10 February 2021: Articles 
A 62-Year-Old Man with Acute Alcohol Withdrawal and Stress-Induced Cardiomyopathy
Unusual clinical course
Olubunmi O. Oladunjoye1ABCDEF*, Oreoluwa Oladiran2ABCDEF, Adeolu O. Oladunjoye3ABCDEF, Rajesh Reddy2ABCDEFDOI: 10.12659/AJCR.928518
Am J Case Rep 2021; 22:e928518






Abstract
BACKGROUND: Stress-induced cardiomyopathy is also known as takotsubo cardiomyopathy, broken heart syndrome, and left ventricular apical ballooning syndrome. Patients may present with chest pain and electrocardiogram (EKG) changes, but without coronary artery occlusion, and a reduced ejection fraction that may undergo spontaneous reversal if the patient receives appropriate hemodynamic support. This is a case report of stress-induced cardiomyopathy associated with alcohol withdrawal in a 62-year-old man.
CASE REPORT: We present the case of 62-year-old man who came to the emergency room on account of nausea and vomiting after a reduction in the daily intake of alcohol. He had no chest pain or shortness of breath but had new T wave inversions in anterolateral leads on EKG, elevated troponin, and apical wall hypokinesis with ejection fraction 40% on echocardiography. He subsequently developed active symptoms of alcohol withdrawal and was managed with intravenous Lorazepam and chlordiazepoxide. With the improvement in his mental state over the next couple of days, he had a coronary angiogram which showed no coronary disease. He was diagnosed with stress-induced cardiomyopathy or takotsubo cardiomyopathy due to alcohol withdrawal.
CONCLUSIONS: This report describes a case of takotsubo cardiomyopathy, or stress-induced cardiomyopathy, that was believed to be associated with acute alcohol withdrawal, with spontaneous improvement in the reduced left ventricular ejection fraction following medical support.
Keywords: Alcohol Withdrawal Delirium, Cardiomyopathies, Ventricular Dysfunction, Echocardiography, Stroke Volume, takotsubo cardiomyopathy, Ventricular Function, Left
Background
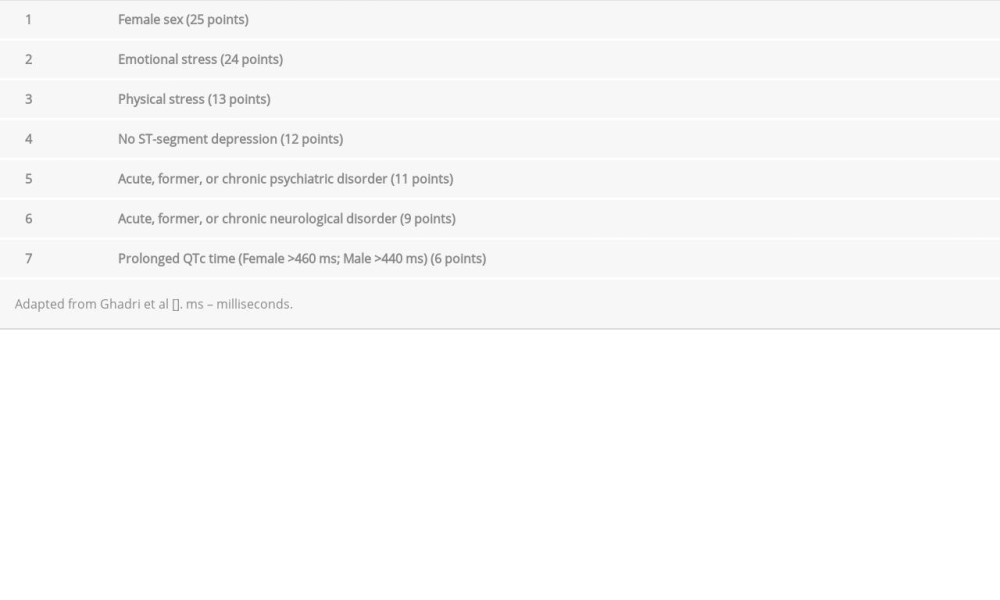
Stress-induced cardiomyopathy is also known as takotsubo cardiomyopathy (TC), “broken heart syndrome”, and left ventricular (LV) apical ballooning syndrome. Patients may present with chest pain that can mimic acute coronary syndrome (ACS), as well as electrocardiogram (EKG) changes that are similar to acute myocarditis, but with normal coronary arteries on cardiac catheterization, and a ‘signature’ sign on the echocardiogram. Diagnostic features include elevated troponin and creatinine kinase. Ghadri also reported that some EKG finding where specific to TC compared ACS. In 2017, a clinical score (InterTAK diagnostic score) was developed to differentiate TC from acute coronary syndrome (Table 1). It comprises 7 variables, including sex, presence of emotional or physical trigger, EKG finding, and presence of psychiatric or neurologic disorders. Patients with score ≥50 are more likely to have TC [1,2]. Takotsubo cardiomyopathy is associated with a reduced ejection fraction (EF) that may undergo spontaneous reversal if the patient receives appropriate hemodynamic support [3–7]. However, a study done by Jurisic et al showed that patients with TC who do not have early LV recovery have different clinical characteristics and these patients have a less favorable outcome at 1 year compared to those with early recovery. Male sex, reduced LV ejection fraction, and acute neurologic events are factors associated with late recovery [8].
It is known to be precipitated by emotional or physical stress leading to akinesis or dysfunction in apical and ventricular myocardium without coronary artery disease. The International Takotsubo Registry results showed that only 71.5% of patients had triggers that preceded TC [2]. Many other clinical conditions such as recent surgery, stroke, pheochromocytoma, acute exacerbation of asthma or chronic obstructive pulmonary disease (COPD), and acute pulmonary embolism have been reported as triggers of stress-induced cardiomyopathy [9]. It is reversible and more common in postmenopausal women. The pathophysiology is complex and not well understood. However, there is increasing evidence that excess catecholamines may be responsible for TC [10].
Alcohol withdrawal syndrome can result from intentional or unintentional sudden alcohol cassation or a marked reduction in alcohol consumption [11, 12]. Acute alcohol withdrawal has been shown to have some relationship with excess catecholamines, which may potentially have a cardiomyotoxic effect [13]. In a few cases, TC is reported to be associated with alcohol withdrawal [13–16]. This is a case report of Takotsubo cardiomyopathy, or stress-induced cardiomyopathy, associated with alcohol withdrawal in a 62-year-old man.
Case Report
A 62-year-old man with history of alcoholism and medical history of hypertension, hyperlipidemia, and Mallory-Weiss tear status after repair presented to the emergency room with nausea and several episodes non-projectile vomiting without hematemesis. He denied having abdominal pain, diarrhea, or constipation. He had no prior history of chest pain, palpitations, shortness of breath or lower-extremity swelling, and there was no family history of myocardial infarction. He reported that he not experienced any recent significant physical or emotional stressful events. He denied having any psychiatric or neurologic disorders.
He reported taking about 4–5 drinks of alcohol per day and his last alcohol use was a drink 2 days before presentation. He denied the use of tobacco other recreational substances.
On arrival in the emergency room, his vital signs showed a temperature of 37.7°C, pulse rate 86/minute but increased to 120/min within 30 minutes, blood pressure 117/74 mmHg, respiratory rate of 16/minute, and oxygen saturation of 100% on room air. He was alert and oriented to time, place, and person. His abdominal examination revealed a soft, non-tender abdomen, no palpable organomegaly, and normoactive bowel sounds. A cardiovascular exam showed no jugular venous distension, and heart sounds were S1 and S2 without murmurs. Breath sounds were normal without added sounds, but he was noticed to have significant tremors on examination. There was no appreciable lower-extremity edema.
Laboratory investigations showed a normal basic metabolic panel except for mild hypokalemia (potassium 3.4 mEq/L). A hepatic panel revealed aspartate transaminase 156 IU/L, alanine transaminase 97 IU/L, and total bilirubin 1.5 mg/dl. Hemoglobin was 13.1 g/dl with normal white blood cell count. A chest X-ray showed no pulmonary vascular congestion or pleural effusion.
An EKG showed sinus tachycardia, left axis deviation, and new T wave inversions in anterolateral leads without ST elevation or depression (Figure 1). Troponin I was elevated and peaked at 1.18 ng/ml. Brain natriuretic peptide (BNP) of 1294 pg/ml. An urgent transthoracic echocardiogram showed EF 40% and mid- to apical anterolateral, mid-apically anteroseptal, midto apical anterior, and apical marked hypokinesis with no obvious thrombus (Figure 2, Video 1). He received aspirin 324 mg. He was started on a heparin drip and guideline-directed therapy including B-blocker and angiotensin-converting enzyme inhibitor was initiated. Statin therapy was deferred due to abnormal liver enzymes.
His left heart catheterization was delayed as the patient went into active alcohol withdrawal with delirium tremens (he had confusion, visual hallucinations, increasing tremors, agitation, and signs of autonomic hyperactivity including increased heart rate, and sweat paroxysms despite normal temperatures) on the night of admission with Clinical Institute Withdrawal Assessment of Alcohol Scale score that peaked at 16, necessitating treatment with intravenous Lorazepam and chlordiazepoxide. With the improvement in his mental status over the next couple of days, he had a cardiac catheterization which revealed widely patent left main, left anterior descending, circumflex, and right coronary arteries (Figure 3).
He was later discharged on guideline-directed medical therapy for LV EF ≤40% with rehabilitation for alcohol cessation. A follow-up in the clinic weeks later showed normalization of LV function with EF of 62% and normal wall motion. At follow-up, he had also given up drinking and was taking his medications as recommended.
Discussion
We highlight a case of alcohol withdrawal-related stress-induced cardiomyopathy. Our patient did not have any cardiac symptoms such as chest pain or signs of heart failure, but he was found to have elevated troponin and BNP along with EKG findings of sinus tachycardia with T wave inversion. This prompted further evaluation with echocardiography, which showed EF 40% mid- to apical anterolateral, mid-apically anteroseptal, mid- to apical anterior, and apical marked hypokinesis. Obstructive coronary artery disease was ruled out with widely patent coronary arteries on left heart catheterization.
TC is one of the differentials for elevated cardiac biomarkers. It is precipitated by emotional or physical stress leading to akinesis or dysfunction in apical and mid-ventricle in the absence of obstructive coronary artery disease and it is common in post-menopausal women. However, some other conditions have also been reported to trigger TC, including stroke, acute asthma or COPD exacerbation, severe sepsis, recent surgery, and critical illnesses. The pathophysiology is not clearly understood but there is increasing evidence that excess catecholamine may be responsible for this condition. It has been reported that severe emotional or physical stress can lead to overstimulation of the hypothalamus-pituitary-adrenal axis, thereby leading to release of excess catecholamines [9].
Alcohol withdrawal has been associated with excess catecholamines releases from increased adrenergic activity, which can have a cardiomyotoxic effect [13] and there is increasing evidence that excess catecholamines can be responsible for TC [10]. Agu et al in their case report suspected that TC in patients with delirium tremens, which is a severe form of alcohol withdrawal syndrome, is possibly secondary to the cardiomyotoxic effect of catecholamines or CNS-medicated coronary spasm [17].
The clinical profile for TC usually includes postmenopausal female and mimics acute coronary syndrome with symptoms of chest pain, exertional dyspnea, palpitation, or syncope, and many patients report experiencing a severe emotional or physical event [3,9,13,18]. However, our case was a middle-aged man with no reports of chest pain or exertional dyspnea, with no significant stressful event in his life. He reported a history of chronic alcohol use but with a reduction in his alcohol intake 2 days prior to presentation, which likely resulted in alcohol withdrawal symptoms. His symptoms of nausea and vomiting were similar to the presentation of a reported case of 45-year-old woman with TC in the setting of acute alcohol withdrawal [13].
Our patient had EKG findings of sinus tachycardia and T wave inversion with normal QTc interval. Similar findings of T wave inversion were reported in other cases of TC secondary to alcohol withdrawal [13–16]. However, EKG abnormalities may or may not be present in TC. Abnormal EKG findings can be ST elevation or depressions, T wave inversion, or prolonged QTc interval. These findings can also be seen in myocardial infarction. Therefore, an EKG cannot reliably diagnose TC. However, Ghadri et al identified EKG changes specific to TC using the International Takotsubo Registry. Patients with TC were more likely to have ST elevation in aVR with T-inversion in any other lead compared with ST depression in leads V2 and V3 in those with non-ST elevation myocardial infarction [2]. Our patient had T wave inversion but no ST elevation in aVR. Cardiac markers, including troponin and BNP, can also be elevated, as seen in our patient (Troponin I 1.18 ng/ml. BNP 1294 pg/ml) [9,13]. Echocardiogram in TC usually reveals reduced LV EF with regional wall motion abnormalities in the apical and mid-ventricular myocardium. All these findings can also be seen in obstructive coronary disease, making it difficult to differentiate from ACS [19]. Therefore, cardiac catheterization to exclude obstructive lesion is indicated to make a final diagnosis of TC as stated in the Modified Mayo Clinic criteria for the diagnosis of TC or the European Heart failure Association Diagnostic criteria [18,20]. However, in 2017, Ghadri et al developed a clinical score (InterTAK diagnostic score) to differentiate TC from ACS. It comprises 7 non-invasive clinical variables, including sex, presence of emotional or physical trigger, EKG finding, and presence of psychiatric or neurologic disorders. Patients with scores ≥50 are more likely to have TC (sensitivity 94.7%) [1]. Using this score, our patient would have had a score of 12/100 with low probability for TC (Table 1) and would have been incorrectly diagnosed as having ACS.
Management of patients with TC is mostly supportive. Reduced EF may undergo spontaneous reversal if the patient receives appropriate hemodynamic support [3–7]. The underlying conditions that triggered TC should be treated. Some preclinical studies have shown that metoprolol or carvedilol can be beneficial and could be used if there are no contraindications [21,22]. Our patient was discharged on guideline-directed medical therapy for LV EF ≤40% with rehabilitation for alcohol cessation. Patients with TC should be followed up with repeat imaging to ensure recovery from the cardiomyopathy [18]. A study done by Jurisic et al showed that patients with TC who do not have early LV recovery have different clinical characteristics and these patients have a less favorable outcome at 1 year compared with those with early recovery. Male sex, reduced LV ejection fraction, and acute neurologic events were factors associated with late recovery [8]. Although our patient was male with reduced EF (40%), he had an early LV recovery as evident by normalization of LV function with EF of 62% and normal wall motion on follow-up echocardiogram.
Conclusions
This report described a case of takotsubo cardiomyopathy, or stress-induced cardiomyopathy, that was believed to be associated with acute alcohol withdrawal, with spontaneous improvement in the reduced left ventricular ejection fraction following medical support.
Figures
References:
1.. Ghadri JR, Cammann VL, Jurisic S, A novel clinical score (InterTAK Diagnostic Score) to differentiate takotsubo syndrome from acute coronary syndrome. Results from the International Takotsubo Registry: Eur J Heart Fail, 2017; 19(8); 1036-42
2.. Ghadri J-R, Cammann VL, Templin C, The International Takotsubo Registry. Rationale, design, objectives, and first results: Heart Fail Clin, 2016; 12(4); 597-603
3.. Templin C, Ghadri JR, Diekmann J, Clinical features and outcomes of takotsubo (stress) cardiomyopathy: N Engl J Med, 2015; 373(10); 929-38
4.. Brenner ZR, Powers J, Takotsubo cardiomyopathy: Heart Lung, 2008; 37(1); 1-7
5.. Nykamp D, Titak JA, Takotsubo cardiomyopathy, or broken-heart syndrome: Ann Pharmacother, 2010; 44(3); 590-93
6.. Watanabe M, Izumo M, Akashi YJ, Novel understanding of takotsubo syndrome: Int Heart J, 2018; 59(2); 250-55
7.. Pelliccia F, Kaski JC, Crea F, Camici PG, Pathophysiology of takotsubo syndrome: Circulation, 2017; 135(24); 2426-41
8.. Jurisic S, Gili S, Cammann VL, Clinical predictors and prognostic impact of recovery of wall motion abnormalities in takotsubo syndrome. Results from the International Takotsubo Registry: J Am Heart Assoc, 2019; 8(21); e011194
9.. Gupta S, Gupta MM, Takotsubo syndrome: Indian Heart J, 2018; 70(1); 165-74
10.. , Role of psychotropic medications in the treatment of adults with “broken heart” syndrome: Cureus, 2019; 11(7); e5177
11.. Jesse S, Bråthen G, Ferrara M, Alcohol withdrawal syndrome. Mechanisms, manifestations, and management: Acta Neurol Scand, 2017; 135(1); 4-16
12.. Perry EC, Inpatient management of acute alcohol withdrawal syndrome: CNS Drugs, 2014; 28(5); 401-10
13.. Stout BJ, Hoshide R, Vincent DS, Takotsubo cardiomyopathy in the setting of acute alcohol withdrawal: Hawaii J Med Public Health, 2012; 71(7); 193-94
14.. Mitchell SA, Crone RA, Takotsubo cardiomyopathy: A case report: J Am Soc Echocardiogr, 2006; 19(9); 1190.e9-10
15.. Thompson AG, Hung J, Takotsubo cardiomyopathy associated with alcohol withdrawal: Med J Aust, 2011; 194(7); 373-74
16.. Suzuki K, Osada N, Akasi YJ, An atypical case of “takotsubo cardiomyopathy” during alcohol withdrawal: Abnormality in the transient left ventricular wall motion and a remarkable elevation in the ST segment: Intern Med, 2004; 43(4); 300-5
17.. Agu CC, Bakhit A, Basunia M, Takotsubo cardiomyopathy precipitated by delirium tremens: J Community Hosp Intern Med Perspect, 2015; 5(6); 29704
18.. Lyon AR, Bossone E, Schneider B, Current state of knowledge on takotsubo syndrome: A position statement from the Taskforce on Takotsubo Syndrome of the Heart Failure Association of the European Society of Cardiology: Eur J Heart Fail, 2016; 18(1); 8-27
19.. Akashi YJ, Nef HM, Lyon AR, Epidemiology and pathophysiology of takotsubo syndrome: Nat Rev Cardiol, 2015; 12(7); 387-97
20.. Prasad A, Lerman A, Rihal CS, Apical ballooning syndrome (tako-tsubo or stress cardiomyopathy):A mimic of acute myocardial infarction: Am Heart J, 2008; 155(3); 408-17
21.. Izumi Y, Okatani H, Shiota M, Effects of metoprolol on epinephrine-induced takotsubo-like left ventricular dysfunction in non-human primates: Hypertens Res, 2009; 32(5); 339-46
22.. Paur H, Wright PT, Sikkel MB, High levels of circulating epinephrine trigger apical cardiodepression in a β2-adrenergic receptor/Gi-dependent manner. A new model of takotsubo cardiomyopathy: Circulation, 2012; 126(6); 697-706
Figures
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133