12 February 2021: Articles 
Myocardial Metastasis of Tongue Cancer: A Rare Localization
Challenging differential diagnosis, Rare disease
Marco Carbonaro1ABCDEF*, Giulia Russo1ABCDEF, Silvia Mezi2BF, Giuseppe Mancuso2BCDE, Vincenzo Paravati1AD, Francesco Barillà1AD, Carlo Gaudio1AD, Giuseppe Pannarale1ADE, Concetta Torromeo1ACDEDOI: 10.12659/AJCR.927459
Am J Case Rep 2021; 22:e927459






Abstract
BACKGROUND: Cardiac metastases of head and neck tumors are extremely rare, and antemortem diagnosis is even rarer. In most cases, patients show symptoms or electrocardiographic abnormalities and expected survival is considerably low.
CASE REPORT: A 72-year-old man was admitted to our cardiology ward with suspected endocarditis 2 months after a right hemiglossectomy for a squamous cell carcinoma. He was asymptomatic and showed no electrocardiogram abnormalities. Echocardiography showed an iso-ipoechogenic round-shaped formation at the right ventricle apex that was suspected to be a metastasis owing to 2 cardiac magnetic resonance imaging examinations showing a significant increase in its volume over 14 days. The patient was evaluated by a multidisciplinary team and referred for first-line chemotherapy with carboplatin, 5-fluoruracil, and cetuximab. He died after almost 4 months of follow-up.
CONCLUSIONS: This case presents a very rare diagnosis as well as some unique features, including the intramyocardial localization, the absence of symptoms, and electrocardiogram abnormalities. Our report shows the relevance of imaging techniques in defining even the most unusual clinical findings, and it emphasizes the significance of early recognition of cardiac masses in order to identify the appropriate medical or surgical therapy for patients.
Keywords: Cardiology, Echocardiography, Magnetic Resonance Imaging, Carcinoma, Squamous Cell, Heart Neoplasms, Tongue Neoplasms
Background
Cardiac tumors represent a rare, yet challenging diagnosis and can be differentiated into primary tumors (rates between 0.001% and 0.3%) and secondary tumors (ranging from 2.3% and 18.3%) [1]. In theory, the heart can be metastasized by any malignant neoplasm, but antemortem diagnosis is very rare because clinical manifestations are subtle or even absent, especially at an early stage [1,2]. At more advanced stages, however, metastatic tumors gradually lead to heart failure, conduction disturbances, or valvular disease resembling mitral stenosis, anginal pain, or Stokes-Adams syndrome [3]. Cardiac metastasis is more frequently detected accidentally, usually at surgery or autopsy (in 2.3–7.1% of cases) [4].
In order of frequency, tumors metastasize to the pericardium, endocardium and valves, and the myocardium. The mechanisms of metastasis to the heart remain uncertain, but explanatory hypotheses include hematogenous spread via the coronary arteries, retrograde lymphatic extension, and intracavitary diffusion either by the inferior vena cava or by pulmonary veins [2,3]. Lymphatic spread tends to give rise to pericardial metastases, as seen in lung and breast cancer, owing to their topography; whereas, hematogenous spread leads to myocardial metastases [5]. The most common primary tumors that produce cardiac metastasis are melanoma, carcinoma of the bronchus, breast carcinoma, and lymphoma. Due to their propensity for generalized hematogenous spread, malignant melanomas frequently metastasize to the heart in this manner; whereas, esophageal and breast cancers metastasize to the heart predominantly by lymphatics [5].
Case Report
A 72-year-old man received a diagnosis of tongue carcinoma in December 2018. He subsequently underwent a right subtotal hemiglossectomy with right lateral neck dissection and a reconstruction with a fasciocutaneous flap from the left thigh. Histological examination revealed poorly differentiated (G3) ulcerated squamocellular carcinoma infiltrating the muscular tissue and various metastatic lymph nodes (pT3, N2b, M0). About a month after surgery the patient was admitted to the Emergency Department for a surgical wound infection and dismissed with an oral antimicrobial therapy.
In January 2019, computed tomography-positron emission tomography (CT-PET) was performed and showed hypermetabolic activity in the patient’s tonsils and laterocervical lymph nodes. A hypermetabolic signal (standardized uptake value, maximum 15.1) was also shown in the heart at the ostium of the mitral valve and near the apex of the right ventricle (Figure 1). These images were thought to be suggestive of a septic thrombus. The patient was admitted to our cardiology ward with suspected endocarditis.
The patient presented no symptoms and, in particular, he did not report chest discomfort, palpitations, dyspnea, or syncope. Physical evaluation was normal, and an electrocardiogram (ECG) showed no significant abnormalities. The patient’s C-reactive protein and erythrocyte sedimentation rate were slightly increased. With few clinical data to confirm or exclude the suspected diagnosis of endocarditis, a better characterization of the hypermetabolic signal areas shown by CT-PET was essential.
A transthoracic echocardiography (TTE) (Figure 2A, 2B, Video 1) was done, and it showed an iso-ipoechogenic round-shaped formation at the right ventricle apex, with no signs of vascularization. The patient next underwent a cardiac magnetic resonance imaging (MRI) scan (Figure 3A, 3B, Video 2) for better tissue characterization. A round-shaped mass with a diameter of 17 mm, hardly distinguishable from the right ventricular wall, was found. The mass showed a hyperintense signal in T2-weighted images and in T1-weighted scans with late gadolinium enhancement and a hypointense signal in T1 scans with early gadolinium enhancement. These findings were suggestive of cardiac metastasis.
The patient was re-evaluated by a multidisciplinary team of oncologists, radiologists, and maxillofacial surgeons. A second TTE (Figure 4, Video 3) and a follow-up MRI scan (Figure 5A, 5B, Video 4) were done 14 days later and showed significant augmentation in the sizes of the right ventricular lesion (34×25×34 mm) and infiltration of the right ventricular free wall and the pericardial adipose tissue. This formation also showed, in the patient’s intracavitary portion, a nodular extension wedged between the right ventricular trabeculae with synchronous movement in cine sequences.
Because of the lesion localization, it was impossible to obtain a sample for histological examination. During the first weeks of his hospital stay, the patient had also developed a subcutaneous lesion that appeared as a protuberance in the right frontal area that rapidly increased in volume. This lesion was not evident on admission, nor was it reported on the initial CT-PET. It was also investigated with an MRI scan of the head and neck district, and findings suggested that it was a metastasis. An incisional biopsy of the lesion was then performed, and the results were compatible with the localization of a squamocellular carcinoma.
From February to April 2019, the patient received 2 cycles of first-line chemotherapy according to the scheme carboplatin area under the curve (AUC) of 5 on day 1, 5-fluoruracil 800 mg/m2/d from day 1 to day 5 every 21 days, along with the anti-epidermal growth factor receptor drug cetuximab, at a loading dose of 400 mg/m2 for the first cycle and then at the standard dose of 250 mg/m2 weekly [6]. Treatment toxicity was assessed every 3 weeks, according to the National Cancer Institute-Common Terminology Criteria for Adverse Events (CTCAE version 4.03, 2010).
Moderate renal toxicity with moderate anemia, associated with electrolyte imbalances, was recorded. The ECG started to show some changes, including repolarization abnormalities in the anterior leads that were not present in the first ECG. Moreover, a central venous catheter infection (that required removal of the catheter) was reported. Objective response was clinically evaluated before every cycle and by imaging after the 2 cycles. The patient was restaged by radiological imaging with a contrast-enhanced CT scan. The patient’s objective response rate was assessed according to Response Evaluation Criteria in Solid Tumors (RECIST) criteria [7]. The patient experienced progression of disease due to the appearance of a new cardiac metastasis. Because of disease progression, chemotherapy was definitively suspended, and the patient received supportive care during the rapid decline of his physical condition. The patient died in April 2019.
Discussion
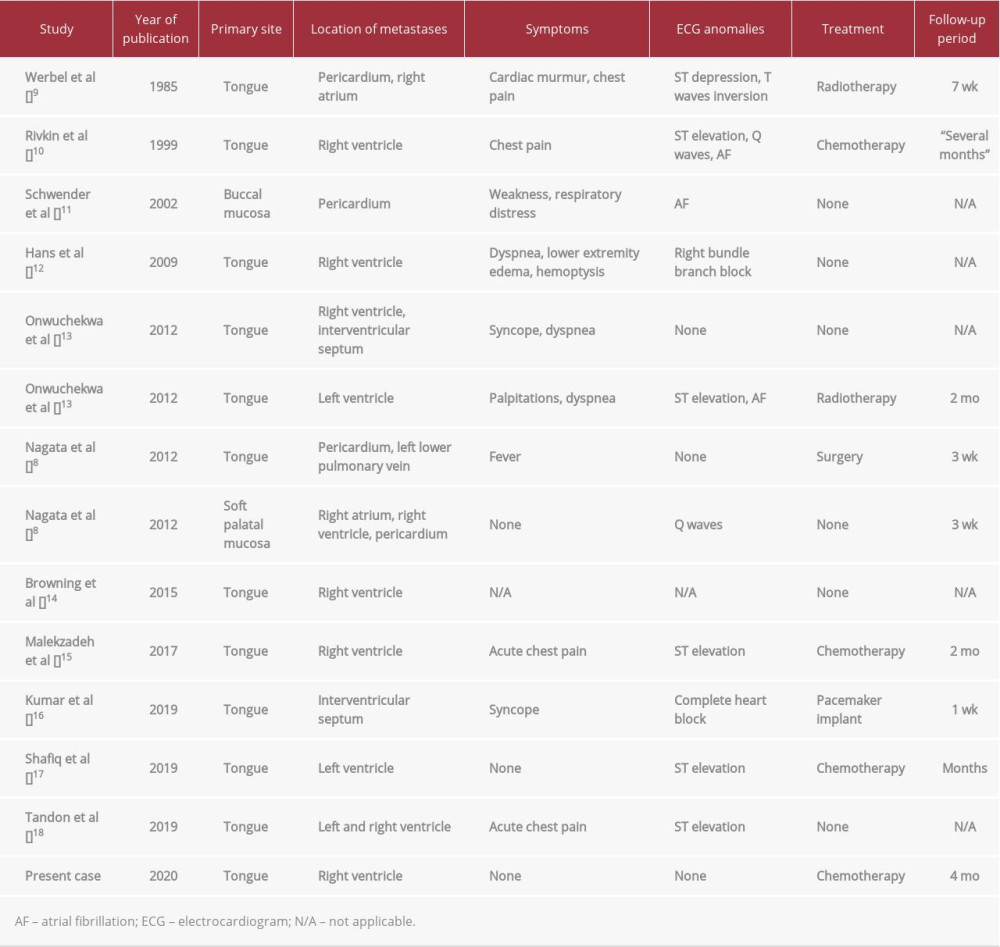
Head and neck tumors represent an extremely rare source of cardiac metastasis, with fewer than 15 cases described in the medical literature [2,5,8] (Table 1). Differential diagnosis has to include a number of clinical conditions. In our case, the main imaging finding at admission was a hypermetabolic mass described in the apex of the right ventricle and at the ostium of the mitral valve. The suspected diagnosis on admission was endocarditis. This hypothesis was subsequentially excluded based on clinical findings. The patient did not show any clinical characteristics of endocarditis. His levels of C-reactive protein and other inflammatory markers were just slightly altered, and his blood cultures were repeatedly negative. In addition, the TTE images were also highly atypical for endocarditis, with a round-shaped mass detected near the apex of the right ventricle. Other possible causes of cardiac hypermetabolic signals are primary tumors of the heart, but they are 40 times as rare as secondary tumors (with a reported prevalence in autopsy series of 0.001–0.3%). Furthermore, the most common tumor in this group is the myxoma, which generally shows very low or absent 2-[18F]fluoro-2-deoxy-d-glucose (FDG) up-take [19]. Blood thrombi can occasionally present as circular masses, but they tend to show no FDG uptake [20].
The main clinical findings that supported the diagnosis of a myocardial metastasis, even in the absence of a direct histological confirmation, were the tissue characterization and demonstration of tissue infiltration based on MRI and the significative volumetric increase of the mass in a limited time frame. The diagnosis was also reinforced by the detection of a sub-cutaneous metastasis that suggested widespread disease.
We believe that our case presents a series of particularities that stand out even in the frame of a very rare diagnosis. In our literature search we observed that symptoms or electrocardiographic abnormalities were reported in most cases. In contrast, our patient remained completely asymptomatic for months and did not show any significant abnormality in his initial ECG. We also believe that our case can be considered unusual for the intramyocardial localization because most reported patients showed pericardial or intracavitary metastasis. Life expectancy is considered to be of few weeks in most patients, while our patient had a survival of about 4 months.
Conclusions
The paucity of antemortem diagnosis of cardiac metastasis emphasizes the importance of early recognition of cardiac masses in order to determine appropriate medical or surgical therapy for patients. Our case highlights the significance of echocardiography and MRI in the antemortem detection of a single metastasis, even in the most unusual localizations.
Figures
References:
1.. Nomoto N, Tani T, Konda T, Primary and metastatic cardiac tumors: Echocardiographic diagnosis, treatment and prognosis in a 15-years single center study: J Cardiothorac Surg, 2017; 12; 103
2.. Bussani R, De-Giorgio F, Abbate A, Silvestri F, Cardiac metastases: J Clin Pathol, 2007; 60; 27-34
3.. Gassman HS, Meadows R, Baker LA, Metastatic tumors of the heart: Am J Med, 1955; 19; 357-65
4.. Al-Mamgani A, Baartman L, Baaijens M, Cardiac metastases: Int J Clin Oncol, 2008; 13; 369-72
5.. Puranik AD, Purandare NC, Sawant S, Asymptomatic myocardial metastasis from cancers of upper aero-digestive tract detected on FDG PET/CT: A series of 4 cases: Cancer Imaging, 2014; 14; 1-6
6.. Vermorken JB, Mesia R, Rivera F, Platinum-based chemotherapy plus cetuximab in head and neck cancer: N Engl J Med, 2008; 359; 1116-27
7.. Schwartz LH, Litière S, De Vries E, RECIST 1.1 – update and clarification: From the RECIST committee: Eur J Cancer, 2016; 62; 132-37
8.. Nagata S, Ota K, Nagata M, Shinohara M, Cardiac metastasis of head and neck squamous cell carcinoma: Int J Oral Maxillofac Surg, 2012; 41; 1458-62
9.. Werbel GB, Skom JH, Mehlman D, Michaelis LL, Metastatic squamous cell carcinoma to the heart. Unusual cause of angina decubitus and cardiac murmur: Chest, 1985; 88; 468-69
10.. Rivkin A, Meara JG, Li KK, Squamous cell metastasis from the tongue to the myocardium presenting as pericardial effusion: Otolaryngol Neck Surg, 1999; 120; 593-95
11.. Schwender FT, Wollner I, Kunju LP, Squamous cell carcinoma of the buccal mucosa with metastases to the pericardial cavity, lung and thyroid: Oral Oncol, 2002; 38; 114-16
12.. Hans S, Chauvet D, Sadoughi B, Brasnu DF, Cardiac metastasis after squamous cell carcinoma of the base of tongue: Am J Otolaryngol, 2009; 30; 206-8
13.. Onwuchekwa J, Banchs J, Early cardiac metastasis from squamous cell carcinoma of the tongue in 2 patients: Tex Heart Inst J, 2012; 39; 565-67
14.. Browning CM, Craft JF, Renker M, Squamous cell carcinoma of the tongue with metastasis to the right ventricle: Am J Med Sci, 2015; 349; 461-62
15.. Malekzadeh S, Platon A, Poletti PA, Cardiac metastasis of tongue squamous cell carcinoma complicated by pulmonary embolism: Medicine (Baltimore), 2017; 96; e7462
16.. Kumar D, Mankame P, Sabnis G, Nabar A, A case report: Metastatic complete heart block: Eur Heart J Case Rep, 2018; 2(4); yty131
17.. Shafiq A, Samad F, Roberts E, Squamous cell carcinoma of the tongue with metastasis to myocardium: Report of a case and literature review: Case Rep Cardiol, 2019; 2019; 1649580
18.. Tandon V, Kethireddy N, Balakumaran K, Kim AS, Metastatic squamous cell carcinoma to the heart: An unusual cause of ST elevation – a case report: Eur Heart J Case Rep, 2019; 3(2); ytz029
19.. Maurer AH, Burshteyn M, Adler LP, Steiner RM, How to differentiate benign versus malignant cardiac and paracardiac 18 F FDG uptake at oncologic PET/CT: Radiographics, 2011; 31; 1287-305
20.. Rinuncini M, Zuin M, Scaranello F, Differentiation of cardiac thrombus from cardiac tumor combining cardiac MRI and 18F-FDG-PET/CT Imaging: Int J Cardiol, 2016; 212; 94-96
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953068
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133