16 August 2020: Articles 
Renal Transplant Recipient with Concurrent COVID-19 and Pneumonia Treated with Trimethoprim/Sulfamethoxazole Leading to Acute Kidney Injury: A Therapeutic Dilemma
Diagnostic / therapeutic accidents, Unusual setting of medical care, Adverse events of drug therapy, Educational Purpose (only if useful for a systematic review or synthesis), Rare coexistence of disease or pathology
Mohamed A. Mohamed1BEF, Jasleen Kaur2CDEF, Farah Wani1BF, Asim Kichloo1ADE, Ravinder Bhanot3ACDEF*DOI: 10.12659/AJCR.926464
Am J Case Rep 2020; 21:e926464






Abstract
BACKGROUND: Although coronavirus disease 2019 (COVID-19) manifests primarily as a lung infection, its involvement in acute kidney injury (AKI) is gaining recognition and is associated with increased morbidity and mortality. Concurrent infection, which may require administration of a potentially nephrotoxic agent, can worsen AKI and lead to poor outcomes. Stenotrophomonas maltophilia is a multidrug-resistant gram-negative bacillus associated with nosocomial infections, especially in severely immunocompromised and debilitated patients. Trimethoprim/sulfamethoxazole combination (TMP/SMX) is considered the treatment of choice but can itself lead to AKI, posing a significant challenge in the management of patients with concomitant COVID-19 and S. maltophilia pneumonia.
CASE REPORT: A 64-year-old male with end-stage renal disease and post renal transplant presented with severe respiratory symptoms of COVID-19 and was intubated upon admission. His renal functions were normal at the time of admission. The patient subsequently developed superimposed bacterial pneumonia with S. maltophilia requiring administration of TMP/SMX. However, TMP/SMX led to the development of AKI, which continued to worsen despite appropriate management including hemodialysis. This coincided with and most likely resulted in the patient’s clinical deterioration and ultimate death.
CONCLUSIONS: The etiology of kidney disease involvement in patients with COVID-19 is still evolving and appears to be multifactorial. The condition can significantly worsen especially when nephrotoxic agents are given, probably due to a cumulative or synergistic effect. Great caution should be taken when administering nephrotoxic agents in the setting of COVID-19 as it can lead to adverse patient outcomes.
Keywords: Acute Kidney Injury, COVID-19, Stenotrophomonas maltophilia, Trimethoprim-Sulfamethoxazole Combination, Kidney Transplantation, Anti-Bacterial Agents, Betacoronavirus, COVID-19, Clinical Deterioration, coinfection, Coronavirus Infections, Fatal Outcome, Gram-Negative Bacterial Infections, Immunocompromised Host, Pandemics, Pneumonia, Bacterial, Pneumonia, Viral, SARS-CoV-2, transplant recipients
Background
Since the global outbreak of the coronavirus disease 2019 (COVID-19), which is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), it has been established that the disease manifests mainly as a lower respiratory tract infection [1,2]. Although its involvement in other systems has been noted, the extended effects have not yet been fully studied. However, the renal system is commonly affected and acute kidney injury (AKI) has been reported in 3% to 37% of COVID-19 patients, often with increased morbidity and mortality [3–5]. This poses a significant challenge in the treatment of such patients who may require nephrotoxic drug administration to treat a concurrent infection or underlying pathology.
Case Report
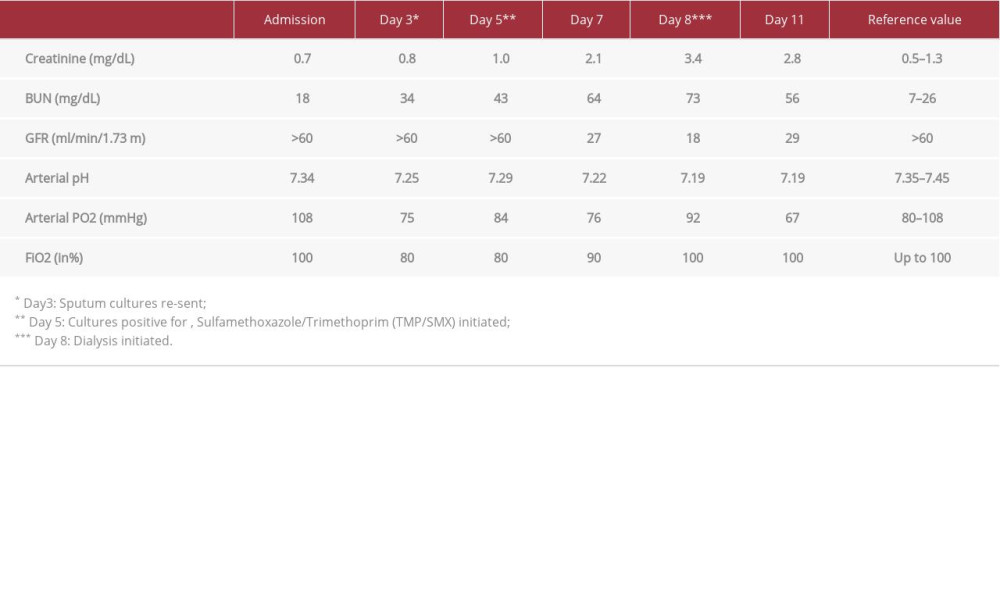
A 64-year-old Caucasian man with a medical history including type 2 diabetes and hypertension presented to the emergency department with symptoms of progressive shortness of breath, recurrent fever, and cough for 4 days. He was also a kidney transplant recipient (deceased donor) maintained on immunosuppressive drugs including 5 mg tacrolimus twice per day, 250 mg mycophenolic acid twice per day, and 5 mg prednisone once per day. His renal parameters were normal upon admission with serum creatinine of 0.7 mg/dL and a glomerular filtration rate (GFR) >60 ml/min/1.73 m2. Relevant workup included a chest radiography (CXR) which revealed diffuse inter-stitial and airspace opacities in the bilateral lungs, suggestive of multifocal pneumonia (Figure 1). The gram stain on the sputum sample was negative for any organism, and a rapid influenza test and pneumococcal and legionella urinary antigen test were negative. His nasopharyngeal swab results returned positive for SARS-CoV-2 infection by a real-time reverse transcriptase polymerase chain reaction test (RT-PCR), done using the Abbott ID Now SARS-CoV-2 RT-PCR testing system. He was admitted to the intensive care unit and was electively intubated because of his worsening respiratory status and severe acute hypoxic respiratory failure. The patient was started on compassionate use of hydroxychloroquine with azithromycin for COVID-19 infection, which was standard care during the time of his hospitalization and our institution’s policy. While awaiting the final sputum culture report, he was also started on cefepime for broad antibiotic coverage because of the severity of his disease. His immunosuppressive medications were adjusted and included the suspension of mycophenolic acid, reduction of tacrolimus to 2.5 mg twice per day, and the continuation of prednisone at his home dose of 5 mg per day. For mechanical ventilation, a low tidal volume lung-protective strategy was employed along with prone positioning and neuromuscular blockade (atracurium) under sedation. High positive end-expiratory pressure therapy was also instituted to maintain adequate oxygenation.
On day 3, the patient’s sputum sample was redrawn because of increased endotracheal secretions, worsening results of the CXR, and hypoxemia (Figure 2). The patient was switched to a high dose of corticosteroids (60 mg IV methylprednisolone once daily). The sputum examination came back positive for gram-negative bacilli on hospitalization day 4, and on day 5 the automated culture with antibiogram identified the bacterium
Discussion
There is increasing evidence that AKI and kidney abnormalities are associated with COVID-19 and lead to a higher risk of morbidity and mortality [3–5]. Although the exact mechanism remains unclear, it is postulated that SARS-CoV-2 can penetrate the cells of the kidney tubule and cause direct cytotoxic effects through rapid replication within each cell [3]. Renal histopathological analysis of patients with COVID-19 has revealed distinct features of injury involving the direct injury to the parenchyma, likely due to endothelial damage from severe acute tubular necrosis with lymphocyte and macrophage infiltration [9,10]. The main binding site for cell entry of SARSCoV-2 is the angiotensin-converting enzyme 2 protein, which is found on a much larger scale in the proximal and distal tubules of the kidney than in those found in the lung alveoli [11]. Morphological findings of RBC fragments and fibrin thrombi in renal vasculature have also been seen leading to small vessel occlusion, suggesting another theory of AKI in patients with COVID-19 [9,10]. Kidney disease in patients with COVID-19 can manifest as proteinuria, hematuria, or AKI, and each of these presentations can be an independent risk factor for in-patient hospital death as shown in a recent prospective analysis of 701 COVID-19 patients [3]. Another large observational study from New York showed that AKI occurs frequently among patients with COVID-19 and in temporal association with respiratory failure and is associated with a 35% mortality rate [12]. In addition to having been severely affected by COVID-19, our patient had underlying risk factors to develop AKI, namely, his single-functioning transplanted kidney, diabetes, hypertension, and immunosuppressed status.
We question how much of our patient’s AKI burden was attributable to TMP-SMX and how much was attributable to the COVID-19 infection. In a previous study, the adverse effects of TMP/SMX were assessed in 573 patients, of which 5.8% developed AKI solely due to the drug without confounding factors, and only 1 patient required dialysis [8]. These results agreed with other studies which showed that, although AKI is a common adverse effect of TMP/SMX, it is usually transient and often subsides after discontinuation of the medication [17]. On the other hand, a recent epidemiological study showed that renal replacement therapy was required in 5% (14) of 278 pooled patients with COVID-19, indicating a relatively high prevalence [18]. Considering the speed and severity of our patient’s renal decline, we believe that the nephrotoxic effects of COVID-19, even after discontinuation of the TMP/SMX, played an independent role in his poor outcome. More research is needed to analyze the additive or possible synergistic nephrotoxic effects of COVID-19 and common nephrotoxic agents administered during clinical practice. Currently data on AKI in association with COVID-19 infection is minimal and is based mostly on case reports and small-scale retrospective studies. Larger scale studies are needed to fully assess the role of COVID-19 on renal function.
Conclusions
The burden of COVID-19 needs to be considered as a contributing factor in patients with worsening AKI, even in the setting of shock, sepsis, and nephrotoxic agents. This burden is believed to be secondary to the direct tubular damage caused by virus replication inside cells or by microthrombi formation leading to microangiopathy [3,9]. Caution should be taken when administering nephrotoxic agents in cases of severe COVID-19 as it can lead to poor outcomes.
References:
1.. Huang C, Wang Y, Li X, Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China: Lancet, 2020; 395; 497-506
2.. Guan WJ, Ni ZY, Hu Y, Clinical characteristics of coronavirus disease 2019 in China: N Engl J Med, 2020; 382; 1708-20
3.. Cheng Y, Luo R, Wang K, Kidney disease is associated with in-hospital death of patients with COVID-19: Kidney Int, 2020; 97(5); 829-38
4.. Chen T, Wu D, Chen H, Clinical characteristics of 113 deceased patients with coronavirus disease 2019: retrospective study: BMJ, 2020; 368; m1091
5.. Ng JJ, Luo Y, Phua K, Choong AMTL, Acute kidney injury in hospitalized patients with coronavirus disease 2019 (COVID-19): A meta-analysis: J Infect, 2020 [Online ahead of print]
6.. Anthony AA, Thor AS, Anthony IO: Front Microbiol, 2017; 8; 2276
7.. Chang YT, Lin CY, Chen YH, Hsueh PR: Front Microbiol, 2015; 6; 893
8.. Traci NF, Andres AA, Edward AG, Daniel MM, Acute kidney injury associated with trimethoprim/sulfamethoxazole: J Antimicrob Chemother, 2012; 67(5); 1271-77
9.. Su H, Yang M, Wan C, Renal histopathological analysis of 26 postmortem findings of patients with COVID-19 in China: Kidney Int, 2020; 98(1); 219-27
10.. Diao B, Feng Z, Wang C, Human kidney is a target for novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection: MedRxiv, 2020 2020.03.04.20031120
11.. Serfozo P, Wysocki J, Gulua G, Ang II (angiotensin II) conversion to angiotensin-(1–7) in the circulation is POP (prolyloligopeptidase)-dependent and ACE2 (angiotensin-converting enzyme 2)-independent: Hypertension, 2020; 75(1); 173-82
12.. Hirsch JS, Ng JH, Ross DW, Acute kidney injury in patients hospitalized with COVID-19: Kidney Int, 2020; 98; 209-18
13.. Brooke JS: Clin Microbiol Rev, 2012; 25(1); 2-41
14.. Saied WI, Merceron S, Schwebel C: J Infect, 2020; 80(3); 279-85
15.. Nseir S, Di Pompeo C, Brisson H: Critical Care, 2006; 10(5); R143
16.. Fraser TN, Avellaneda AA, Graviss EA, Musher DM, Acute kidney injury associated with trimethoprim/sulfamethoxazole: J Antimicrobl Chemother, 2012; 67(5); 1271-77
17.. Ho JMW, Juurlink DN, Considerations when prescribing trimethoprim–sulfamethoxazole: Can Med Assoc J, 2011; 183(6); 1851-58
18.. Lai CC, Shih TP, Ko WC, Severe acute respiratory syndrome corona-virus 2 (SARS-CoV-2) and corona virus disease-2019 (COVID-19): The epidemic and the challenges: Int J Antimicrob Agents, 2020; 55(3); 105924
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133