07 December 2020: Articles 
Testicular Ectopia in a Child’s Anterior Abdominal Wall: A Case Report and Literature Review
Challenging differential diagnosis, Congenital defects / diseases
Suliaman Mohammed Alaqeel1ABDEF, Anan Hassan Hakeem2ABDEF, Jamila Obaid Almaary1ABDEF*DOI: 10.12659/AJCR.927495
Am J Case Rep 2020; 21:e927495






Abstract
BACKGROUND: Ectopic testis is an uncommon congenital anomaly that has been reported in different sites in the body. The anterior abdominal wall is an exceptionally rare variant site for ectopic testis. The purpose of this case report is to highlight the importance of being aware of this rare clinical entity, thereby increasing the chance of preserving an ectopic testis. In addition, this case report shows how a laparoscopic approach is advantageous for better localizing and treating such rare cases, as this is the first reported case of such a condition to be managed with a laparoscopic approach.
CASE REPORT: This is a rare case of testicular ectopia in an unclassified abdominal wall defect mimicking a Spigelian hernia that occurred in a 1.5-year-old boy. He presented with congenital swelling of the right lower abdominal wall and an empty right hemiscrotum. Diagnostic laparoscopy was performed and the intraoperative findings suggested right testicular ectopia in the anterior abdominal wall defect. The right testis was herniated through an abnormal, unclassified, abdominal wall defect with both a closed inguinal ring and no defect in the semilunar line. Using a laparoscopic approach, the ectopic testis and hernia were managed successfully with primary hernia repair and single-stage orchidopexy. The patient’s postoperative recovery was uneventful. At his 10-month follow-up appointment, he had no evidence of hernia recurrence.
CONCLUSIONS: As demonstrated in this case, laparoscopic surgery, which has not been used in previously reported cases of ectopic testis, aids in proper localization and repair of an anterior abdominal wall defect along with orchidopexy.
Keywords: Abdominal Wall, Laparoscopy, orchiopexy, Hernia, Abdominal, Cryptorchidism, Child, herniorrhaphy, Infant
Background
Embryological testicular descent is a complex process that occurs in 2 distinct stages: transabdominal and inguinal-scrotal [1–3]. A failure of or deviation from this process can result in an undescended testis (UDT), known as cryptorchidism. The approximate incidence of UDT in term infants is 1.0% to 4.6%; in preterm infants, the incidence is 1.1% to 45.3% [4]. UDT is classified as congenital, acquired, or ectopic testis [3]. Testicular ectopia has been reported as femoral, perineal, pubo-penile, transverse, or abdominal. Of the known reported ectopic sites, testicular ectopia into an anterior abdominal wall is the rarest [1,2].
Here, we report on an infant with an ectopic testis herniating through an abnormal, unclassified, anterior, abdominal wall defect located lateral to a closed, internal inguinal ring. The other reported similar cases in the literature have described an ectopic testis herniating through either the external or the internal ring, looping up and finally being located within the anterior abdominal wall.
Case Report
A 1.5-year-old, full-term male presented to the clinic with an empty right scrotum, undescended right testis, and asymptomatic ipsilateral lower abdominal wall swelling, all of which were present since birth. Physical examination revealed a reducible abdominal wall hernia in the right lower quadrant, empty right hemiscrotum, and a nonpalpable right testis. The patient’s left testis was located in its respective hemiscrotal sac and normal in size and appearance. The rest of his physical examination was unremarkable.
Our initial impression was that the patient had a right abdominal UDT associated with a Spigelian hernia. However, abdomen/groin ultrasound with Doppler demonstrated an abdominal wall defect containing bowel loops and an ectopic right testicle that had adequate color flow and a homogeneous echo texture that measured 1.1 cm (Figure 1).
Diagnostic laparoscopy was performed (Figure 2). Intraoperatively, the patient’s right testis, vas, and vessels herniated into an abnormal defect in the anterior abdominal wall lateral to the internal ring. The right internal ring was closed, with no patent processus vaginalis. No defects were found through the semilunar line (Figure 3). The right ectopic testis was normal size, measuring 1.51 cm. After the ectopic testis was mobilized and reduced, primary closure of the hernia defect was performed, followed by a single-stage laparoscopic orchidopexy. The testis was exteriorized through the Hesselbach triangle lateral to the urinary bladder and medial to the inferior epigastric vessels and then affixed to the scrotum under no tension (Figure 4).
Postoperatively, the child recovered well and he was discharged on the day of surgery. He had no evidence of hernia recurrence, and his testis remained fixed in the right hemiscrotum during the 10-month follow-up period.
Discussion
In utero, normal testicular development and descent rely on the interplay of multiple factors, including genetic, hormonal, and mechanical factors [1,2]. The normal process of embryological testicular descent occurs in 2 distinct stages: intra-abdominal and inguinoscrotal [5,6]. When any of the involved steps are interrupted, abnormal testicular descent occurs [7]. The “Tails of Lockwood” or “traction theory” provides a hypothesis for the cause of testicular ectopia. The distal part of the gubernaculum is a smooth, jelly-like mass that can transform into a chain of muscle fibers. These fibers are liable to contract and pull the testis down into the scrotum. Lockwood’s theory proposed that any abnormal development of the gubernaculum tail could pull the testis into an aberrant, abnormal position [8].
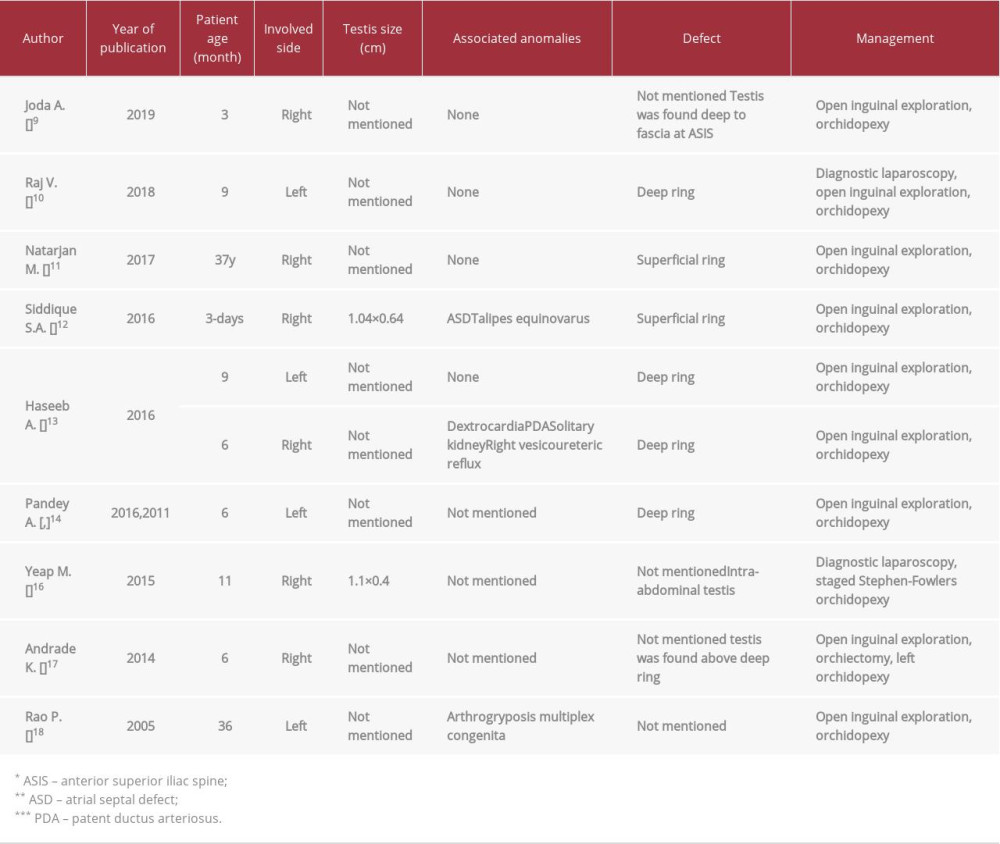
Of the known ectopic sites, the anterior abdominal wall is the rarest site of testicular ectopia [1,2]. A total of 10 reported cases have been described in the English literature [9–18]. Only 1 case has been reported in an adult [11]. To our knowledge, the present case is the 11th with special attention to the type of hernia defect (Table 1).
Spigelian-cryptorchidism syndrome has been described in the English literature as a new congenital syndrome. It is distinct from an ordinary undescended testis and from Spigelian hernia.
Seventy-five percent of male infants with Spigelian hernias had a coexisting Spigelian hernia and ipsilateral undescended testis, and the testis was found inside the hernia sac in 87% of these children [19]. Our patient’s initial clinical presentation was indicative of Spigelian hernia, with no palpable content and nonpalpable abdominal UDT. With the aid of imaging and diagnostic laparoscopy, it was determined not to be such a case. The right testis was found to be ectopic within an abdominal wall defect that was lateral and superior to the internal inguinal ring. There is no known name or classification for such a defect. The internal inguinal ring was closed, with no patent processus vaginalis, and no defects within the semilunar line.
Two of the reported cases had similar presentations of ectopic testis in the abdominal wall mimicking a Spigelian hernia [11,14,15]. The first reported case was a 37-year-old man who presented with acute severe right iliac fossa pain and an irreducible mass [11]. The second reported case was a 6-month-old boy who presented with a reducible mass in his left lower abdomen [14,15]. Although the previous 2 cases were initially diagnosed as Spigelian hernias, no semilunar line defects were identified at surgical exploration. During open exploration, the defect was found to be in either the internal or the external inguinal ring.
Seven other cases of abdominal testicular ectopia have been reported. In 5 cases, the patients underwent open groin exploration and orchidopexy, except in the 1 case in which the testis was torsed, nonviable, and removed [17]. Diagnostic laparos-copy was performed in 2 patients; the surgery was converted to a groin exploration in 1 case [10], and in the other case, scrotal orchidopexy was performed after the testicular vessel was scarified (single-stage Fowler-Stephens technique) [16].
The advantage of preoperative abdominal wall imaging has been addressed, including with ultrasound, cord tracking techniques with ultrasound, and magnetic resonance. Moreover, laparoscopy has been documented to have significant advantages.
With a laparoscopic approach, the abdominal wall defect and the position of the testes can be better characterized and assessed, and different technical options can be used to repair and fix an ectopic testis [3,20,21].
Conclusions
The present case has been reported because of the rarity of the condition. It highlights the importance of clinical awareness of the condition and preoperative imaging for it, as well as the usefulness of laparoscopy for confirming the exact diagnosis and managing ectopic testis, thereby increasing the possibility of preserving an ectopic testis.
Figures
References:
1.. Husmann DA, Levy JB, Current concepts in the pathophysiology of testicular undescent: Urology, 1995; 46; 267-76
2.. Pescovitz OH, Eugster EA: Pediatric endocrinology mechanisms, manifestations, and management, 2004; 256-67, Philadelphia, Lippincott Williams & Wilkins
3.. Vikraman J, Hutson JM, Li R, Thorup J, The undescended testis: Clinical management and scientific advances: Semin Pediatr Surg, 2016; 25(4); 241-48
4.. Sijstermans K, Hack WWM, Meijer RW, The frequency of undescended testis from birth to adulthood: A review: Int J Androl, 2008; 31; 1-11
5.. Heyns CF, The gubernaculum during testicular descent in the human fetus: J Anat, 1987; 153; 93-112
6.. Barteczko KJ, Jacob MI, The testicular descent in human. Origin, development and fate of the gubernaculum Hunteri, processus vaginalis peritonei, and gonadal ligaments: Adv Anat Embryol Cell Biol, 2000; 156; III-X
7.. Hutson JM, Southwell BR, LiR , The regulation of testicular descent and the effects of cryptorchidism: Endocr Rev, 2013; 34(5); 725-52
8.. Lockwood CB, Development and transition of the testis, normal and abnormal: J Anat Physiol, 1888; 22; 505-41
9.. Joda A, Five different cases of ectopic testes in children: A self-experience with literature review: World J Ped Surg, 2019; 2(3); e000068
10.. Raj V, Redkar R, Joshi S, Abdominal wall ectopic testis – case report and review of literature: J Pediatr Surg Case Rep, 2018; 31; 26-28
11.. Natarajan M, Alnajjar HM, Woodward CI, Abdominal wall ectopic testis torsion mimicking a Spigelian hernia in an adult: Ann R Coll Surg Engl, 2017; 99(2); e65-68
12.. Siddiqui SA, Marei TI, Al-Makhaita G, Testicular ectopia in the anterior abdominal wall of a neonate: A rare site of ectopic testis: Am J Case Rep, 2016; 17; 490-93
13.. Haseeb AA, Okasha S, Elbarawy A, Anterior abdominal wall ectopic testes: A report of two cases: Ann Pediatr Surg, 2016; 12; 25-27
14.. Pandey A, Gupta V, Singh SP, Verma R, Undescended testis and swelling in spigelian belt: Not always a spigelian hernia: J Indian Assoc Pediatr Surg, 2016; 21(1); 44-45
15.. Pandey A, Rawat J, Pandey J, Abdominal wall ectopic testis mimicking spigelian hernia: J Pediatr Surg, 2011; 46(2); 415-16
16.. Yeap MC, Chen JC, Testicular ectopia underneath anterior abdominal wall following fetal peritonitis: Pediatr Neonatol, 2015; 56(4); 275-76
17.. Andrade K, Smith S, Goodarzian F, An infant with an ectopic torsed testis in the abdominal wall: Emerg Radiol, 2014; 21(2); 223-25
18.. Rao PL, Gupta V, Kumar V, Anterior abdominal wall – an unusual site for ectopic testis: Pediatr Surg Int, 2005; 21(8); 687-88
19.. Rushfeldt C, Oltmanns G, Vonen B, Spigelian-cryptorchidism syndrome: A case report and discussion of the basic elements in a possibly new congenital syndrome: Pediatr Surg Int, 2010; 26(9); 939-42
20.. Fahlenkamp D, Rassweiler J, Fornara P, Complications of laparoscopic procedures in urology: Experience with 2,407 procedures at 4 German centers: J Urol, 1999; 162(3 Pt 1); 765-70
21.. Thorup JM, Cortes D, Visfeldt J, Germ cells may survive clipping and division of the spermatic vessels in surgery for intra-abdominal testes: J Urol, 1999; 162(3 Pt 1); 872-74
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133