22 January 2021: Articles 
A 64-Year-Old Man with Low Back Pain Due to Lumbar Discitis
Unknown etiology
Harshil Bhatt1EF*, Sandeep Singh2EFDOI: 10.12659/AJCR.928014
Am J Case Rep 2021; 22:e928014






Abstract
BACKGROUND: Lumbar discitis caused by Clostridium perfringens is extremely rare. There have only been 7 published cases of confirmed discitis caused by Clostridium perfringens. We write this report to underscore this unusual relationship by discussing an additional case and providing a review of the previously published cases so clinicians can adequately evaluate and treat patients presenting with discitis.
CASE REPORT: A 64-year-old morbidly obese man presented with an acute onset of worsening back pain and generalized weakness after incurring physical trauma related to falling. Additionally, he also developed fever and chills before the presentation. Based on the clinical presentation and elevated serum levels of inflammatory markers, magnetic resonance imaging was ordered, which showed L5–S1 discitis with extension of infection into the epidural space. Fluoroscopy-guided aspiration of the L5–S1 epidural space facilitated the detection of Clostridium perfringens as the involved pathogen. Based on the antibiotic susceptibility report, the patient was treated with intravenous ampicillin for 8 weeks, after which his symptoms resolved.
CONCLUSIONS: Diagnosis of discitis can be very challenging due to its ambiguous clinical presentation, especially in the elderly population due to the presence of underlying degenerative changes. Even though Clostridium perfringens remains a rare cause of lumbar discitis, it should be considered as a pathogen capable of causing infection of the vertebrae and intervertebral discs, thus allowing clinicians to make necessary diagnostic evaluations to provide appropriate targeted treatment to patients presenting with discitis.
Keywords: Clostridium perfringens, Discitis, intervertebral disc, Spine, Clostridium Infections, Low Back Pain, Lumbar Vertebrae, Magnetic Resonance Imaging
Background
Case Report
A 67-year-old man presented to the Emergency Department (ED) with complaints of generalized weakness for 4 days. He had repeatedly fallen at home 3 days prior to the arrival in the ED and he had a dull lower-back pain since then. The pain was controlled for a couple of days, but prior to his presentation to the ED, he noted that his pain was worsening. In addition, he noted generalized weakness without any lower-extremity weakness. He developed fever and chills at home but did not take his temperature. He did not report any productive cough, dysuria, hematuria, bowel/bladder incontinence, nausea, vomiting, diarrhea, headache, abdominal pain, or leg swelling. Hiss past medical history was significant for hypothyroidism, diabetes mellitus type 2, morbid obesity (weight 140 kg), and gout. His medication list included levothyroxine, metformin, and allopurinol. His surgical history included bilateral rotator cuff surgeries, right hammertoes, bilateral cataracts status after extraction, and colonoscopy. Family history was significant for hypertension in his father. He had never smoked cigarettes and denied alcohol use or use of illicit substances. He was allergic to ciprofloxacin (reaction unknown).
On examination, the patient had mild tachypnea and was mildly febrile. His vital signs examination revealed blood pressure of 126/76 mmHg, heart rate of 104 beats per minute, temperature of 39°C (102.3°F), respiratory rate of 18 breaths per minute, and oxygen saturation of 94% on nasal cannula at 2 liters. His mucus membranes were slightly dry. There were no crackles or rhonchi on respiratory examination. He did not have any hepatosplenomegaly or abdominal tenderness on examination. An examination of his back revealed mild tenderness on palpation of the lumbosacral spine. He did not have tenderness on palpation of cervical or thoracic spines. He had no palpable paraspinal muscle spasm. Neurologically, sensation was intact to light touch in all lower extremities, but subjectively decreased in the feet. He had 5/5 strength in his bilateral extensor hallucis longus, peroneals, gastroc soleus complex, hamstrings, quadriceps, and iliopsoas. He had no pain with range of motion of the hips. He had negative straight leg raise bilaterally. He had bilateral down-going toes with Babinski testing. He had a slow, steady gait. He was alert, awake, and oriented to time, place, and person. A skin exam showed no lesions or rash. Results of the systemic examination were within normal limits otherwise.
Laboratory studies on presentation showed leukocytosis (17.2 k/uL) with bands (17%), mild thrombocytopenia (158 k/uL), hyperglycemia (235 mg/dL), lactic acidosis (3.5 mmol/L), elevated D-dimer (635 ng/ml), elevated ESR (erythrocyte sedimentation rate – 50 mm/h), elevated CRP (C-reactive protein – 194 mg/L), and normal renal function (Table 1). Urine analysis did not suggest urinary tract infection. A chest X-ray did not show any abnormal findings. A computed tomography (CT) angiogram of the chest was done to rule out pulmonary embolism and it did not show any signs of pulmonary embolism or pneumonia, but showed bibasilar atelectasis. A lumbar spine X-ray showed lumbar spondylosis but no evidence of fracture.
Due to back pain and elevated inflammatory markers, a magnetic resonance imaging (MRI) of the lumbosacral spine with and without contrast was obtained. It showed abnormal thin enhancement within the L5–S1 disc contiguous with infiltrative enhancement in the epidural space of the lumbosacral junction, concerning for discitis with extension of infection into the epidural space. No large focal fluid collection was identified to suggest a drainable abscess formation. Degenerative disc disease was present (Figure 1). Blood cultures were obtained as well. He was started on IV ceftriaxone 2 g and IV vancomycin empirically based on the MRI findings.
The patient also underwent fluoroscopy-guided L5–S1 aspiration of the epidural space, and 2 mL of brown blood-tinged fluid was removed and sent for culture. The procedure was performed after starting the empiric antibiotics. An initial gram stain was negative. Meanwhile, the patient was continued on antibiotic and other supportive care. His back pain improved, and his fever also resolved. White cell counts gradually improved. Inflammatory markers also improved (Table 1). He slowly started working with physical therapy.
After 4 days, his spinal fluid cultures grew light growth of slow-growing anaerobic
Discussion
Only 7 confirmed cases of
Among the 7 reported cases, 2 had diverticular disease as a potential risk factor, and hematogenous dissemination of
We postulate that our patient’s discitis likely originated from the gastrointestinal tract after infiltrating the vascular submucosal tissue, which led to its dissemination to the lumbar intervertebral disc area.
Our patient was on empiric IV ceftriaxone and IV vancomycin for 4 days until identification of
Additionally, while the presented case shares some similarities with the previously reported cases, it does contain several differences. For example, the time between onset of symptoms and adequate diagnosis was several weeks to months in the previous cases. Our case resulted in an adequate diagnosis in only 4 days. This shows the need for prompt diagnosis allowing for the use of targeted antibiotic therapy early in the course of the disease to improve morbidity. Not all previously reported cases identified gas in the lesions. Beguiristain’s and Yong’s case reports did not report lesions with gas. We believe that in our case the time between the onset and diagnosis was the key, and the diagnosis was made rather quickly before gas could form within the lesions.
Conclusions
Although
References:
1.. Lotte R, Popoff MR, Degand N: J Clin Microbiol, 2014; 52; 3813-15
2.. Caudron A, Grados F, Boubrit Y: Joint Bone Spine, 2008; 75; 232-34
3.. Bednar DA: J Spinal Disord Tech, 2002; 15; 172-74
4.. Pate D, Katz A, Clostridia discitis: A case report: Arthritis Rheum, 1979; 22; 1039-40
5.. Beguiristain JL, de Pablos J, Llombart R: Spine, 1986; 11; 170-72
6.. Seller M, Burghardt RD, Rolling T: Br J Neurosurg, 2018; 32(5); 574-76
7.. Yong CH, Lam M: BMJ Case Rep, 2017; 2017; bcr2017220646
8.. , 2018 www.cdc.gov/foodsafety/diseases/clostridium-perfringens.html
9.. Yang CC, Hsu PC, Chang HJ: Int J Infect Dis, 2013; 17; e955-60
10.. Bernard L, Dinh A, Ghout I, Antibiotic treatment for 6 weeks versus 12 weeks in patients with pyogenic vertebral osteomyelitis: An open-label, non-inferiority, randomised, controlled trial: Lancet, 2015; 385; 875-82
Figures
Tables
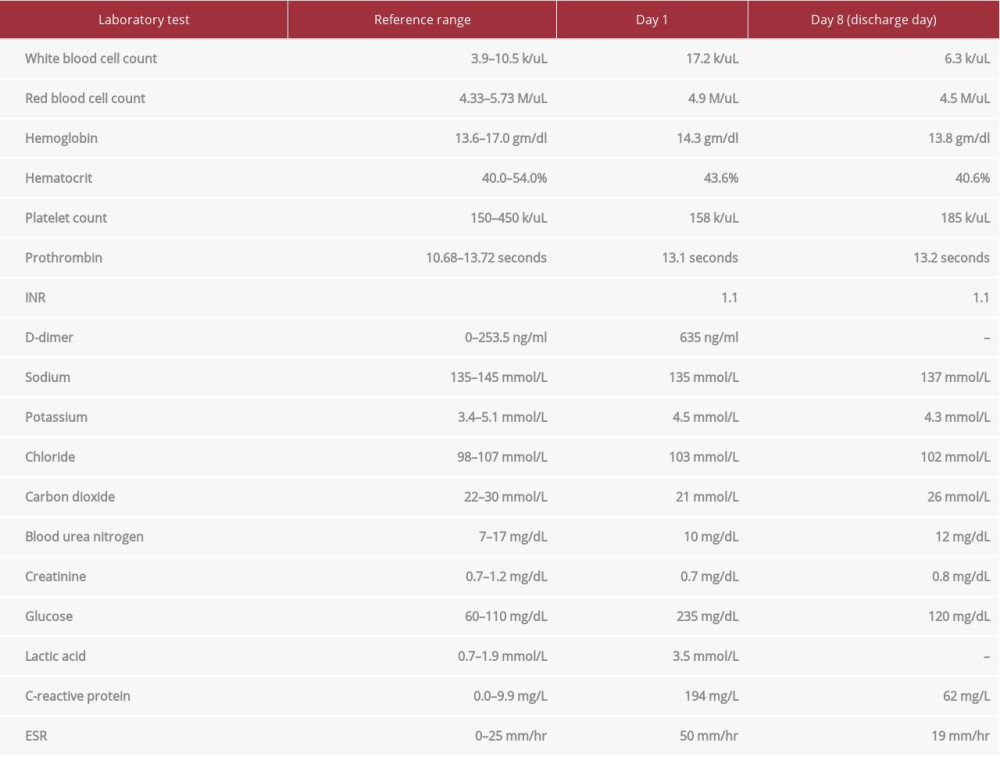 Table 1.. Laboratory data.
Table 1.. Laboratory data.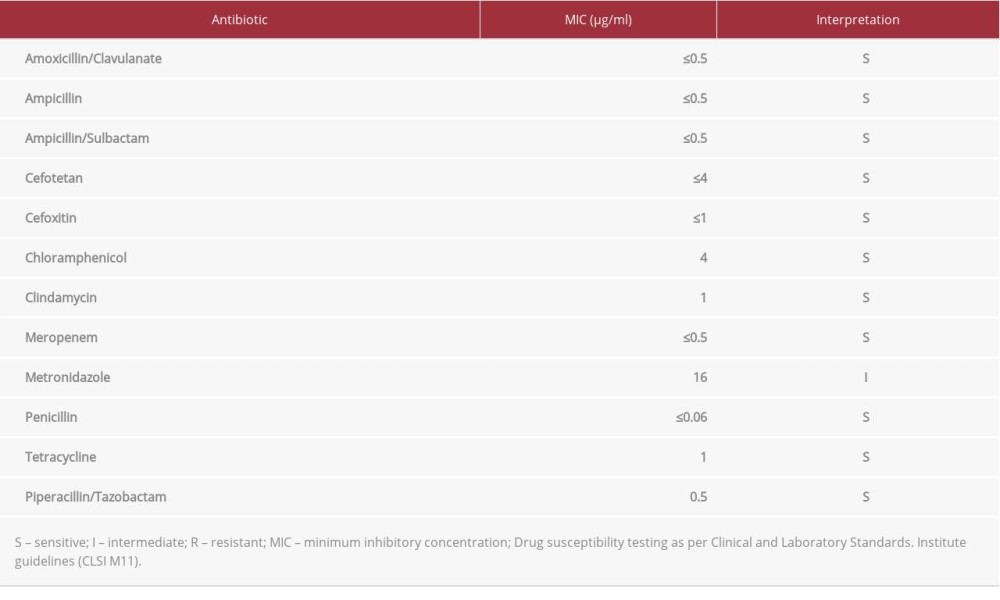 Table 2.. Antimicrobial susceptibilities of C. perfringens.
Table 2.. Antimicrobial susceptibilities of C. perfringens.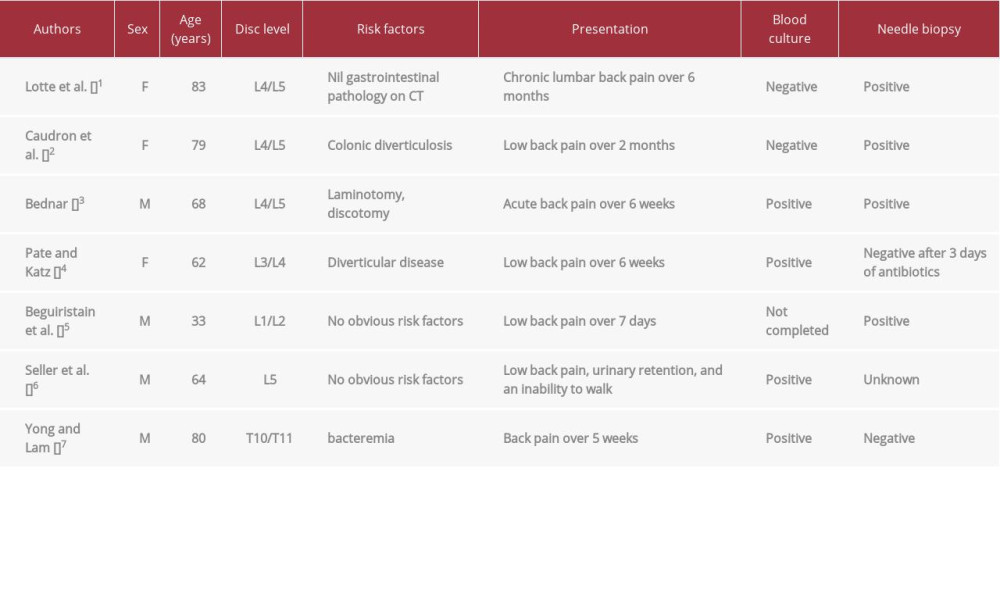 Table 3.. Main features of published Clostridium perfringens discitis cases.Table 1.. Laboratory data.Table 2.. Antimicrobial susceptibilities of C. perfringens.Table 3.. Main features of published Clostridium perfringens discitis cases.
Table 3.. Main features of published Clostridium perfringens discitis cases.Table 1.. Laboratory data.Table 2.. Antimicrobial susceptibilities of C. perfringens.Table 3.. Main features of published Clostridium perfringens discitis cases. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133