12 January 2021: Articles 
Ptosis and Miosis Associated with Fibrosing Mediastinitis
Challenging differential diagnosis, Unusual or unexpected effect of treatment, Rare disease
Shakeel Ahmed1AEF*, Mansoor Hameed12EF, Merlin M. Thomas12EF, Khezar S. Syed1EF, Irfan U. Haq1F, Abbas AlAbbas1DFDOI: 10.12659/AJCR.927556
Am J Case Rep 2021; 22:e927556






Abstract
BACKGROUND: Fibrosing mediastinitis is a rarely seen, progressive disease. It results from an excessive fibrotic reaction in the mediastinum. We describe a presentation of fibrosing mediastinitis that, to our knowledge, has never been seen before.
CASE REPORT: A 30-year-old female Colombian flight attendant presented with a right eyelid droop. Examination revealed partial right-sided ptosis and miosis but no anhidrosis. An ill-defined firm swelling was palpable at the root of the neck. Chest radiography revealed a widened mediastinum, and computerized tomography (CT) showed a right paratracheal mass without calcification extending to the thoracic inlet, encasing multiple blood vessels. All basic blood tests, magnetic resonance imaging of the head, and ultrasound Doppler of the neck vessels were normal. History and work up for infections including fungal diseases, granulomatous diseases, vasculitis, and autoimmune diseases were negative. Positron emission tomography (PET) showed significant FDG uptake in the mediastinum. Mediastinal biopsy was histologically consistent with fibrosing mediastinitis. All relevant immunohistochemistry and microbiological studies were negative. Subsequently, the patient developed signs of superior vena cava compression; this was managed by balloon angioplasty, which resulted in improvement of symptoms. However, over time, her symptoms worsened progressively, resulting in a left-sided ptosis and radiological progression of the mass on CT. She received treatment with rituximab and concomitant steroids, which yielded excellent results: the treatment led to both resolution of her symptoms and regression of the mass and its metabolic activity on PET scan.
CONCLUSIONS: Fibrosing mediastinitis can present with an incomplete Horner’s syndrome. Treatment with rituximab and steroids shows promising results in select cases of metabolically active idiopathic fibrosing mediastinitis.
Keywords: Fibrosis, Fluorodeoxyglucose F18, Tomography, Spiral Computed, mediastinitis, Positron-Emission Tomography, Vena Cava, Superior, Blepharoptosis, Miosis, Sclerosis
Background
Fibrosing mediastinitis (FM) is caused by an excessive fibroinflammatory reaction within the mediastinum. The expansive growth of fibroinflammatory tissue results in narrowing and obstruction of vital vascular structures, airways, and/or the esophagus, with associated symptoms [1]. The pathogenesis of FM remains unclear, with the current consensus being that it is a hypersensitivity reaction, with an association with microorganisms like mycobacteria,
Case Report
A previously healthy 30-year-old female Colombian flight attendant presented with drooping of her right eyelid, along with numbness over the right side of her face of 6 weeks’ duration. The droop was more pronounced on waking up in the morning or during strenuous work and gradually improved through the day. There was no anhidrosis. There was a gradual increase and persistence of the drooping over a period of 6 weeks. She had an associated intermittent dry cough, chest discomfort, and palpitations, mainly when supine. She denied any visual disturbances, eye swelling, headaches, focal neurological symptoms, hoarseness of voice, anorexia, or weight loss. There was no known exposure or prior history of tuberculosis or histoplasmosis infection. Drug history revealed contraceptives use only, using subcutaneous progesterone depot. Her family history was significant for her grandmother having had lung cancer.
On examination, the patient looked well, with normal vital signs and oxygen saturation on room air. The neurological examination was unremarkable except for a partial right-sided ptosis and miosis, but no anhidrosis. A chest examination revealed normal breath sounds, with an ill-defined firm palpable swelling at the root of the neck. There were no signs of superior vena cava obstruction at initial presentation, and no palpable cervical or axillary lymphadenopathy. Cardiovascular and abdominal examinations were also normal.
Baseline investigations, including complete blood count, liver function, and renal function, were within normal range. An initial chest radiograph revealed a widened mediastinum. CT of the chest with contrast showed a right paratracheal mass of 35x29x63 mm encasing the right brachiocephalic, internal jugular, and subclavian veins, and the right carotid and subclavian arteries (Figure 1A, 1B). Other laboratory tests, including an autoimmune panel for antibodies including anti-nuclear antibody and anti-neutrophil cytoplasmic antibody, were negative. She underwent a mediastinoscopy and biopsies of a glistening hard mass. Histological analysis revealed areas of dense fibrous collagen and adipose tissue, suggestive of FM (Figure 2). There was no evidence of malignancy and flow cytometry revealed a polyclonal B cell population. Immunohistochemistry analysis for lymphoma, fungi, and stains for IgG4 disease were all negative. Smears/stains and cultures of sputum and tissue biopsies were negative for acid-fast bacilli.
Magnetic resonance imaging/angiography of the head and neck ruled out any intracranial/cervical pathology or carotid dissection. Ultrasound Doppler of the neck vessels was also normal. She was followed up for 8 months with no progression of symptoms, when she developed signs of superior vena cava (SVC) compression with facial swelling, and mild dizziness on exertion. An examination showed distended veins in the neck and upper chest with visible collaterals. The chest CT was repeated, which revealed the mass now encasing the right subclavian artery, subclavian vein, and both common carotids proximally, along with the distal part of the internal jugular vein and SVC with mild compression of the right subclavian and internal jugular veins. She underwent 2 sessions of SVC balloon angioplasty 6 weeks apart, resulting in a remarkable improvement of her symptom complex. She now noticed the right-side partial ptosis during physical stress and fatigue only.
A PET scan showed the lesion to be fluorodeoxyglucose avid with standardized uptake value max ranging up to 9.4 (Figure 3A, 3B). Treatment with immunosuppressants was discussed with her at this point, but she opted for follow-up and close observation. Over the next 10 months, she developed a left-sided ptosis as well. A repeat chest and neck CT now showed radiological progression, with the mass extending toward the left side, with moderate focal stenosis of the medial left subclavian vein and lower left internal jugular vein and severe stenosis of the left innominate and right innominate vein/upper aspect of the SVC.
Due to the progressive symptoms, a treatment trial with rituximab and steroids was initiated in agreement with the patient.
She received 2 doses of rituximab 2 weeks apart and was started on 1 mg/kg of prednisolone to be tapered over a 3- to 4-month period. She was also given
Discussion
Fibrosing mediastinitis is a rare, chronic fibro-inflammatory disease that develops as a consequence of an excessive fibrotic reaction within the mediastinum and eventually results in compression of the vital structures. Presentation of FM is clinically variable, with an incidental pickup on CT or MRI scans in about 40% of the cases. Compression or occlusion of the mediastinal structures like the tracheobronchial tree, esophagus, pulmonary vessels, and SVC results from its progressive nature, and this determines the clinical presentation of the disorder [1]. The most frequent presenting symptoms include cough, shortness of breath, hemoptysis, and chest pain. SVC syndrome is also a common manifestation of FM. It may occur in up to 42% of patients and requires revascularization to prevent hemodynamic sequelae [2].
To the best of our knowledge, there have been no reported cases of FM presenting initially with ptosis or incomplete Horner’s syndrome (miosis and ptosis without anhidrosis). Horner’s syndrome (unilateral ptosis, miosis, and facial anhidrosis) results from the interruption of the ipsilateral sympathetic pathway. Its etiology can be divided into 3 subtypes, according to the location of the interruption: central (first-order neurons), preganglionic (second-order neurons), and postganglionic (third-order neurons).
From the superior cervical ganglion arise the postganglionic neurons, which move as a plexus in the wall of the internal carotid arteries (ICA) and enter the cavernous sinus. Classically, an incomplete Horner’s results from ICA lesions like spontaneous dissection, severe atherosclerosis, acute thrombosis, aneurysms, arteritis, trauma, fibromuscular dysplasia, and connective tissue problems like Ehler–Danlos and Marfan’s syndrome. This occurs because only the sympathetic fibers in the internal carotid plexus are affected, with sparing of the external carotid plexus, which supplies the facial sweat glands. Compression of the carotid sympathetic neurons can also result in Horner’s syndrome, mainly because of mass lesions in the neck, including inflammatory masses, tumors, and lymphadenopathy [3]. We postulate that our patient’s incomplete Horner’s syndrome resulted from either irritation of or compression of the postganglionic nerve fibers in the carotid plexus by the fibrotic mass in the mediastinum, leading to the unique presenting symptoms.
The etiology of FM remains unclear. Several triggers, such as fungal infections due to
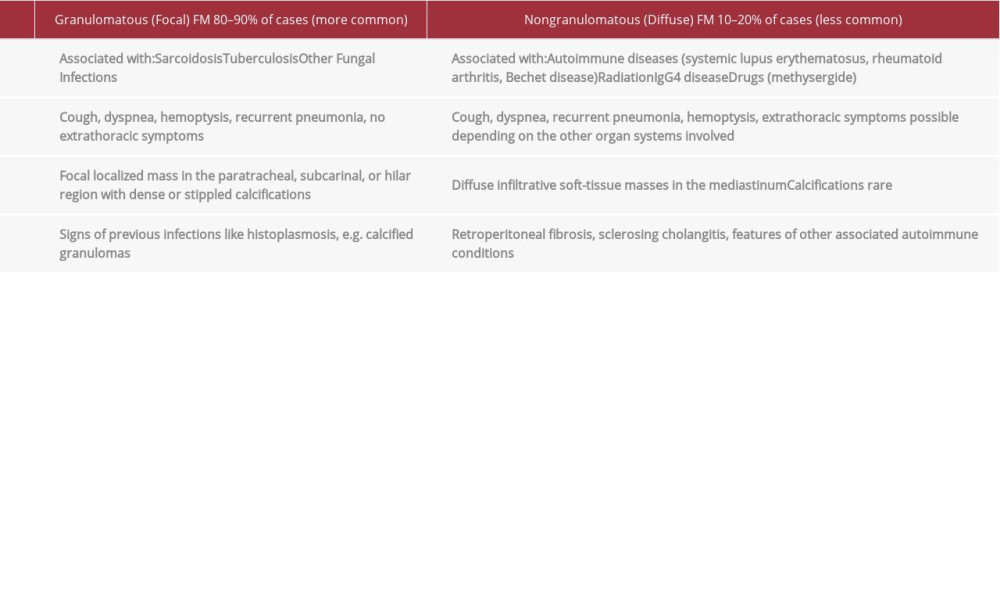
Granulomatous FM can occur as a sequela of TB or due to an abnormal immunological response to
The idiopathic or nongranulomatous subtype may be associated with drugs, an underlying autoimmune disorder, or prior radiation. Radiologically, it shows soft-tissue masses in the mediastinum without calcifications, depicting a rather diffuse infiltrative process. Nongranulomatous FM is the less common subtype. Although its true prevalence is not known, it is thought that about 10–20% of all cases of FM are of this sub-type [4]. A cohort of patients with nongranulomatous FM show immunological and histopathological features falling under the spectrum of IgG4-related disease. Similarly, other fibrotic conditions like retroperitoneal fibrosis, orbital pseudotumors, and primary sclerosing cholangitis can also be associated with IgG4-related disease. The radiological appearance of nongranulomatous FM makes its diagnosis much more challenging, as the appearance of this subtype can mimic various conditions, including malignancy. The absence of calcifications and typical patient characteristics often necessitates tissue biopsies for histological assessments, microbiological cultures, and immunohistochemical staining [5] (Table 1). Our case fits into the rare nongranulomatous idiopathic subtype with a very unusual initial presentation which has not been reported before.
The prognosis and natural history of idiopathic FM is poorly understood in large part because case series are small and include only selected symptomatic patients with often-incomplete follow-up. However, the prognosis is observed to be distinctly worse with bilateral mediastinal involvement. Although some case reports suggest spontaneous remission, they are often reports from before the advent of CT or had an incorrect initial diagnosis, likely reflecting mediastinal granulomas, which are a different sequela of histoplasmosis [6].
There are no established medical treatment options available for either form of FM. Therapeutic approaches should therefore be guided and driven by consideration of how specific mediastinal structures have been compromised by the condition, and the resulting extent of the clinical symptoms. Treatment options include medical, surgical, interventional radiological, and palliative measures [7].
Although surgical interventions like mediastinotomies can help to determine the extent of vascular involvement, their use in decompression of the involved structures is complex and risky given the difficulties of excision of the excessive fibrous tissue growth often found to be invading and infiltrating the surrounding vessels. Patients with non-functional lung parenchyma have been reported to have had lobectomies and pneumonectomies [8].
Vascular compression, however, can be treated effectively, providing symptomatic relief through interventional radiological procedures like balloon angioplasty, with or without intravascular stenting. Albers et al. [9] reported its effectiveness in providing symptomatic relief in up to 87% of patients. In accordance with these results, our patient showed symptomatic relief after angioplasty alone. Stent placement can be tricky in FM given the higher pressures required for stent deployment in compressed vessels. Re-stenting due to progressive fibrosis, stent collapse, or thrombosis is reported in up to 28% of cases, with a median time to recurrence of 115 months [9]. In similar fashion, endobronchial stents have been used to treat compressed airways but require repeat procedures owing to similar issues to those encountered with intravascular stents.
Medically, some isolated case reports cite improvement of symptoms with the use of corticosteroids and tamoxifen, although corticosteroids are not believed to be beneficial [10,11]. However, there have been no prospective studies or randomized clinical trials to date. Therefore, we suggest using corticosteroids for patients with nongranulomatous FM, especially in those with IgG4- or sarcoid-related disease, where it has shown some benefit [5].
Immunosuppressants like mycophenolate mofetil and methotrexate have also been used in combination with steroids in case reports showing benefits for idiopathic mediastinal fibrosis [12,13]. The effectiveness of these treatments has not been established on a long-term basis; the availability of reports from individual cases only makes it impossible to assess whether the response was related to the treatment or not. Further studies providing long-term efficacy data are hence necessary.
Rituximab, which is a monoclonal antibody treatment that decreases B lymphocytes, has been proposed as an investigational therapy (off-label) due to the possible pathogenic role of B lymphocytes in FM. Westerly et al. [14] studied this in 3 PET-positive patients with histoplasmosis-related FM who showed improvement in clinical symptoms, mass size, and metabolic activity. Their study suggests that some patients have ongoing B cell-mediated inflammation, which responds to B cell depletion [14]. In 2 case series abstracts from the Mayo Clinic, with 12 and 17 patients, respectively, with progressive and metabolically active FM on PET CT with airway and vascular compromise and granulomatous or IgG4-related FM, treatment with a regimen of 2 doses of 1000 mg IV rituximab with 8–10 weeks of tapering prednisolone resulted in symptomatic and radiologic improvement at 3–6 months [15,16]. It was unclear, however, whether the second abstract was a continuation of the first study or a separate original study. Retreatment with rituximab without prednisolone or active surveillance depends on clinical response and imaging findings. We chose to treat our patient with a similar regimen. Improvement of clinical symptoms, mass size, and metabolic activity on PET scan in our case also highlights the possible benefits in select patients of rituximab with concomitant steroids for progressive idiopathic FM. The hypothesis that a significant pathogenic role is played by B lymphocytes detected in FM tissue is supported by our report as well. This novel mechanism-based treatment approach through rituximab therefore deserves further investigation through prospective studies and randomized controlled trials.
Conclusions
We present the first case of progressive idiopathic FM with a never-before seen initial presenting symptom of incomplete Horner’s syndrome. We conclude that FM should be a differential diagnosis in patients presenting with ptosis, miosis, and widened mediastinum, especially without additional neurological features, a negative autoimmune screen, infection, or malignancy, as these symptoms can present with compression of any mediastinal structure. Furthermore, treatment with rituximab and steroids in select cases of FM shows promising results; therefore, its use should be considered in clinical practice and its role deserves further investigation and prospective trials.
Figures
References:
1.. Rossi GM, Emmi G, Corradi D, Idiopathic mediastinal fibrosis: A systemic immune mediated disorder. A case series and a review of the literature: Clin Rev Allergy Immunol, 2017; 52(3); 446-59
2.. Deshwal H, Ghosh S, Magruder K, A review of endovascular stenting for superior vena cava syndrome in fibrosing mediastinitis: Vasc Med, 2020; 25(2); 174-83
3.. Kanagalingam S, Miller NR, Horner syndrome: Clinical perspectives: Eye Brain, 2015; 7; 35-46
4.. Garrana SH, Buckley JR, Rosado-de-Christenson ML, Multimodality imaging of focal and diffuse fibrosing mediastinitis: Radiographics, 2019; 39(3); 651-67
5.. Peikert T, Colby TV, Midthun DE, Fibrosing mediastinitis: Clinical presentation, therapeutic outcomes, and adaptive immune response: Medicine (Baltimore), 2011; 90(6); 412-23
6.. Lima TD, Marchiori E, Capone D, Fibrosing mediastinitis: A case report: Radiol Bras, 2009; 42(5); 337-39
7.. Kuranga AO, Eubank AM, Bowling MR, Fibrosing mediastinitis: A review of epidemiology, diagnosis and management: Int J Respir Pulm Med, 2018; 5; 079
8.. Arbra CH, Valentino JD, Martin JT, Vascular sequelae of mediastinal fibrosis: Asian Cardiovasc Thorac Ann, 2015; 23; 36-41
9.. Albers EL, Pugh ME, Hill KD, Percutaneous vascular stent implantation as treatment for central vascular obstruction due to fibrosing mediastinitis: Circulation, 2011; 123; 1391-99
10.. Ikeda K, Nomori H, Mori T, Successful steroid treatment for fibrosing mediastinitis and sclerosing cervicitis: Ann Thorac Surg, 2007; 83(3); 1199-201
11.. Savelli BA, Parshley M, Morganroth ML, Successful treatment of sclerosing cervicitis and fibrosing mediastinitis with tamoxifen: Chest, 1997; 111(4); 1137-40
12.. Witschi M, Gugger M, Nicod LP, Treatment of mediastinal fibrosis with mycophenolate mofetil: Respiration, 2009; 78(3); 330-33
13.. Joury AU, Al Boukai AA, Kashour TS, Severe fibrosing mediastinitis with atypical presentation: Effective control with novel therapeutic approach: Ann Thorac Med, 2017; 12(3); 209-12
14.. Westerly BD, Johnson GB, Maldonado F, Targeting B lymphocytes in progressive fibrosing mediastinitis: Am J Respir Crit Care Med, 2014; 190(9); 1069-71
15.. Mirza S, Specks U, Keogh K, Rituximab in the management of complicated fibrosing mediastinitis: The Mayo Clinic experience: Am J Respir Crit Care Med, 2017; 195; A7121
16.. Varghese C, Johnson G, Eiken P, Tobias P, Late breaking abstract – Rituximab limits the progression of fibrosing mediastinitis: Eur Respir J, 2019; 54; OA5325
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133