14 August 2020: Articles 
Tracheal Stenosis After Tracheostomy for Mechanical Ventilation in COVID-19 Pneumonia– A Report of 2 Cases from Northern Italy
Unusual clinical course, Challenging differential diagnosis, Diagnostic / therapeutic accidents, Management of emergency care
Carmine Fernando Gervasio1E, Gianluca Averono1C, Luca Robiolio1B, Massimo Bertoletti2B, Umberto Colageo3D, Luca De Col3D, Fabio Bertone1E*DOI: 10.12659/AJCR.926731
Am J Case Rep 2020; 21:e926731






Abstract
BACKGROUND: The role of tracheostomy during the coronavirus disease 2019 (COVID-19) pandemic is still to be determined, and the complication rate of the tracheostomy in COVID-19 patients is still unknown. Postintubation tracheal stenosis is a well-known risk of prolonged endotracheal intubation, but it is too early to define the existence of any difference among the COVID-19 cohort of patients and non-COVID-19 patients. This report is of 2 cases of COVID-19 pneumonia that required tracheostomy and prolonged endotracheal intubation, which were followed by delayed tracheal stenosis.
CASE REPORT: Case 1. A 54-year-old male was admitted to our hospital (Biella, Italy) for severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection. The patient underwent orotracheal intubation, progressively improving his breathing function, and was discharged after 20 days. Ten days later, the patient presented with severe respiratory distress. Computed tomography (CT) scan and bronchoscopy showed signs of tracheal stenosis. We administered intravenous steroids for 10 days. The patient showed increasing improvement in his breathing function and was discharged with no other signs of respiratory distress. Case 2. A 43-year-old male was admitted to our hospital for SARS-CoV-2 infection. The patient underwent orotracheal intubation, progressively improving his breathing function, and was discharged after 25 days. Eighteen days later, the patient came to our emergency room with severe respiratory distress. CT scan and bronchoscopy showed signs of tracheal stenosis. The patient had to undergo tracheal resection.
CONCLUSIONS: The 2 cases presented in this report have shown that even when patients recover from severe COVID-19 pneumonia requiring tracheostomy and mechanical ventilation, tracheal stenosis should be recognized as a potential complication and careful follow-up is required.
Keywords: COVID-19, tracheal stenosis, Tracheotomy, Betacoronavirus, COVID-19, Coronavirus Infections, Glucocorticoids, Intubation, Intratracheal, Methylprednisolone, Pandemics, Pneumonia, Viral, Respiration, Artificial, SARS-CoV-2, Tracheostomy
Background
The role of tracheostomy during the pandemic of coronavirus disease 2019 (COVID-19) is still to be determined. The decision about performing tracheostomy in patients affected by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) presents unique challenges. Mortality rate for those requiring critical care and invasive mechanical ventilation is higher (approximately 50%) than in non-COVID-19 patients [1,2], and the prognosis and sequelae of this new disease have not been fully understood yet. In Wuhan (China), of 201 patients requiring intubation, 134 patients died (67%) [3]. The same mortality rate has been reported in Washington State [4,5]. Tracheostomy normally eases weaning from invasive mechanical ventilation to natural breathing, and also prevents long-term complications, including tracheal stenosis. In patients affected by SARS-CoV-2, a different trend has been observed: during invasive mechanical ventilation there has been either a rapid progression toward death or a quick resolution; in both cases benefits from tracheostomy would be null [5]. Such reasons increase the risk of performing futile procedures if tracheostomy is carried out too early [6]. In addition, the risk of viral dissemination caused by tracheostomy in the operating room and in postoperative care is notable [5]. Therefore, current literature and opinion suggest that tracheostomy should be considered only after invasive mechanical ventilation. Additional criteria for tracheostomy are the favorable prognosis of the patient and the fact that it does not impede breathing [1–3]. The decision on the timing of tracheostomy is even more complex because the complication rate of tracheostomy in positive COVID-19 patients is still undetermined, especially in late-performed ones.
Postintubation tracheal stenosis is a well-known risk of prolonged endotracheal intubation, but in systematic reviews there is no statistically significant evidence that it is reduced in patients treated with early tracheostomy.
The current literature estimates the incidence of posttracheostomy stenosis from 1.5% to 2.6% [7–9]. Tracheal stenosis in patients who underwent orotracheal intubation is estimated to be 1–2%. Therefore, the rates are comparable, with no substantial difference between the procedures [8,9].
Early conversion to tracheostomy within the first 7 days of intubation does not significantly decrease the risk of tracheal stenosis compared with later conversions. Anyway, it is too early to define the existence of any difference among the cohort of COVID-19 and non-COVID-19 patients [10–12].
Tracheostomy can be performed either as an open procedure or percutaneously, depending on the patient’s characteristics and on the surgeon’s preference. An important recent meta-analysis [13] showed that there was no statistically significant difference between the 2 techniques in terms of mortality rate, intraoperative hemorrhage, and postoperative hemorrhage. At the moment, there is no scientific evidence on which of the 2 procedures is preferable for COVID-19 patients [12].
In this paper we report cases of 2 patients presenting with COVID-19 pneumonia who required tracheostomy and prolonged invasive mechanical ventilation and developed delayed tracheal stenosis.
Case Reports
CASE 1:
A 54-year-old male was admitted to our hospital (Ospedale Degli Infermi, Biella, Italy) with symptoms corresponding to SARS-CoV-2 infection. He presented with hypertension, obesity (body mass index [BMI] 32), and disc herniation (L1–L2). A computed tomography (CT) scan was performed and showed bilateral diffuse opacities compatible with interstitial pneumonia. A nasopharyngeal swab confirmed the diagnosis of SARSCoV-2. The patient showed severe respiratory distress and subsequently underwent to orotracheal intubation. After 7 days in the intensive care unit (ICU), an open surgical tracheostomy was performed. The patient was then transferred to semi-intensive care. With progressively improved breathing function, the cannula was removed and the patient was discharged after 20 days, with oxygen saturation of 98%.
Ten days later, the patient was brought to our emergency room with severe respiratory distress. CT scan and bronchoscopy were performed and showed signs of tracheal stenosis (Figures 1, 2). We administered intravenous infusion of 80 mg/day of 6-methylprednisolone (6-MP) for 10 days. The patient showed increasing improvement in his breathing function and was discharged with no other signs of respiratory distress.
CASE 2:
A 43-year-old male was admitted to our hospital with symptoms corresponding to SARS-CoV-2 infection. He had diabetes mellitus type 2 and was obese (BMI 42). A CT scan was performed and showed bilateral diffuse opacities compatible with interstitial pneumonia. A nasopharyngeal swab confirmed the diagnosis of SARS-CoV-2. The patient showed severe respiratory distress and subsequently underwent orotracheal intubation. After 9 days in the ICU, an open surgical tracheostomy was performed. The patient was then transferred to semi-intensive care. After progressive improvement in his breathing function, the cannula was removed and the patient was discharged after 25 days, with an oxygen saturation of 96%.
Eighteen days later, the patient was brought to our emergency room with severe respiratory distress. CT scan and bronchoscopy were performed; signs of tracheal stenosis were visible (Figures 3, 4). We administered intravenous infusion of 80 mg/day of 6-MP for 10 days. The patient did not show any improvement in his breathing function and had to undergo tracheal resection.
Discussion
Between March and April 2020, 15 tracheotomies were performed at Ospedale Degli Infermi (Biella, Italy) for patients with COVID-19 pneumonia after invasive mechanical ventilation. All tracheostomies were performed through open procedures.
The diagnosis of SARS-CoV-2 infection was always confirmed by reverse transcription – real-time polymerase chain reaction from nasopharyngeal swabs.
A multidisciplinary intensive-care group made up of anesthesiologists and ear, nose, and throat (ENT) surgeons agreed on proceeding with tracheostomies in such patients. All procedures were carried out below the isthmus of the thyroid gland, incising the trachea, when possible, between the second and third tracheal rings, with several detached ties (from minimum of 5 to maximum 8 ties) with nonabsorbable stitches, following the guidelines of the Italian Society of Otolaryngology in every procedure. The first cannula change was delayed to 7–10 days. Of 15, 5 patients recovered clinically and serologically in the following weeks.
Upon discharge from the ICU, patients were transferred to a dedicated department for tracheostomized COVID-19 patients with specifically trained and experienced nursing staff. The decision to remove the cannula was made by the multi-disciplinary team after verifying that the patient was able to breathe without mechanical adjuvants, as well as clinical and serological healing that was determined through 2 negative nasopharyngeal swabs. All 5 patients then underwent bronchoscopy with evidence of normal laryngeal and tracheal findings before the cannula removal.
At the moment of discharge, all 5 patients were in good health, with 96–98% saturation, without any oxygen administration, and no respiratory distress.
Approximately 2 weeks after discharge, 2 of 5 patients developed progressive respiratory fatigue. They were brought to the emergency room, where they underwent neck and chest CT and bronchoscopy. Both patients showed marked tracheal stenosis, with reduction of respiratory volumes. At bronchos-copy, markedly fibrotic inflamed granulation tissue was found in the trachea. The patients were readmitted to specialized departments and assessed by a multidisciplinary group of pneumologists, anesthesiologists, and ENT surgeons. The decision was made to treat patients with significant doses of steroids as primary therapy.
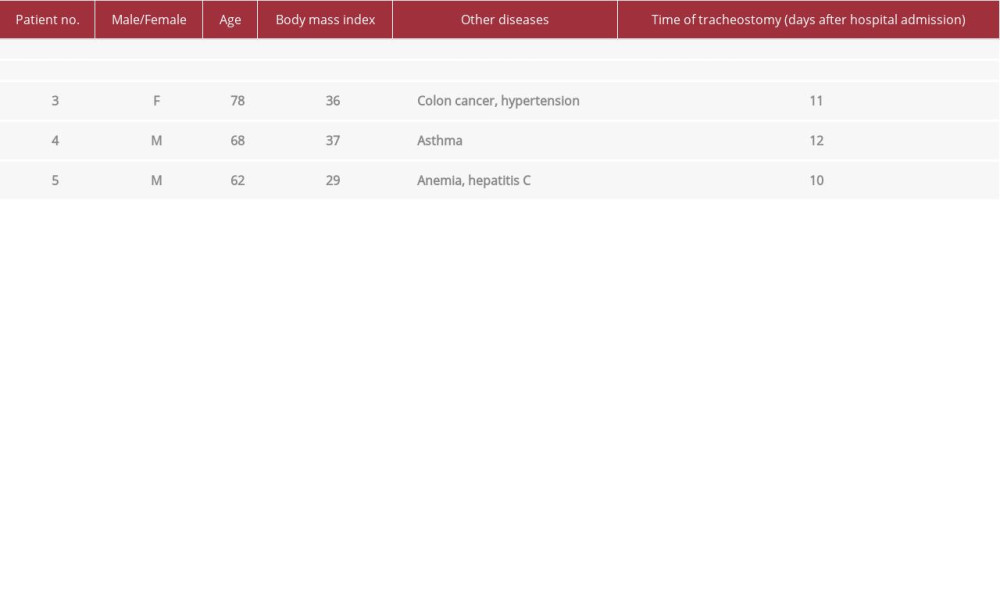
One patient experienced rapid improvement in respiratory function and the second bronchoscopy, performed after a week, showed a good reduction of the inflammatory tissue stenosing the trachea. The second patient, however, showed no significant improvement and it was necessary to proceed with tracheal resection. These 2 patients had no particularly different risk factors compared with the other 3 patients who did not develop any tracheal complications (Table 1).
There are still no data in the literature about the possible appearance of tracheal stenosis in COVID-19 patients after prolonged intubation and tracheostomy. In this manuscript we reported 2 cases of tracheal stenosis in such patients. This posttreatment complication appeared 10 and 18 days after discharge. It is well known that the most common cause of tracheal stenosis is iatrogenic, particularly common when large endotracheal tubes are used and in instances of a prolonged endotracheal tube placement [14–16]. However, it is not clear if the risk increases in COVID-19 patients. Laryngotracheal stenosis may also develop as a consequence of several auto-immune and rheumatological diseases. Its most known association is represented by granulomatosis and polyangiitis. Laryngotracheal stenosis was noticed in 12 to 23% of patients with granulomatosis [17,18]. In addition, higher rates of tobacco consumption, cardiovascular disease, obesity, and diabetes may cause increased vulnerability to ischemic damage and dysregulated wound healing [15].
At Ospedale Degli Infermi we reported 2 cases of severe tracheal stenosis of 5 COVID-19 extubated patients (complication rate: 40%); we did not detect any case of stenosis in 58 non-COVID patients who underwent tracheostomy in our department in the 2 previous years. Many factors are known to influence the incidence of tracheal stenosis or are considered likely to do so. Some examples are the injury severity, duration of intubation (pretracheostomy), posttracheostomy duration, cuff management, and ICU management. However, it is reasonable to think that COVID-19 patients may have a higher risk of developing tracheal stenosis. This is because those patients often have comorbidities such as hypertension or diabetes, are subjected to long intubation periods, and, above all, they show a marked tendency to tissue inflammation, which causes altered healing and fibrosis.
The decision to administer steroids was made on the grounds of the well-known fact that in COVID-19 patients, an overreaction of the immune system results in a cytokine storm. These cytokines induce immune cells to release a vast number of free radicals, which are the leading cause of multiple organ failure. Immunosuppression is essential to treat cytokine storms, especially for patients under the most severe distress. Steroids, as they are immunosuppressives, were widely used in treatment of COVID-19 to decrease cytokine storm and reduce the severity of inflammatory damage [19]. In 1 patient we found a remarkable and decisive improvement with the administration of steroids, which avoided having to use invasive procedures.
Conclusions
In this paper we reported 2 cases of tracheal stenosis in COVID-19 patients undergoing prolonged intubation and subsequent tracheostomy. Obviously, more histopathological and statistical data are needed in the next months to draw more evident conclusions and compare the data with those of COVID-19-negative patients. This could allow us to determine if the risk of tracheal stenosis is higher in COVID patients. This risk may be due to severe virus-related inflammatory damage and by the proven higher prevalence of stenosis in patients with chronic and granulomatous inflammatory diseases, similar conditions as in COVID-19.
The 2 cases presented in this report have shown that even when patients recover from severe COVID-19 pneumonia requiring tracheostomy and mechanical ventilation, tracheal stenosis should be recognized as a potential complication and careful follow-up is required.
Figures
References:
1.. Wu Z, McGoogan JM, Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72314 cases from the Chinese Center for Disease Control and Prevention: J Am Med Assoc, 2020 [Online ahead of print]
2.. , ICNARC report on COVID-19 in critical care, 2020 https://www.icnarc.org/Our-Audit/Audits/Cmp/Reports
3.. Wu C, Chen X, Cai Y, Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China: J Am Med Assoc Intern Med, 2020; 180(7); 1-11
4.. Arentz M, Yim E, Klaff L, Characteristics and outcomes of 21 critically ill patients with COVID-19 in Washington State: J Am Med Assoc, 2020; 323(16); 1612-14
5.. Shiba T, Ghaz-izadeh S, Chhetri D, Tracheostomy considerations during the COVID-19 pandemic: OTO Open, 2020; 4(2); 1-5
6.. Takhar A, Walker A, Tricklebank S, Recommendation of a practical guideline for safe tracheostomy during the COVID-19 pandemic: Eur Arch Otorhinolaryngol, 2020; 277(8); 2173-84
7.. Goldenberg D, Ari E, Golz A, Tracheotomy complications: A retrospective study of 1130 cases: Otolaryngol Head Neck Surg, 2000; 123; 495-500
8.. Halum S, Ting J, Plowman E, A multi-institutional analysis of tracheotomy complications: Laryngoscope, 2012; 122; 38-45
9.. Li M, Yiu Y, Merrill T, Risk factors for posttracheostomy tracheal stenosis: Otolaryngol Head Neck Surg, 2018; 159(4); 698-704
10.. Silva BNG, Andriolo RB, Saconato H, Early versus late tracheostomy for critically ill patients: Cochrane Database Syst Rev, 2015; 1(1); CD007271
11.. Curry SD, Rowan PJ: Otolaryngol Head Neck Surg, 2020; 162(2); 160-67
12.. David AP, Russell MD, El-Sayed IH, Tracheostomy guidelines developed at a large academic medical center during the COVID-19 pandemic: Head Neck, 2020; 42(6); 1291-96
13.. Johnson-Obaseki S, Veljkovic A, Javidnia H, Complication rates of open surgical versus percutaneous tracheostomy in critically ill patients: Laryngoscope, 2016; 126(11); 2459-67
14.. Woliansky J, Paddle P, Phyland D, Laryngotracheal stenosis management: A 16-year experience: Ear Nose Throat J, 2019 [Online ahead of print]
15.. Gadkaree SK, Pandian V, Best S, Laryngotracheal stenosis: Risk factors for tracheostomy dependence and dilation interval: Otolaryngol Head Neck Surg, 2017; 156(2); 321-28
16.. Halum SL, Ting JY, Plowman EK, A multi-institutional analysis of tracheostomy complications: Laryngoscope, 2012; 122(1); 38-45
17.. Langford CA, Sneller MC, Hallahan CW, Clinical features and therapeutic management of subglottic stenosis in patients with Wegener’s granulomatosis: Arthritis Rheum, 1996; 39(10); 1754-60
18.. Reinhold-Keller E, Beuge N, Latza U, An interdisciplinary approach to the care of patients with Wegener’s granulomatosis: Long-term outcome in 155 patients: Arthritis Rheum, 2000; 43(5); 1021-32
19.. Ye Y, Philip NP, Lagniton SY, COVID-19: What has been learned and to be learned about the novel coronavirus disease: Int J Biol Sci, 2020; 16(10); 1753-66
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133