsive Therapy: A Case Report
Unusual or unexpected effect of treatment
Kevin Lee1BCDEF, Tanaya Sparkle1BCDEF*DOI: 10.12659/AJCR.925883
Am J Case Rep 2020; 21:e925883






Abstract
BACKGROUND: The choice of pharmacologic agents used for electroconvulsive therapy (ECT) is critical as this can affect seizure duration and, ultimately, the effectiveness of ECT for the underlying condition. We report the use of nitrous oxide (N2O) to sedate and place an intravenous (IV) catheter in a combative patient for the induction of anesthesia. We found no significant clinical effect on seizure duration while using N2O in the pre- and intra-procedural period.
CASE REPORT: We present the case of a 48-year-old woman with a history of major depressive disorder scheduled for electroconvulsive therapy (ECT). We used 50% nitrous oxide (N2O) to sedate her and facilitate the placement of a 22-gauge IV catheter. When IV access was established, induction of anesthesia was done with 80 mg of methohexital, which was later switched to 16 mg of etomidate and 80 mg of succinylcholine. After multiple ECT treatments, we observed no significant clinical effect on seizure duration while using N2O when home medications were optimized. There is limited literature on the use of N2O as a sedative agent in the perioperative period with other agents known to have no effect or beneficial effect on ECT treatments. We found no studies assessing the effect of N2O on seizure duration.
CONCLUSIONS: Considering the pleasant odor, independent antidepressant activity, vasodilatory effect, low blood-gas partition coefficient, and minimal effect on respiration, N2O may serve as the ideal adjunct to intravenous induction of anesthesia in an uncooperative or anxious patient. Further studies are warranted to confirm the efficacy and the safety of N2O for use during ECT.
Keywords: Electroconvulsive Therapy, Nitrous Oxide, Receptors, N-Methyl-D-Aspartate, Anesthetics, Intravenous, Depressive Disorder, Major, Methohexital
Background
Electroconvulsive therapy (ECT) is a well-established treatment in the field of psychiatry for conditions such as treatment-resistant major depressive disorder, catatonia, mania, and schizophrenia. ECT involves an electrically induced seizure, ideally lasting more than 30 s. To induce a seizure, 70 to 120 volts of pulsed electricity is used unilaterally or bilaterally [1]. Anesthesia is provided during ECT for sedation and muscle relaxation. However, the choice of anesthetic agents for sedation is critical as it can affect the seizure quality, seizure duration, and post-procedure course. There is limited literature on use of nitrous oxide (N2O) as an adjunct anesthetic agent in the perioperative period for ECT.
We present the case of a 48-year-old woman with a history of major depressive disorder with severe psychotic (catatonic) features scheduled for ECT, in whom N2O was used to facilitate the placement of an intravenous catheter. We noted no significant decrease in seizure duration after optimizing the patient’s home and induction medications. This report adheres to the applicable EQUATOR guidelines and the Institutional Review Board (IRB) guidelines. HIPAA consent was obtained from the patient’s daughter to publish this case report.
Case Report
The patient was a 48-year-old woman with a history of mild cerebral palsy, postural orthostatic tachycardia syndrome, gastric esophageal reflux disease, and rheumatoid arthritis disease who presented with worsening symptoms of major depressive disorder. She was scheduled to undergo ECT sessions. Her home medications included lorazepam 0.5 mg 3 times a day and mirtazapine 7.5 mg daily. Before presenting to our hospital, the patient displayed symptoms of depression, loss of appetite, aggression towards others, trichotillomania, and self-harming behavior. Her symptoms were worsening over time and did not respond to oral medications. The results of testing for organic neuropsychiatric conditions such as autoimmune encephalitis and drug-related psychosis were negative.
The patient’s ECT treatments were performed using MECTA spectrum 5000 bilateral ECT with brief pulse. MECTA settings for the stimulus for all of the patient’s ECT treatments were the following: pulse width 1.0 meter per s, frequency 60 hertz, duration 6.0 s, and amplitude 0.8 meters. The initial seizure threshold was established by titration-threshold dosing. Motor seizure activity was observed, followed by seizure activity confirmed via EEG monitoring.
For her first 2 ECT sessions, physical restraints were required to obtain intravenous access, after which general anesthesia was induced with weight-based methohexital and succinylcholine. Due to the risks associated with bodily restraints, a decision was made to use N2O in her future sessions. A mask was used to deliver 50% N2O with 50% oxygen. A 22-gauge intravenous catheter was placed in the right hand as soon as adequate sedation was achieved. N2O was shut off, and 100% oxygen was used for the remainder of the procedure. We intravenously administered 80 mg of methohexital and 80 mg of succinylcholine for the procedure. The patient’s ventilation was managed with mask ventilation by the anesthesia provider.
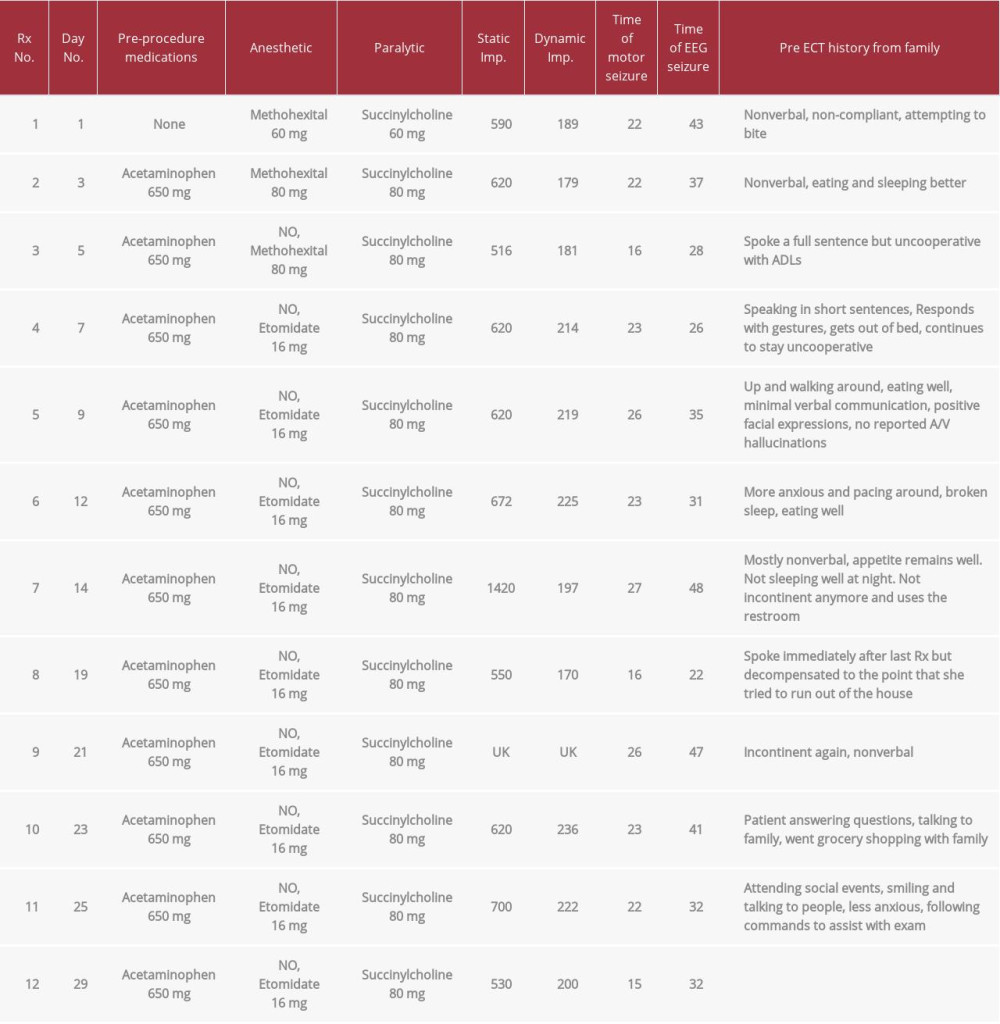
The electroencephalogram (EEG) seizure duration lasted 28 s, which was shorter than her previous EEG seizure durations of 43 s and 37 s, respectively. For her fourth ECT, 16 mg of etomi-date was used instead of methohexital. This treatment session resulted in an inadequate seizure duration of 26 s. Adequate seizure durations (>30 s) were obtained with subsequent ECT procedures after the discontinuation of her home medication, lorazepam. Based on the values in Table 1, N2O did not seem to have a clinically significant effect on EEG seizure duration when other medications and adjuvant anesthetic agents were optimized. With successive ECT treatments, the patient’s clinical and functional status greatly improved compared to pharmacologic therapy alone, as seen in Table 1. Prior to the patient’s initial treatment, she was nonverbal, uncooperative, and combative; however, after treatments 4–6, she began to speak in short sentences and was able to express herself. By treatments 10 and 11, she continued to be able to answer questions and by then was able to attend social events. Of note, care was provided by different anesthesia providers with varying levels of experience during each treatment, making it challenging to account for any differences in ventilatory strategy.
Discussion
Anesthetic agents such as muscle relaxants and anxiolytics were trialed in the mid-1900s to mitigate some of the musculoskeletal and psychological complications associated with ECT [2,3]. Historically, 35% of patients have fractured vertebrae during ECT done without muscle relaxants. The adjuvant use of short-term paralytics such as succinylcholine by the anesthesia provider has greatly decreased fracture rates while simultaneously minimizing residual paralysis in the post-anesthesia care unit. In fact, Luccarelli, Henry, and McCoy noted a fracture rate of 3.56 per 1 million treatments in their study [4].
Over time, the drugs used have changed, and the complications due to ECT have decreased significantly. Among the commonly used anesthetic agents, propofol, lorazepam, and midazolam (oral and intranasal) decrease seizures and thus have little role in ECT [5–7]. Similarly, EMLA cream should not be used for pretreatment of myalgias as it can contain lidocaine, an amide local anesthetic, which decreases seizure duration and inhibits the ability to achieve a therapeutic seizure. However, seizure duration is prolonged with etomidate [5–7]. Methohexital and remifentanil are short-acting agents that have been found to have no significant effect on seizure duration [5,6]. It should be noted that in our patient, the decision was made to switch from methohexital to etomidate during ECT treatment 4 because of unsatisfactory seizure duration. Methohexital is typically favored over etomidate as the first-line anesthetic agent for ECT because of its ability to blunt the hemodynamic response, whereas etomidate is associated with myoclonus and does not block the hypertension and tachycardia associated with ECT.
Dexmedetomidine has also been studied for use in ECT. Dexmedetomidine serves as an alpha-2 agonist. Because of its highly selective alpha-2 agonist effects, a recent study in 2017 found that dexmedetomidine at a rate of 0.2 μg/kg was beneficial in minimizing the sympathetic hyperdynamic response caused by ECT without altering seizure duration or delaying recovery [8]. Further, dexmedetomidine does not lead to respiratory depression, which is advantageous, particularly in patients for whom mask ventilation is difficult. It should be noted that it is possible that a more rapid infusion of dexmedetomidine can increase the risk of severe sinus bradycardia during anesthetic induction [8].
There are mixed reports on the effect of ketamine on seizure duration. N2O and ketamine, however, are known to have an antidepressant activity of their own through affecting the N-methyl-D-aspartate (NMDA) receptor [6,9–11]. Because of the role of ketamine in acute reduction of depression severity, its role in ECT was recently studied as part of the KANCET randomized controlled trial. The KANCET trial found that there were no significant differences in any outcome measure during, at the end of, or 1 month following the ECT course, and that ketamine as an anesthetic does not enhance the efficacy of ECT [12].
Our literature search found that the use of N2O during ECT has been documented as an adjunct maintenance agent with other agents that decrease seizure duration. However, we did not find any reports or studies on use of N2O for ECT in the perioperative period with induction agents that are known to have no shortening effect on seizure duration. Considering the pleasant odor, independent antidepressant activity, calming psychological effect, low blood-gas partition coefficient, and minimal impact on respiration, N2O needs to be investigated to confirm its acceptability and safety for use during ECT.
N2O is a non-competitive N-methyl-D-aspartate (NMDA) receptor antagonist that confers an analgesic and anti-depressive effect to the gas. Sympathetic stimulation and release of endogenous opioids have also been reported to contribute to its antidepressant effects [13–15]. N2O has a low blood-gas solubility coefficient of 0.42, with limited metabolism in the body, allowing its use in patients with renal and liver dysfunction without prolonging recovery times. Ketamine acts as an NMDA antagonist but is less favored due to its unpleasant hallucinogenic effects and sympathomimetic effect. A proof-of-concept study revealed a significant antidepressant effect but excluded patients undergoing ECT and patients with psychotic symptoms [15]. The inhibition of methionine synthetase by N2O, a well-known side effect that results in elevated plasma homocysteine concentration and a decrease in B12 and folate levels, has not found to be clinically significant with repeated but short durations of exposure and can be managed by a folate-rich diet [16].
Finally, while volatile anesthetic agents such as sevoflurane have been shown to be adequate maintenance anesthetics for ECT, there have been no studies in the past decade to establish its widespread use in ECT. In comparison to nitrous oxide, sevoflurane would be less advantageous for several reasons. First, the time to induction and emergence of anesthesia would be longer due to its blood-gas partition coefficient of 0.65, which would argue against its use in a relatively short procedure like ECT [15]. Second, hypotension and arrhythmias are more pronounced with sevoflurane when compared to nitrous oxide [17].
Conclusions
Considering the above factors, we propose that N2O may be useful as an anesthetic agent in patients with anxiety, symptoms of severe psychological disorders, history of difficult intravenous access, or needle phobia. Studies to evaluate the effect of N2O on seizure duration, depression scores in conjunction with ECT, and perioperative adverse events are essential before expanding the use of N2O.
References:
1.. Singh A, Kar SK, How electroconvulsive therapy works? Understanding the neurobiological mechanisms: Clin Psychopharmacol Neurosci, 2017; 15(3); 210-21
2.. Andrade C, Arumugham SS, Thirthalli J, Adverse effects of electroconvulsive therapy: Psychiatr Clin North Am, 2016; 39(3); 513-30
3.. Gazdag G, Ungvari GS, Electroconvulsive therapy: 80 years old and still going strong: World J Psychiatry, 2019; 9(1); 1-6
4.. Luccarelli J, Henry ME, McCoy TH, Quantification of fracture rate during electroconvulsive therapy (ECT) using state-mandated reporting data: Brain Stimul, 2020; 13(3); 523-24
5.. Singh PM, Arora S, Borle A, Evaluation of etomidate for seizure duration in electroconvulsive therapy: A systematic review and meta-analysis: J ECT, 2015; 31(4); 213-25
6.. Soehle M, Bochem J, Anesthesia for electroconvulsive therapy: Curr Opin Anaesthesiol, 2018; 31(5); 501-5
7.. Pekel M, Postaci NA, Aytaç İ, Sevoflurane versus propofol for electro-convulsive therapy: Effects on seizure parameters, anesthesia recovery, and the bispectral index: Turk J Med Sci, 2016; 46(3); 756-63
8.. Li X, Tan F, Jian CJ, Effects of small-dose dexmedetomidine on hyper-dynamic responses to electroconvulsive therapy: J Chin Med Assoc, 2017; 80(8); 476-81
9.. Zolezzi M, Medication management during electroconvulsant therapy: Neuropsychiatr Dis Treat, 2016; 12; 931-39
10.. Ray-Griffith SL, Eads LA, Han X, A randomized pilot study comparing ketamine and methohexital anesthesia for electroconvulsive therapy in patients with depression: J ECT, 2017; 33(4); 268-71
11.. Erdil F, Ozgul U, Çolak C, Effect of the addition of ketamine to sevoflurane anesthesia on seizure duration in electroconvulsive therapy: J ECT, 2015; 31(3); 182-85
12.. Fernie G, Currie J, Perrin JS, Ketamine as the anaesthetic for electro-convulsive therapy: The KANECT randomised controlled trial [published correction appears in Br J Psychiatry, 2018; 212(5): 323]: Br J Psychiatry, 2017; 210(6); 422-28
13.. Tadler SC, Mickey BJ, Emerging evidence for antidepressant actions of anesthetic agents: Curr Opin Anaesthesiol, 2018; 31(4); 439-45
14.. Zorumski CF, Nagele P, Mennerick S, Conway CR, Treatment-resistant major depression: Rationale for NMDA receptors as targets and nitrous oxide as therapy: Front Psychiatry, 2015; 6; 172
15.. Nagele P, Duma A, Kopec M, Nitrous oxide for treatment-resistant major depression: A proof-of-concept trial: Biol Psychiatry, 2015; 78(1); 10-18
16.. Edigin E, Ajiboye O, Nathani A, Nitrous Oxide-induced B12 deficiency presenting with myeloneuropathy: Cureus, 2019; 11(8); e5331
17.. Kim D, Oh J, Choi W, The economic evaluation of nitrous oxide in sevoflurane anesthesia: Anesthesia and Pain Medicine, 2017; 12(1); 23-27
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133