19 August 2020: Articles 
A 28-Year-Old Man from India with SARS-Cov-2 and Pulmonary Tuberculosis Co-Infection with Central Nervous System Involvement
Challenging differential diagnosis, Rare coexistence of disease or pathology
Fateen Ata1EF, Qudsum Yousaf2DF, Jessiya Veliyankodan Parambil1F, Jabeed Parengal3B, Mohamed G. Mohamedali1F, Zohaib Yousaf1ABDEF*DOI: 10.12659/AJCR.926034
Am J Case Rep 2020; 21:e926034






Abstract
BACKGROUND: Tuberculosis (TB) is a great mimic of central nervous system (CNS) tumors. This mimicry may pose a challenge, as the management of both diseases is quite different. Furthermore, the temporal association of initiating treatment affects prognosis. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) mainly infects the pulmonary system. However, in a patient with concomitant pulmonary tuberculosis, it can be a diagnostic challenge.
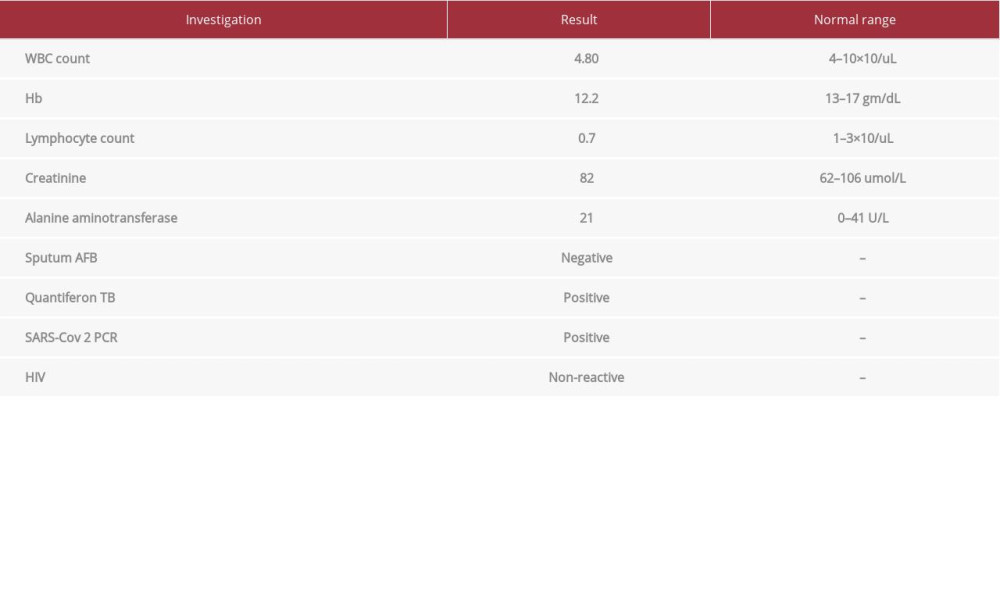
CASE REPORT: A 28-year-old man of Indian origin presented with headache and vomiting. He had a brain mass on imaging suggestive of a glioma. He also had lung infiltrates and was diagnosed with a co-infection by SARS-CoV-2, by a reverse-transcription polymerase chain reaction (RT-PCR) using the GeneXpert system. The mass was excised and was found to be a tuberculoma, diagnosed by Xpert MTB. He received first-line anti-TB and treatment for COVID-19 pneumonia based on local guidelines.
CONCLUSIONS: This report highlights that COVID-19 can co-exist with other infectious diseases, such as TB. A high degree of clinical suspicion is required to detect TB with atypical presentation. A co-infection of pulmonary and CNS TB with COVID-19 can present a diagnostic challenge, and appropriate patient management relies on an accurate and rapid diagnosis. Surgery may be necessary if there are compressive signs and symptoms secondary to CNS TB. A diagnosis of COVID-19 should not delay urgent surgeries. Further studies are needed to understand the effects of COVID-19 on the clinical course of TB.
Keywords: COVID-19, Glioma, Mycobacterium Infections, Tuberculosis, Central Nervous System, Betacoronavirus, COVID-19, Cerebellar Diseases, Cerebellum, coinfection, Comorbidity, Coronavirus Infections, Magnetic Resonance Imaging, Pandemics, Pneumonia, Viral, Radiography, Thoracic, SARS-CoV-2, Tuberculosis, Pulmonary
Background
TB is an extensively studied disease [1]. Occasionally, a diagnostically challenging case presents atypically. The prevalence of TB is higher in patients infected with human immunodeficiency virus (HIV) [2]. The co-infection of active pulmonary TB with COVID-19 has recently been described [3]. As of 10 July 2020, COVID-19 has infected more than 12 million people globally [4]. Indirectly, it has affected society’s entire fabric, with psychological, social, and economic repercussions [5]. There are concerns about a possible increase in TB-related mortality and morbidity if the disease diagnosis is delayed or missed. Changes in clinical practice due to the COVID-19 pandemic may negatively affect clinical outcomes in such patients [6]. Any critical procedures, including neurosurgery, must not be delayed due to SARS-CoV-2 co-infection.
Case Report
FOLLOW-UP:
The patient was discharged from the TB facility 28 days after his initial presentation. On follow-up in the TB clinic after 2 weeks, he was asymptomatic. Ethambutol was stopped, and he was continued on Rifampicin, Isoniazid, and Pyridoxine, with a twice-a-monthly follow-up plan.
Discussion
Tuberculosis is one of the most extensively studied infectious diseases due to the mortality and morbidity burden since the stone age [7]. The most common organ system involved is the respiratory system, documented as far back as 1932 [8]. TB affects the CNS in 3 common patterns: meningitis, tuber-culomas, or spinal arachnoiditis [9]. Patients with CNS involvement usually present with a headache and fever, which can progress to coma if left untreated or if diagnosis is delayed [10–12]. Atypical presentations of TB are relatively rare, but have been reported. CNS TB can mimic a malignant CNS tumor clinically and on radiography, which can pose a diagnostic challenge [13,14].
The diagnosis of CNS TB starts with a strong clinical suspicion followed by a cerebrospinal fluid (CSF) analysis, QuantiFERON TB test, or purified protein derivative test. The classical CSF picture shows a raised protein level and reduced glucose level, with a lymphocytic predominance. However, one-third of the cases have neutrophil predominance [15]. Additional tests from the CSF that can help include AFB smear, PCR, and culture. Although a spot AFB smear has a low yield, repeated samples can increase its yield to around 87% [12]. Adenosine deaminase from the CSF has a sensitivity and specificity of 79% and 91%, respectively [16]. Nucleic acid amplification can aid in rapid diagnosis, as results can be available within hours [17].
Pulmonary TB should be considered if there are radiographic changes in the thoracic cavity in the presence of Tb involvement of any other system [18].
A treacherous situation arises when a patient has 2 menacing infections that are unrelated to each other. Our case report describes such a scenario of COVID-19 and TB co-infection. This is a diagnostic challenge because the presentation and radiological manifestations can be comparable. Fever is one of the most frequent clinical signs of TB. It is also the most common sign in COVID-19, irrespective of comorbidities [19]. Chest X-ray findings can be present in both. COVID-19 has a bilateral, diffuse, infiltrative pattern, and the most common X-ray finding seen in TB is unilateral upper-zone opacity [20].
In a high-resolution CT thorax, ground-glass opacities are seen mainly in COVID-19 infection, whereas disseminated TB usually manifests as multiple nodular opacities. However, 20% of TB patients have ground-glass opacities [21,22].
In a previous study describing TB and COVID-19 co-infection, ground-glass opacities were attributed to COVID-19 rather than TB, due to the higher prevalence of these findings in SARS-CoV-2 infection. However, as it can be due to both, it is difficult to confidently identify the cause [3].
A single ring-enhancing brain mass, with rapidly worsening clinical symptoms, can be seen in CNS tumors and TB. In addition to radiological similarities, the clinical presentation can be similar.
Upon initiation of ATT, an enhanced delayed-type hypersensitivity reaction leads to lymphocyte and macrophage chemotaxis to the site of TB infection. This chemotaxis in CNS TB can lead to a glioma-like aggravated lesion, causing a paradoxical worsening of symptoms despite being on appropriate anti-TB treatment [23].
A biopsy to diagnose TB is rarely the first step. With an initial suspicion of TB, the MRI described a glioma with a mass effect. In such a dilemma, a delay in surgical intervention could increase mortality and morbidity. Restrictions have been in place globally to mitigate the spread of SARS-CoV-2. These restrictions have negatively affected care for diseases other than COVID-19, including non-urgent surgeries. Prompt clinical diagnosis and careful clinical judgment are essential to assure performance of essential surgical interventions [6].
Conclusions
This report highlights that COVID-19 can co-exist with other infectious diseases, such as TB. A high degree of clinical suspicion is required to detect TB with atypical presentation. A co-infection of pulmonary and CNS TB with COVID-19 can present a diagnostic challenge, and appropriate patient management relies on an accurate and rapid diagnosis. Surgery may be necessary in the case of compressive signs and symptoms secondary to CNS TB. A diagnosis of COVID-19 should not delay urgent surgeries. Further studies are needed to understand the effects of COVID-19 on the clinical course of TB.
Figures
References:
1.. Murray JF, Schraufnagel DE, Hopewell PC, Treatment of tuberculosis. A historical perspective: Ann Am Thorac Soc, 2015; 12(12); 1749-59
2.. Getahun H, Gunneberg C, Granich R, Nunn P, HIV infection-associated tuberculosis: the epidemiology and the response: Clin Infect Dis, 2010; 50(Suppl. 3); S201-7
3.. Tadolini M, Codecasa LR, García-García JM, Active tuberculosis, sequel-ae and COVID-19 co-infection: first cohort of 49 cases: Eur Respir J, 2020; 56(1); 2001398
4.. , Coronavirus disease (COVID-19) Situation Report – 172 2020 11 July, 00 CEST, 10 July 2020] Available from: .https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200710-covid-19-sitrep-172.pdf?sfvrsn=70724b90_2
5.. Dubey S, Biswas P, Ghosh R, Psychosocial impact of COVID-19: Diabetes Metab Syndr, 2020; 14(5); 779-88
6.. Ramakrishna R, Zadeh G, Sheehan JP, Inpatient and outpatient case prioritization for patients with neuro-oncologic disease amid the COVID-19 pandemic: General guidance for neuro-oncology practitioners from the AANS/CNS Tumor Section and Society for Neuro-Oncology: J Neurooncol, 2020; 147(3); 525-29
7.. Pezzella AT, History of pulmonary tuberculosis: Thorac Surg Clin, 2019; 29(1); 1-17
8.. Poulsen A, Some clinical features of tuberculosis: Acta Tuberc Scand, 1957; 33(1–2); 37-92 ; concl
9.. al-Deeb SM, Yaqub BA, Motarey KR, Neurotuberculosis: A review: Clin Neurol Neurosurg, 1992; 94(Suppl.); S30-33
10.. Farinha NJ, Razali KA, Holzel H, Tuberculosis of the central nervous system in children: A 20-year survey: J Infect, 2000; 41(1); 61-68
11.. Hinman AR, Tuberculous meningitis at Cleveland Metropolitan General Hospital 1959 to 1963: Am Rev Respir Dis, 1967; 95(4); 670-73
12.. Kennedy DH, Fallon RJ, Tuberculous meningitis: JAMA, 1979; 241(3); 264-68
13.. Chaudhry UR Farooq, Rauf F, Bhatti SK, Tuberculosis simulating brain tumour: Neuroradiol J, 2011; 24(3); 350-56
14.. Suslu HT, Bozbuga M, Bayindir C, Cerebral tuberculoma mimicking high grade glial tumor: Turk Neurosurg, 2011; 21(3); 427-29
15.. Karandanis D, Shulman JA, Recent survey of infectious meningitis in adults: Review of laboratory findings in bacterial, tuberculous, and aseptic meningitis: South Med J, 1976; 69(4); 449-57
16.. Xu HB, Jiang R-H, Li L, Diagnostic value of adenosine deaminase in cerebrospinal fluid for tuberculous meningitis: A meta-analysis: Int J Tuberc Lung Dis, 2010; 14(11); 1382-87
17.. Marks SM, Cronin W, Venkatappa T, The health-system benefits and cost-effectiveness of using Mycobacterium tuberculosis direct nucleic acid amplification testing to diagnose tuberculosis disease in the United States: Clin Infect Dis, 2013; 57(4); 532-42
18.. Pai M, Nicol MP, Boehme CC, Tuberculosis diagnostics: State of the art and future directions: Microbiol Spectr, 2016; 4(5)
19.. Guan WJ, Liang W-H, Zhao Y, Comorbidity and its impact on 1590 patients with COVID-19 in China: A nationwide analysis: Eur Respir J, 2020; 55(5); 2000547
20.. Barnes PF, Verdegem TD, Vachon LA, Chest roentgenogram in pulmonary tuberculosis. New data on an old test: Chest, 1988; 94(2); 316-20
21.. Hu Z, Song C, Xu C, Clinical characteristics of 24 asymptomatic infections with COVID-19 screened among close contacts in Nanjing, China: Sci China Life Sci, 2020; 63(5); 706-11
22.. Lee J, Lim JK, Seo H, Clinical relevance of ground glass opacity in 105 patients with miliary tuberculosis: Respir Med, 2014; 108(6); 924-30
23.. Kim JK, Jung T-Y, Lee K-H, Kim S-K, Radiological follow-up of a cerebral tuberculoma with a paradoxical response mimicking a brain tumor: J Korean Neurosurg Soc, 2015; 57(4); 307-10
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133