15 January 2021: Articles 
The Role of Anticoagulation in Post-COVID-19 Concomitant Stroke, Myocardial Infarction, and Left Ventricular Thrombus: A Case Report
Unusual clinical course, Challenging differential diagnosis, Management of emergency care, Educational Purpose (only if useful for a systematic review or synthesis), Rare coexistence of disease or pathology
Phool Iqbal1ABCDF*, Bushra Laswi1DEF, Muhammad Bilal Jamshaid1EF, Aamir Shahzad1EF, Hammad Shabir Chaudhry1EF, Dawlat Khan1EF, Muhammad Sohaib Qamar2F, Zohaib Yousaf1EFDOI: 10.12659/AJCR.928852
Am J Case Rep 2021; 22:e928852






Abstract
BACKGROUND: Coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) primarily affects the lungs but can involve any organ. The medical community is struggling to cope with the critical illness associated with the disease. On top of that, patients who have recovered from COVID-19 have presented with complications such as thrombotic episodes in various organs both during and after being infected with SARS-CoV-2. A COVID-19-associated prothrombotic state has been mentioned in multiple recent research articles. The role of anticoagulants is debatable, because even after receiving them prophylactically, many patients have experienced thrombotic episodes. The situation, therefore, represents a challenge to the medical community.
CASE REPORT: We report on a COVID-19-associated prothrombotic state in a 65-year-old man with no history of comorbid illness. Initially, he presented with right-sided weakness and was found to have had an acute ischemic stroke. Urgent imaging after the stroke revealed changes on electrocardiography that were remarkable for left bundle branch block. The patient’s elevated cardiac enzyme levels correlated with a silent acute myocardial infarction (MI). His echocardiogram revealed a left ventricular (LV) thrombus. He was managed with a multidisciplinary approach involving Neurology, Cardiology, and Medicine.
CONCLUSIONS: COVID-19-associated prothrombotic episodes involving arterial and venous systems have been reported in the literature. But concomitant stroke, acute MI, and LV thrombus rarely have been documented. The role of prophylactic or therapeutic anticoagulation is still unclear because even when patients are on these drugs, they continue to develop thrombotic episodes. Indeed, further studies are required to develop a standard management plan for what can be a fatal situation.
Keywords: COVID-19, Stroke, Thrombosis, Bundle-Branch Block, COVID-19, Echocardiography, Heart Ventricles, ischemic stroke, Tomography, X-Ray Computed
Background
Since the start of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic in Wuhan, China in December 2019 as a cluster of unknown pneumonia cases, the infection has become widespread and a pandemic was declared on March 11, 2020 [1]. Currently, the world is striving to gain an understanding of the disease’s pathophysiology so as to achieve an optimal solution. SARS-CoV-2 primarily affects the pulmonary system. However, because of various mechanisms of underlying dysregulated immunity and systemic inflammation, some of which are not well understood, the virus tends to cause extrapulmonary complications, such as stroke, thromboembolic episodes, heart failure, acute kidney injury, and liver injury. [1]. The diagnosis is based on real-time reverse transcription polymerase chain reaction using GeneXpert technology [2]. We report a case of post-COVID-19-associated thrombotic complications in a previously healthy man. He presented with right-sided weakness and was later found to have experienced an acute ischemic stroke. Further investigation revealed an acute myocardial infarction (MI) and left ventricular (LV) thrombus.
Case Report
A healthy 65-year-old man with no previously diagnosed comorbidities or history of smoking, who was not an alcoholic, presented to the Emergency Department within 2 h of onset of right-sided weakness. There was no preceding trauma nor had the patient lost consciousness. On physical examination, he was conscious and oriented to time, place, and person. His initial vital signs revealed a blood pressure of 148/99 mmHg with mild tachypnea and tachycardia of 26/min and 102/min, respectively. His oxygen saturation was normal while breathing room air. The patient’s neurological examination was remarkable for global aphasia, left gaze deviation, right-sided hemiparesis with a decrease in power of 3/5 in both upper and lower limbs, and right hemispatial neglect. Chest auscultation revealed coarse crepitation bilaterally that was mild, diffuse, and scattered. The patient’s cardiovascular examination was unremarkable.
An immediate computed tomography (CT) perfusion scan of the head showed a matched perfusion defect in the left fronto-parieto-temporal region that gave the impression of an infarct with occlusion of the left middle cerebral artery (Figure 1). Because the patient had presented within 2 h of symptom onset, he was eligible for stroke thrombolysis. As per stroke protocol, 5 mg of intravenous alteplase, a tissue plasminogen activator (tPA), was administered, but it was discontinued after 8 minutes because of moderate bleeding from the patient’s oral mucosa.
Review of some of the upper chest images from the patient’s neck CT scan revealed incidental bilateral peripheral pulmonary consolidations. A chest X-ray was performed, which showed bilateral patchy infiltrates and scattered reticulations (Figure 2). An electrocardiogram showed a left bundle branch block with sinus tachycardia and elevated troponin-T levels suggestive of MI (Figure 3). An echocardiogram was remarkable for compromised left LV function and LV thrombus with severely reduced systolic LV function (26% ejection fraction [EF]) and mild mitral valve regurgitation (Figure 4).
Given the chest X-ray findings, the patient was isolated and tested for COVID-19 infection. Two COVID-19 reverse transcription polymerase chain reaction (PCR) tests returned negative results. A CT scan of the patient’s chest showed bilateral consolidations with diffuse ground-glass opacities (Figure 5).
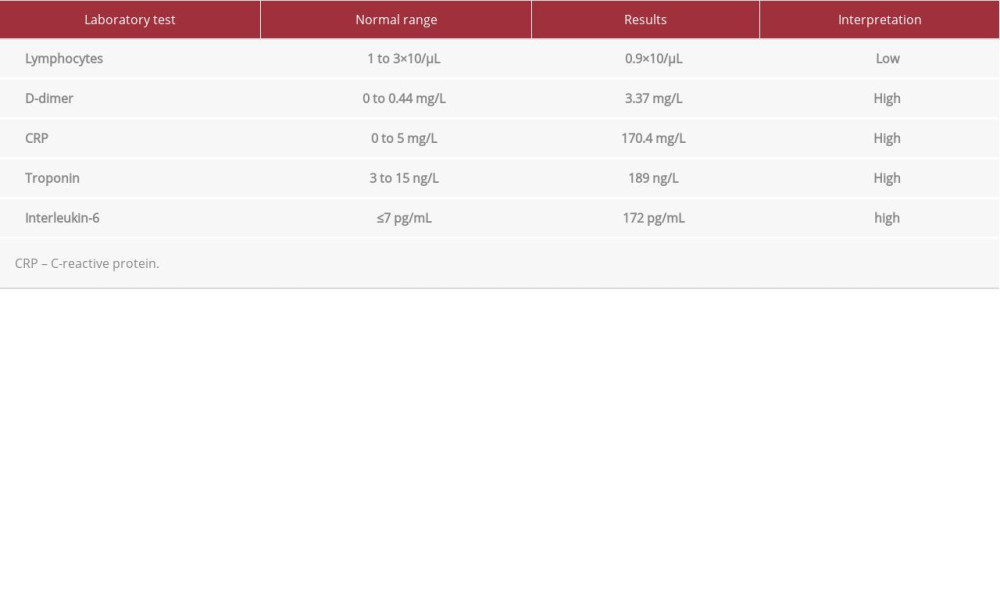
Further bloodwork showed high levels of C-reactive protein (CRP) and ferritin, elevated levels of interleukins (ILs) and D-dimer, and lymphopenia (Table 1). A multidisciplinary team, including representatives from Neurology, Cardiology, and Internal Medicine, was involved in managing the patient for an acute stroke, MI, and LV thrombus. He was started on aspirin 100 mg, clopidogrel 75 mg, and atorvastatin 40 mg.
On the second day of the patient’s admission, he became short of breath, requiring 4L/min of oxygen to maintain saturation. COVID-19 serology was immunoglobulin (Ig) M-negative and IgG-positive, which correlated with his previous infection. Workup for sepsis, including testing for
The patient’s condition gradually improved and he continued physical and occupational therapy in the hospital. A repeat transthoracic echocardiogram done on an inpatient basis 1 month after admission showed resolution of the thrombus but the persistence of the reduced EF (22%). The patient did not deteriorate further during his hospital stay and began to maintain normal oxygen saturation. However, because he was critically ill with myopathy, he is receiving physiotherapy and rehabilitation therapy. He also is being rigorously followed by a consultant cardiologist, and once his condition has been stabilized with the rehabilitation therapy, he is scheduled to undergo coronary angiography on an outpatient basis.
Discussion
Various underlying pathophysiological mechanisms are associated with COVID-19. The SARS-CoV-2 virus manifests as systemic inflammation and immune cell overactivation with the release of cytokines and IL production [3]. Recent evidence also supports an association between COVID-19 and thrombotic events, and the literature has documented cases of both arterial and venous thrombotic events [4]. Thrombotic complications, such as pulmonary embolism, acute aortic thrombosis, cerebral vein thrombosis, coronary artery thrombosis, stroke, and acute superior mesenteric artery thrombosis, are associated with severe COVID-19 illness [5–9]. Although the exact mechanism of a COVID-19 hypercoagulable state remains unclear, Haimei proposed that the increased risk of thrombosis in patients with COVID-19 is related to SARS- CoV-2-mediated enhanced angiotensin-converting enzyme 2 (ACE2) activation, which is an essential component of the renin-angiotensin system expressed by vascular endothelial cells. ACE2 converts angiotensin (Ang) 2 into Ang-(1–7) and Ang 1 into Ang-(1–9), respectively [10]. Ang-(1–9) causes an imbalance between the plasma concentration of tPA and plasminogen activator inhibitor-1 (PAI-1), resulting in an increased risk of thrombosis [10]. Another suggested mechanism involves elevation of D-dimer levels and presence of antiphospholipid antibodies, which are frequently reported in patients with COVID-19 who have vascular thrombotic complications and can lead to thrombotic events [11].
Our patient initially presented with stroke. Further investigation revealed acute MI and an LV thrombus was seen on echo-cardiography, which might have been the cause of his stroke. The reason for the LV thrombus could be related to a low EF after a silent MI. On the other hand, the possible rationale for silent MI can be attributed to SARS- CoV-2-related coronary artery thrombosis; however, it can only be confirmed after coronary angiography. The cardiologist suggested that our patient not undergo that test because of his history of acute stroke. The patient does not have any of the traditional risk factors for development of thrombosis, such as a hypercoagulable state, nor previously known thrombophilia or a family history of thrombosis. Hence, because he had positive IgG antibodies against the SARS-CoV-2 virus, the likely explanation is a post-COVID-19-associated prothrombotic state that led to a MI, stroke, and LV thrombus.
There may be several approaches to management of hyper-coagulability associated with COVID-19. In a narrative review, Carfora et al. suggested using anti-inflammatory drugs (corticosteroids and human monoclonal antibodies) or statins and ACE-I, which reduce endothelial dysfunction in keeping with their proposed mechanisms of action. LMWH usually also is used to prevent thrombosis [12]. In an observational cross-sectional prospective study by Ionescu et al., therapeutic anticoagulation was found to have better efficacy in preventing thrombotic episodes in severe COVID-19, leading to a decrease in mortality [13]. Similarly, Nadkarni and Lala, in a retrospective observational study of 4389 elderly individuals confirmed to be COVID-19-positive, evaluated the role of anticoagulation in decreasing mortality and intubation in hospitalized patients [14]. In a multicenter, prospective cohort study, Helms et al. reported an increased risk of thrombosis associated with severe COVID-19 disease despite the fact that the patients were kept on prophylactic or therapeutic anticoagulation [15]. Overall, the results of research in this area show a lower risk of thrombosis in patients receiving preventive and therapeutic doses of anticoagulants. However, optimal types and regimens are yet to be explored.
Conclusions
Published reports indicate that some patients with COVID-19 infection have received anticoagulants as prophylaxis and also for therapy, with beneficial results in terms of reduction in associated thrombotic episodes. Currently, there are no guidelines or recommendations for prevention of COVID-19-associated thrombosis, raising a critical concern about the need for further studies of ways to avoid this life-threatening situation.
Figures
References:
1.. Zaim S, Chong JH, Sankaranarayanan V, COVID-19 and multiorgan response: Curr Probl Cardiol, 2020; 45(8); 100618
2.. Axell-House DB, Lavingia R, Rafferty M, The estimation of diagnostic accuracy of tests for COVID-19: A scoping review: J Infect, 2020; 81(5); 681-97
3.. Guzik TJ, Mohiddin SA, Dimarco A, COVID-19 and the cardiovascular system: Implications for risk assessment, diagnosis, and treatment options: Cardiovasc Res, 2020; 116(10); 1666-87
4.. McFadyen JD, Stevens H, Karlheinz P, The emerging threat of (micro)thrombosis in COVID-19 and its therapeutic implications: Circ Res, 2020; 127(4); 571-87
5.. Le Berre A, Marteau V, Emmerich J, Concomitant acute aortic thrombosis and pulmonary embolism complicating COVID-19 pneumonia: Diagn Interv Imaging, 2020; 101(5); 321-22
6.. Oxley TJ, Mocco J, Majidi S, Large-vessel stroke as a presenting feature of COVID-19 in the young: N Engl J Med, 2020; 382(20); e60
7.. Cavalcanti DD, Raz E, Shapiro M, Cerebral venous thrombosis associated with COVID-19: Am J Neuroradiol, 2020; 41(8); 1370-76
8.. Shams A, Ata F, Mushtaq K, Coronary thrombosis in a young male with COVID-19: IDCases, 2020; 21; e00923
9.. Cheung S, Quiwa JC, Pillai A, Superior mesenteric artery thrombosis and acute intestinal ischemia as a consequence of COVID-19 infection: Am J Case Rep, 2020; 21; e925753-1-3
10.. Haimei M, Pathogenesis and treatment strategies of COVID-19-related hypercoagulant and thrombotic complications: Clin Appl Thromb, 2020; 26; 1076029620944497
11.. Zhang Y, Xiao M, Zhang S, Coagulopathy and antiphospholipid antibodies in patients with COVID-19: N Engl J Med, 2020; 382(17); e38
12.. Carfora V, Spiniello G, Ricciolino R, Anticoagulant treatment in COVID-19: A narrative review: J Thromb Thrombolysis, 2020 [Online ahead of print]
13.. Ionescu F, Grasso-Knight G, Castillo E, Therapeutic anticoagulation delays death in COVID-19 patients: Cross-sectional analysis of a prospective cohort: TH Open, 2020; 4(3); e263-70
14.. Nadkarni GN, Lala A, Bagiella E, A single health system study: J Am Coll Cardiol, 2020; 76(16); 1815-26
15.. Helms J, Tacquard C, Severac F, High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study: Intensive Care Med, 2020; 46(6); 1089-98
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133