14 January 2021: Articles 
Tissue Plasminogen Activator-Induced Angioedema Involving a Posterior Cerebral Artery Infarct: A Case Presentation
Unusual clinical course, Unusual or unexpected effect of treatment, Rare disease, Adverse events of drug therapy
Shahnaz Duymun1EF*, Vidhya Reddy1EF, Emma Bentley1EF, Anjali Bose-Kolanu1EDOI: 10.12659/AJCR.927137
Am J Case Rep 2021; 22:e927137






Abstract
BACKGROUND: Angioedema is characterized by localized swelling of subcutaneous or submucosal tissue resulting from fluid extravasation due to the loss of vascular integrity. It most commonly occurs with exposure to allergens and certain medications, namely nonsteroidal anti-inflammatory agents and angiotensin-converting enzyme inhibitors. There have been few incidences of angioedema following the administration of tissue plasminogen activator.
CASE REPORT: We describe an 84-year-old woman with a history of hypertension managed with lisinopril who presented with an acute onset of right-sided hemiparesis, slurred speech, and right-sided hemianopsia. Urgent computed tomography of the head revealed subacute infarct of the left pons without hemorrhage. Intravenous alteplase was administered and within 30 min our patient developed severe orolingual edema requiring emergent intubation. Subsequent imaging revealed acute to subacute infarct of the left occipital lobe in the posterior cerebral artery region, consistent with her initial presenting symptoms.
CONCLUSIONS: Angioedema induced by tissue plasminogen activator occurs in approximately 1–5% of patients receiving thrombolysis for ischemic stroke and can be life-threatening. The risk is increased in patients taking angiotensin-converting enzyme inhibitors, in patients with ischemic strokes of the middle cerebral artery, and in the presence of C1 esterase inhibitor deficiency. This phenomenon is usually self-limited and treatment is supportive, although evidence supports the use of antihistamines, steroids, epinephrine, and complement inhibitors. Due to the severity of angioedema and the potential progression to airway compromise, it is crucial to closely monitor patients receiving tissue plasminogen activator.
Keywords: angioedema, Drug-Related Side Effects and Adverse Reactions, Infarction, Posterior Cerebral Artery, Neurology, Thrombolytic Therapy, Tissue Plasminogen Activator, Aged, 80 and over, brain infarction, Fibrinolytic Agents, Posterior Cerebral Artery
Background
It is becoming increasingly common to use tissue plasminogen activator (tPA) in the treatment of acute ischemic stroke, pulmonary embolism, and ST-elevation myocardial infarctions. Since tPA was approved in 1996, its utilization has illustrated marked improvement in stroke recovery and decreased hospital stay [1]. Major concerns with the administration of tPA are intracranial hemorrhage, edema, and possible brain herniation; however, other severe reactions such as hemopericardium, cardiac tamponade, angioedema, and anaphylaxis should not be forgotten.
Angioedema induced by tPA is an infrequent, but potentially fatal outcome of thrombolysis. The mechanisms behind such reactions are presumed to involve mast cells, bradykinin release, histamine, and the complement cascade. It primarily occurs with infarction of the middle cerebral artery and is more likely to occur in patients with concomitant use of angiotensin-converting enzyme inhibitors and in carriers of C1 esterase inhibitor deficiency. It is mostly self-limited and treatment is usually supportive. Some cases may require antihistamines, steroids, and epinephrine, with refractory cases needing complement inhibitors and severe cases leading to intubation or cricothyroidotomy. In this report, we present a case of an elderly woman who developed angioedema following tPA administration for treatment of a posterior cerebral artery stroke, which has only been documented in 2 other cases, as per our literature review.
Case Report
An 84-year-old woman presented to the Emergency Department for right-sided weakness, slurred speech, and right-sided hemianopsia after having collapsed onto the floor. She had a history of hypertension, which managed with lisinopril; chronic obstructive pulmonary disease; and lung cancer with subsequent left upper lobectomy. Her history also included atrial fibrillation, but she had not been on anticoagulation therapy for approximately 3 months due to gastrointestinal bleed. The patient did not experience loss of consciousness, convulsions, or any prodromal symptoms. Upon arrival to the Emergency Department, she was found to have 2/5 strength of her right-sided extremities and right-sided neglect. An urgent computed tomography (CT) scan of the head was performed and revealed a subacute infarct of the left pons with no acute hemorrhage (Figure 1). A CT angiography was obtained and confirmed these findings. She was given 0.9 mg/kg alteplase intravenously, 10% as a bolus followed by an intravenous infusion of the remaining dose. Within 30 min from the onset of infusion, she developed orolingual angioedema consisting of tongue swelling and bilateral lip swelling requiring emergent intubation for airway protection.
The infusion was stopped prematurely, and the patient was given intravenous methylprednisolone 125 mg, diphenhydramine 50 mg, and famotidine 20 mg to help treat her angioedema. The neurology and critical care teams aided in the management of her care. There was marked improvement of her angioedema within 24 h, and she was subsequently extubated the following morning. Repeat CT of the head revealed an acute to subacute infarct with encephalomalacia of the left occipital lobe, which was believed to be the cause of her initial deficits (Figure 2). Echocardiography did not reveal an atrial shunt or evidence of thrombi. Subsequent magnetic resonance imaging illustrated infarct involving the posterior cerebral artery circulation without hemorrhagic conversion (Figure 3). She was started on full-dose aspirin as well as fluoxetine 20 mg daily for stroke recovery. She began to work with physical therapy and had some improvement in her motor skills as well as her vision.
During her hospitalization, she experienced persistent nausea and vomiting, ultimately controlled with promethazine. Her anticoagulation was restarted 10 days after the onset of her stroke. Her strength did not improve as she or her family had hoped. Family discussions were held, and it was decided the best course of action would be to receive hospice care at home. She was ultimately discharged to home with hospice on morphine sulfate, lorazepam, fluoxetine, and promethazine. She died a week later.
Discussion
Tissue plasminogen activator is commonly used to treat ischemic stroke, myocardial infarction, and pulmonary embolism. It is generally well tolerated and can be life-saving; however, there are concerning adverse reactions to be mindful of, one of which is angioedema. Angioedema induced by tPA is an uncommon but potentially fatal occurrence. It is typically observed within 1 h of completing the tPA infusion [2]. It is postulated to occur in approximately 1–5% of patients receiving thrombolysis after an ischemic stroke, and it usually presents with hemifacial edema contralateral to the infarct zone [3]. An extensive study done by Myslimi et al. [4] evaluated 923 patients who received thrombolysis for stroke treatment. Of these patients, only 20 developed angioedema. A retrospective chart review performed by Sczepanski and Bozyk [5] reviewed 147 cases, with only 4 developing edema.
The mechanism behind this phenomenon is still unclear; however, several hypotheses have been proposed to explain this occurrence. One hypothesis suggests a bradykinin-mediated pathway, in which tPA hydrolyzes plasminogen into plasmin, which in turn activates the kinin pathway augmenting the production of bradykinin [5]. Bradykinin is a potent pro-inflammatory and pro-edematous peptide that increases vascular permeability and vasodilation, leading to angioedema. In addition, tPA can augment histamine, causing vasodilation [3]. Other hypotheses propose that both tPA and plasmin activate the complement pathway, increasing complement levels and in turn activating mast cells, histamine, and basophil degranulation, which contribute to angioedema [5,6]. An additional hypothesis focuses on a mutation of the plasminogen gene, drawing on the remarkable clinical similarity between tPA-induced orolingual angioedema and a recently described new subtype of hereditary angioedema with normal C1 inhibitor. This subtype is caused by a highly specific missense mutation of the plasminogen gene and the resulting presence of the aberrant plasminogen protein is hypothesized to lead to angioedema [7].
The risk of developing angioedema following thrombolytic administration is amplified in patients who take angiotensin-converting enzyme (ACE) inhibitors because these drugs increase the concentration of circulating bradykinin [8]. Additionally, neurokinins such as substance P are increased with ACE inhibition and are mediators in inflammation and angioedema [9]. The combination of tPA-related increase in bradykinin, ACE inhibitor-mediated decrease in bradykinin metabolism, and ACE inhibitor-related increase in neurokinin levels amplify the risk of angioedema. For instance, in the study by Myslimi et al. [4], among the 20 patients who developed angioedema after thrombolysis, 45% concomitantly took ACE inhibitors.
Lesion-mapping studies have been performed that concluded infarctions of the middle cerebral artery, especially the branch that supplies the right insular cortex, have the highest propensity of causing angioedema. Ninety percent of patients who developed angioedema in the study completed by Myslimi et al. [4] and 75% of those in the study done by Sczepanski and Bozyk [5] had infarcts of the middle cerebral artery. The lesion-mapping study by Frohlich et al. [3] illustrated an association with right-sided insular infarcts and the development on tPA-related angioedema. The authors postulated that insular infarcts augment sympathetic hyperactivity due to impaired autonomic function, which in turn intensifies proinflammatory cytokine production and vascular permeability thus causing orolingual edema [3]. It is also believed that the tissue damage itself could be a trigger for angioedema via the generation of bradykinin, which increases inflammation and edema [4,8]. Our patient, however, had a posterior cerebral artery infarct, which is not consistent with this hypothesis, making our case unusual. In the retrospective institutional study done by Sczepanski and Bozyk [5], only 1 out of 147 patients had an infarct involving the posterior cerebral artery, and only 1 out of 42 patients in the analysis by Hurford et al. [10] had involvement of the posterior circulation. None were detected in the lesion-mapping study by Frohlich et al. [3] or in the meta-analysis by Yayan [1], and no alternate explanation could be found to support angioedema following tPA treatment of a posterior circulation stroke. The Table 1 summarizes findings from multiple studies including stroke location, development of angioedema after thrombolysis, and concomitant ACE inhibition [11–13].
Angioedema mediated by tPA is a rare and potentially life-threatening occurrence. At the first signs of tPA-induced angioedema, hospital staff should be aware of the commonly used interventions and medications. It is critical to discontinue the tPA infusion when signs of angioedema occur. The 2018 guidelines for the management of tPA-induced angioedema recommend the administration of intravenous methylprednisolone 125 mg, oral diphenhydramine 50 mg, and oral ranitidine 50 mg or famotidine 20 mg with a class IIb recommendation and level C expert opinion [14,15]. If symptoms persist despite these measures, epinephrine can be administered; however, it should be administered cautiously because it may suddenly increase blood pressure and thus the risk of intracranial hemorrhage [14]. Epinephrine would have been a reasonable alternative in this case due to the extent of angioedema that developed. Other alternatives include fresh frozen plasma, ecallantide (a recombinant protein that inhibits kallikrein), and C1 esterase inhibitors, all of which have been primarily used in ACE inhibitor-triggered angioedema or C1 esterase inhibitor deficiency but could have a role in tPA-related angioedema given the role of bradykinin [2,14]. Pahs et al. [16] demonstrated the use of plasma-derived C1 esterase inhibitor in a case of tPA-mediated angioedema. They described a case of potential airway compromise following tPA administration refractory to steroids and H2 blockers that ultimately resolved with a C1 esterase inhibitor and avoided the need for an invasive airway maneuver [16]. One last alternate therapy involves icatibant, a selective bradykinin B2 receptor antagonist; however, this is contraindicated with concomitant use of ACE inhibitors because they exert their vasodilating effect via increased bradykinin concentrations [17]. In severe or refractory cases of angioedema, patients may require intubation or cricothyroidotomy.
Conclusions
Angioedema induced by tPA is an infrequent but potentially fatal outcome of thrombolysis occurring in 1 of 50 patients, which increases to 1 of 10 in insular infarcts and 1 of 6 in individuals who are concomitantly using ACE inhibitors at the time of thrombolysis [4]. Angioedema typically presents within the hour of tPA administration and can quickly compromise the airway. Due to its severity, close monitoring of these individuals is imperative and prompt treatment is essential. Though exposed to ACE inhibitors, our patient was found to have an infarct of her posterior cerebral artery and developed angioedema after thrombolysis. This combination has rarely been documented, making this case unusual.
Figures
References:
1.. Yayan J, Onset of orolingual angioedema after treatment of acute brain ischemia with alteplase depends on the site of brain ischemia: A meta-analysis: North Am J Med Sci, 2013; 5; 589-93
2.. Rathbun K, Angioedema after thrombolysis with tissue plasminogen activator: An airway emergency: Oxf Med Case Reports, 2019; 2019(1); omy112
3.. Frohlich K, Macha K, Gerner ST, Angioedema in stroke patients with thrombolysis a lesion mapping: Stroke, 2019; 50; 1682-87
4.. Myslimi F, Capparos F, Dequatre-Ponchelle N, Orolingual angioedema during or after thrombolysis for cerebral ischemia: Stroke, 2016; 47; 1825-30
5.. Sczepanski M, Bozyk P, Institutional incidence of severe tPA-induced angioedema in ischemic cerebral vascular accidents: Crit Care Res Pract, 2018; 2018; 9360918
6.. Madden B, Chebl R, Hemi orolingual angioedema after tPA administration for acute ischemic stroke: West J Emerg Med, 2015; 16; 175-77
7.. Dewald G, A missense mutation in the plasminogen gene, within the plasminogen kringle 3 domain, in hereditary angioedema with normal C1 inhibitor: Biochem Biophys Res Commun, 2018; 498; 193-98
8.. Gauberti M, Potzeha F, Vivien D, Impact of bradykinin generation during thrombolysis in ischemic stroke: Front Med, 2018; 5; 195
9.. Engelter ST, Fluri F, Buitrago-Tellez C, Life-threatening orolingual angioedema during thrombolysis in acute ischemic stroke: J Neurol, 2005; 252; 1167-70
10.. Hurford R, Rezvani S, Kreimei M, Incidence, predictors and clinical characteristics of orolingual angio-oedema complicating thrombolysis with tissue plasminogen activator for ischaemic stroke: J Neurol Neurosurg Psychiatry, 2015; 86; 520-23
11.. Lin SY, Tang SC, Tsai LK, Orolingual angioedema after alteplase therapy of acute ischaemic stroke: Incidence and risk of prior angiotensin-converting enzyme inhibitor use: Eur J Neurol, 2014; 21; 1285-91
12.. Correia AS, Matias G, Calado S, Orolingual angioedema associated with alteplase treatment of acute stroke: A reappraisal: J Stroke Cerebrovasc Dis, 2015; 24(1); 31-40
13.. Hill MD, Lye T, Moss H, Hemi-orolingual angioedema and ACE inhibition after alteplase treatment of stroke: Neurology, 2003; 60; 1525-27
14.. Burd M, McPheeters C, Scherrer LA, Orolingual angioedema after tissue plasminogen activator administration in patients taking angiotensin-converting enzyme inhibitors: Adv Emerg Nurs J, 2019; 41(3); 204-14
15.. Powers WJ, Rabinstein AA, Ackerson T, 2018 Guidelines for the early management of patients with acute ischemic stroke: A guideline for health-care professionals from the American Heart Association/American Stroke Association: Stroke, 2018; 49; 46-99
16.. Pahs L, Droege C, Kneale H, Pancioli A, A novel approach to the treatment of orolingual angioedema after tissue plasminogen activator administration: Ann Emerg Med, 2016; 68; 345-48
17.. Dubois EA, Cohen AF, Icatibant: Br J Clin Pharmacol, 2010; 69; 425-26
Figures
Tables
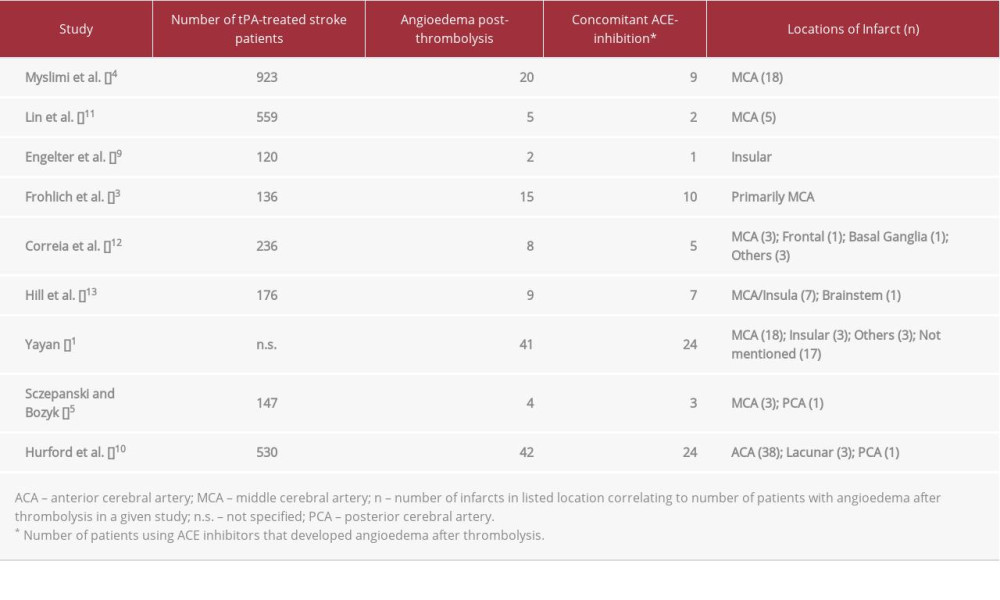 Table 1.. Comparison of studies involving tissue plasminogen activator-associated angioedema, highlighting the location of stroke and concomitant angiotensin-converting enzyme (ACE) inhibition.Table 1.. Comparison of studies involving tissue plasminogen activator-associated angioedema, highlighting the location of stroke and concomitant angiotensin-converting enzyme (ACE) inhibition.
Table 1.. Comparison of studies involving tissue plasminogen activator-associated angioedema, highlighting the location of stroke and concomitant angiotensin-converting enzyme (ACE) inhibition.Table 1.. Comparison of studies involving tissue plasminogen activator-associated angioedema, highlighting the location of stroke and concomitant angiotensin-converting enzyme (ACE) inhibition. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133