26 March 2021: Articles 
Metastatic Infiltration of Anaplastic Carcinoma of the Pancreas Into the Portal Venous System: A Masquerading Cause of Expansive Portal Venous Thrombosis
Challenging differential diagnosis
Yuka Hirakawa1AEF*, Masaki Tago1AEF, Naoko E. Katsuki1AEF, Seijiro Makio1AE, Shu-ichi Yamashita1AEDOI: 10.12659/AJCR.929678
Am J Case Rep 2021; 22:e929678






Abstract
BACKGROUND: The portal vein thrombosis caused by a carcinoma of the pancreas or liver could be a diagnostic challenge. There are some cases which could be diagnosed only by observing changes in patients’ clinical manifestations or imaging studies over time.
CASE REPORT: A 63-year-old man experienced exacerbation of chronic low back pain for 1 month, with abdominal distention. He was admitted to our hospital because abdominal ultrasonography and abdominal contrast-enhanced computed tomography performed at another hospital revealed an extensive thrombus in the portal, splenic, and superior mesenteric veins. Anticoagulation therapy with warfarin was started immediately on admission. Although no baseline disease, such as malignancies, coagulopathies, infections, or collagen diseases were revealed during the 12 days of his hospitalization, the thrombus gradually expanded, with the appearance of obstructive jaundice 8 months after admission. He was readmitted at that time for biopsy of intrahepatic tumors detected by abdominal computed tomography, which diagnosed metastasis of a carcinoma of unknown origin. Although chemotherapy was started, he died 11 months after his initial admission to our hospital. Autopsy revealed a tumorous lesion in the pancreatic head with almost complete replacement of the portal venous thrombus with a similar-appearing tumor. We confirmed the diagnosis of portal venous metastatic infiltration by undifferentiated pancreatic carcinoma, using histopathological examinations.
CONCLUSIONS: It is essential to consider portal venous metastatic infiltration of undiagnosed malignancy inducing local hypercoagulopathy as a possible cause of expansive portal venous thrombosis.
Keywords: Neoplasms, Unknown Primary, Pancreatic Neoplasms, Portal Vein, Thrombosis, Carcinoma, Mesenteric Veins, Pancreas, Venous Thrombosis
Background
Portal venous thrombosis is a rare condition, with a reported prevalence of 3.7 per 100 000 residents and a yearly incidence rate of 0.7, accounting for 1% of autopsy cases [1]. The causes of portal vein thrombosis are diverse and are divided into 2 types: local and patho-anatomical factors of the liver, such as cirrhosis, malignant tumor infiltration of the portal vein, or intra-abdominal inflammatory diseases, and systemic factors, such as genetic or acquired hematological diseases causing systemic coagulopathy, or collagen diseases or malignancy-induced systemic coagulopathy [2,3]. Investigating the cause of portal venous thrombosis consists of various imaging tests, namely abdominal ultrasonography; computed tomography (CT), especially with contrast enhancement; and magnetic resonance imaging (MRI), which also might be useful to detect the presence of portal venous thrombosis; as well as hematological studies, namely coagulation testing, or bacteriological studies, such as blood culture [2,3]. However, even with these diagnostics, some cases caused by a carcinoma of the pancreas or liver could be a diagnostic challenge [4,5], and were diagnosed in some studies only by observing changes in patients’ clinical manifestations or imaging studies over time.
We report an autopsy case of expansive venous thrombosis in the portal, splenic, and superior mesenteric veins, which was a diagnostic challenge because the patient’s condition was intractable to treatment. The final diagnosis was made postmortem as venous thrombosis caused by local hypercoagulopathy induced by portal infiltration of metastatic carcinoma of the pancreas.
Case Report
A 63-year-old man visited another hospital and presented with low back pain and abdominal distension. His chronic dull lower back pain had gradually worsened for the previous 1 month before his visit. In addition, he complained of anorexia and abdominal distention lasting for 1 week. His family history showed that his father had gastric carcinoma, and his mother had pancreatic carcinoma. He had consumed 15 g of alcohol a day and smoked 40 cigarettes a day for 40 years. Because abdominal ultrasonography and abdominal contrast-enhanced CT showed an extensive thrombus in the portal, splenic, and superior mesenteric veins, he was transferred to our hospital.
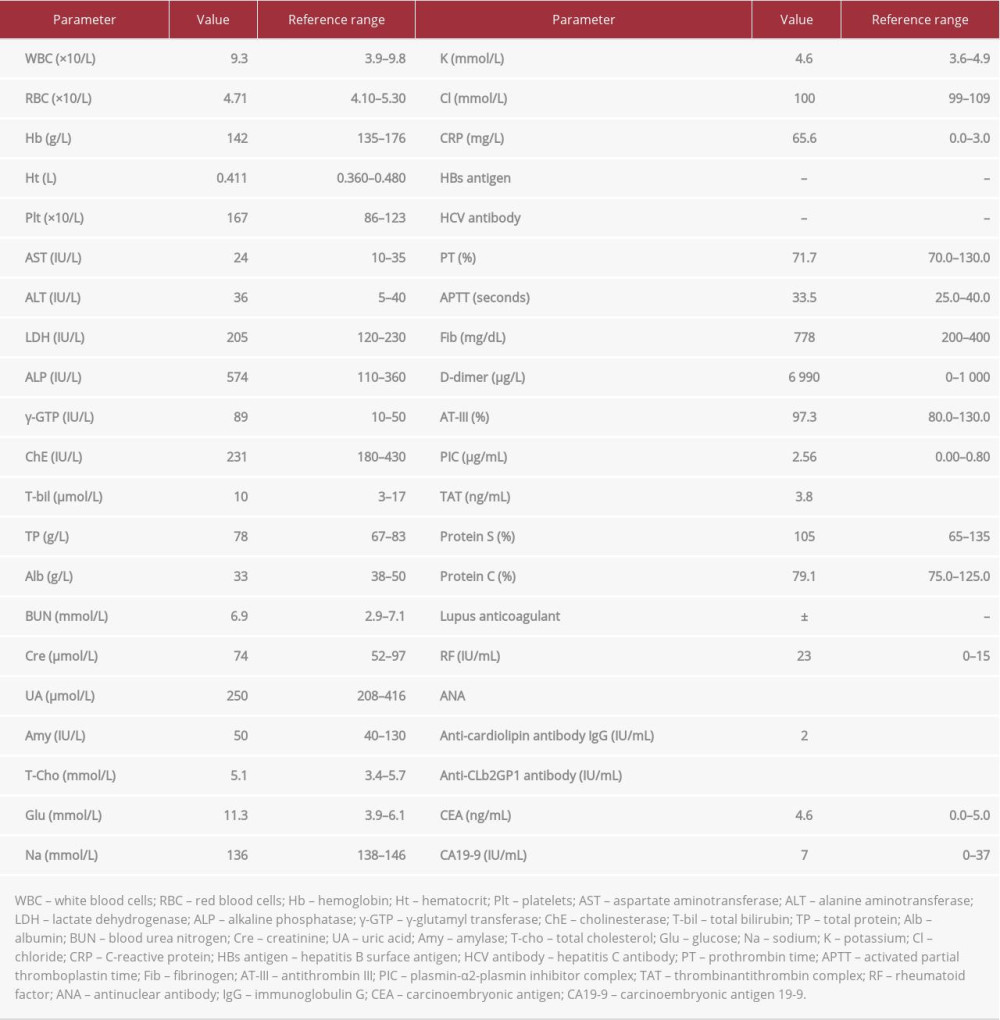
His vital signs on admission were: body temperature 36.4°C, blood pressure 169/66 mmHg, pulse rate 104 beats/min, and percutaneous oxygen saturation 97% on room air. Physical examination revealed no abnormalities in the abdomen except mild epigastric tenderness. Laboratory findings on admission are shown in Table 1, which revealed: aspartate aminotransferase (AST) 24 IU/L, alanine aminotransferase (ALT) 36 IU/L, lac-tate dehydrogenase (LDH) 205 IU/L, alkaline phosphatase (ALP) 574 IU/L, γ-glutamyl transpeptidase (γ-GTP) 89 IU/L, and C-reactive protein (CRP) 65.6 mg/L. Although prothrombin time (PT) and activated partial thromboplastin time (APTT) were normal, the D-dimer concentration was 6 990 μg/L. Rheumatoid factor was positive, antinuclear and anticardiolipin antibodies were negative, lupus anticoagulant±, and protein S and protein C concentrations were normal. Chest and abdominal contrast-enhanced CT revealed a continuous low-density area in the portal, superior mesenteric, and splenic veins without enhancement, which was compatible with the findings of thrombosis according to the CT density value (Figure 1A, 1B). The patient was considered to have chronic portal hypertension owing to the presence of collateral circulation developing in the hilar region of the liver, and splenomegaly (Figure 1A, 1B). CT revealed no tumorous lesions or inflammatory conditions in the hepatic or biliary systems causing the venous thrombosis. Esophagogastroduodenoscopy showed no abnormal findings relating to portal hypertension, such as gastroduodenal ulcers or esophageal varices.
According to the diagnosis of chronic portal venous thrombosis, continuous intravenous heparin infusion was started, maintaining the APTT above 45 s, which was subsequently changed to 3.5 mg/day of oral warfarin, maintaining the prothrombin time-international normalized ratio (PT-INR) above 2.5. Considering the chronicity of the condition, surgical or thrombolytic treatment was not selected. Without apparent conditions that could cause portal venous thrombosis, such as infections, collagen diseases, or congenital hypercoagulopathies, either systemic hypercoagulopathy owing to malignancy, or local coagulation owing to malignant invasion into the vascular endothelium was suspected. However, because even meticulous imaging studies, including whole-body contrast-enhanced CT, esophagogastroduodenoscopy, or colonoscopy failed to detect malignancy, he was discharged on the 22nd hospital day and was followed as an outpatient (0 month). Two months after discharge, magnetic resonance cholangiopancreatography (MRCP) was performed and revealed diffuse thickening of the bile duct wall in the middle to lower common bile duct, which caused stenosis. However, no space-occupying lesions were detected (Figure 2A). Subsequent esophagogastroduodenoscopy revealed the presence of esophagogastric varices. Three months after discharge, esophageal varices ruptured, for which emergency endoscopic ligation therapy was performed. At that point, CT showed exacerbation and enlargement of the venous thrombus, without detecting tumorous lesions. Positron emission tomography-CT (PET-CT) was performed in the same month, which showed only low uptake at the site of the portal venous thrombus, with low probability of malignancy (Figure 3A, 3B). Eight months after discharge, he was readmitted to our hospital owing to the appearance of overt obstructive jaundice with worsened back pain and chest pain. MRCP showed stenosis of the common bile duct and dilatation of the intrahepatic bile ducts (Figure 2B). Brush cytology of the common bile duct performed through endoscopic retrograde cholangiopancreatography (ERCP), during which we placed a stent to decrease icterus, revealed grade IV adenocarcinoma. According to these findings, we repeated abdominal contrast-enhanced CT, which showed higher enhancement of the thrombus in the right branch of the intrahepatic portal vein compared with other parts of the portal venous system, suggesting infiltration of tumor cells in the thrombus (Figure 1C), further enlargement of the portal venous thrombus (Figure 1D), a tumor-like low-density area in the liver segments 4–8 (S4–8) (Figure 1E), and dilation of the intrahepatic bile ducts (Figure 1F). Histopathological examination of the liver biopsy from the lesion in S4–8 showed that undifferentiated atypical cells infiltrating the liver tissue and portal vein (Figure 4). The patient was diagnosed with undifferentiated carcinoma of unknown origin with hepatic and portal venous invasion. Nine months after discharge, chemotherapy with carboplatin plus nab-paclitaxel was started without success, resulting in his death in the 11th month.
An autopsy was performed, which macroscopically showed a 4-cm-diameter mass lesion growing from the pancreatic head to the body with expansive spread of metastatic tumor in the portal venous system (Figure 5A, 5C). Histological examination revealed undifferentiated carcinoma cells infiltrating the portal venous system, similar to the carcinoma cells in the pancreatic mass (Figure 5B, 5D), confirming the diagnosis of pancreatic undifferentiated carcinoma with expansive metastatic infiltration of the portal venous system, with a hepatic meta-static tumor as the cause of death.
Discussion
Causes of portal venous thrombosis are diverse and may include vascular endothelial disorders, blood flow abnormalities, hypercoagulopathy, impaired fibrinolytic capacity, and abnormal platelet count or function [1–3]. In addition to these causes, 10% to 14% of portal venous thrombosis were failed to be identified [1,6]. On the other hand, 27% to 67% of the causes of the disease were reported to have been relevant to some malignancies [1,6]. Among them, primary hepatocellular carcinoma had the highest incidence followed by pancreatic carcinoma, carcinoma in the biliary system, gastric cancer, and colon cancer with relatively high incidence [1,6]. Therefore, it is essential to continue meticulous investigations of causative malignancies with careful observational follow-up while giving appropriate treatments of portal venous thrombosis itself when initial investigations fail to identify any cause of thrombosis.
The present case was an example of cases involving difficulty finding the cause of the thrombosis. Our patient presented with extensive portal vein thrombosis on his first visit, which was considered chronic owing to the presence of collateral circulation or splenomegaly, suggesting long term portal hyper-tension [2,3]. The space-occupying lesion inside the lumens of the portal, splenic, and superior mesenteric veins in this case was initially considered to be a thrombus, according to the CT density values. However, the density of the lesion in the portal vein increased 8 months later, compatible with emergence of a tumor [2,3,7]. This was finally confirmed as meta-static infiltration of pancreatic cancer, by postmortem examination. Thus, the mechanism of this thrombus formation was considered to be infiltration of malignant cells from the pancreatic cancer into the endothelium of the portal venous system, resulting in local hypercoagulopathy in the vascular lumen. This fact could explain the initial difficulties finding the actual cause of the thrombosis because it is almost impossible to detect exceedingly small tumorous lesions in gross thrombi at an early stage.
Occasionally, it can be difficult to differentiate between portal vein thrombosis and tumor metastasis with infiltration into the portal venous system, which was a problem in the present case from the onset. Ultrasonography, CT, MRI, or angiography are commonly used to clarify the differential diagnoses [2,3,7]; PET-CT has also been reported to be useful [8]. Regarding ultrasonography, color Doppler can detect the presence of arterial blood flow in the thrombus [2,3,7], which suggests tumor infiltration into the thrombus. Additionally, contrast-enhanced ultrasonography is more useful than CT because of the higher sensitivity (88%) and specificity (100%) [9]; regrettably, we did not use this modality. Contrast-enhanced CT is one of the most commonly used modalities to investigate the presence of tumorous lesions in a thrombus. Lesions are judged according to the level of contrast enhancement and the CT density value, in addition to evaluating expansion of the thrombus and the primary tumor [3,7]. The thread and streaks sign in abdominal angiography could also be a useful indicator of infiltration of hepatocellular carcinoma into the portal venous system. This sign indicates the development of bundles of tiny blood vessels in the thrombus in the late arterial phase [10], which was also reported in a case with infiltration of islet cell carcinoma into the portal vein [11]. Regarding PET-CT, whereas a standardized uptake value (SUV) max >3.35 as a cutoff criterion for malignant infiltration into the portal venous thrombosis was reported to be accurate, with a sensitivity and specificity of 93% and 80% [8], respectively, the specificity of visual judgment is much lower at only 64% [8]. Regrettably, in this case, we visually diagnosed the absence of malignant invasion into the thrombus, without using SUV max. Although we did not perform angiography or contrast-enhanced ultra-sonography because of the failure to suspect tumor infiltration, it might have been unlikely that these modalities would have provided a correct diagnosis in the early phase of this patient’s course, with the presence of only a small number of malignant cells in the thrombus [2,3,7].
The definitive diagnosis of infiltration of malignant cells into a thrombus in the portal venous system requires histopatho-logical examinations [12–14]. A case of hepatocellular carcinoma producing portal venous thrombosis before the appearance of a definite mass lesion in the liver has been reported, which suggests the necessity and usefulness of liver biopsy targeting the thrombus and surrounding portal venous system [14], especially when the thrombus etiology is inapparent [12]. In addition, a case of hepatocellular carcinoma invading the endothelium of the portal vein before showing any mass lesions in the liver was diagnosed by CT-guided portal vein biopsy [14], and another case of malignant melanoma with no signs of mass lesions in the liver was diagnosed by liver biopsy [15]. These reports also suggest the usefulness of liver biopsy in cases showing portal venous thrombosis without tumorous lesions in the liver. Although brush cytology of the common bile duct performed through ERCP in the 8th month after discharge contributed a great deal to our suspecting tumor infiltration as the cause of the portal venous thrombosis in our case, a mass lesion was already present in the liver at the time of the biopsy. Furthermore, MRI in the 2nd month revealed thickening and stenosis of the common bile duct, which suggested that we could have made the same diagnosis by brush cytology of the common bile duct through ERCP at that point.
Conclusions
It is essential to distinguish infiltration of malignant cells into the portal venous system from other more benign conditions as a cause of portal venous thrombosis owing to marked differences in the prognosis of these conditions. In patients with portal venous thrombosis of unknown origin, continuation of meticulous investigations with careful observational follow-up is essential because initial investigations could fail to identify the hidden causative malignancy. In particular, liver biopsy in addition to brush cytology of the common bile duct through ERCP could lead to a diagnosis of infiltration of malignancy into the portal venous system as a cause of thrombosis.
Figures
References:
1.. Rajani R, Björnsson E, Bergquist A, The epidemiology and clinical clinical features of portal vein thrombosis: a multicentre study: Aliment Pharmacol Ther, 2010; 32(9); 1154-62
2.. DeLeve LD, Valla D-C, Garcia-Tsao G, Vascular disorders of the liver: Hepatology, 2009; 49(5); 1729-64
3.. del Carmen Manzano-Robleda M, Barranco-Fragoso B, Uribe M, Portal vein thrombosis: What is new?: Ann Hepatol, 2015; 14(1); 20-27
4.. Badi Y, Badro N, Dhawan S, Portal vein thrombosis: the overlooked association between pancreatic cancer and PVT: Oncol Cancer Case Rep, 2017; 3(128); 1-2
5.. Søgaard KK, Farkas DK, Pedersen L, Splanchnic venous thrombosis is a marker of cancer and a prognostic factor for cancer survival: Blood, 2015; 126(8); 957-63
6.. Ögren M, Bergqvist D, Björck M, Portal vein thrombosis: Prevalence, patient characteristics and lifetime risk: A population study based on 23796 consecutive autopsies: World J Gastroenterol, 2006; 12(13); 2115-19
7.. Margini C, Berzigotti A, Portal vein thrombosis: The role of imaging in the clinical setting: Dig Liver Dis, 2017; 49(2); 113-20
8.. Hu S, Zhang J, Cheng C, The role of 18 F-FDG PET/CT in differentiating malignant from benign portal vein thrombosis: Abdom Imaging, 2014; 39(6); 1221-27
9.. Tarantino L, Francica G, Sordelli I, Diagnosis of benign and malignant portal vein thrombosis in cirrhotic patients with hepatocellular carcinoma: Color Doppler US, contrast-enhanced US, and fine-needle biopsy: Abdom Imaging, 2006; 31(5); 537-44
10.. Matsumoto N, Ogawa M, Abe M, The thread and streaks sign: J Med Ultrason (2001), 2009; 36(2); 99-100
11.. Bok E, Cho K, Williams D, Venous involvement in islet cell tumors of the pancreas: Am J Roentgenol, 1984; 142(2); 319-22
12.. Sule A, Borja A, Chin TJ, Progression of thrombus in portal vein, superior mesenteric vein, and splenic vein even on anticoagulation in a patient with ascending colonic malignancy with liver metastasis: Portal vein thrombosis versus portal vein tumor thrombosis: Int J Angiol, 2016; 25(05); e97-99
13.. Igarashi H, Shinozaki S, Mukada T, A case of acinar cell carcinoma of the pancreas that formed extensive tumor thrombus of the portal vein: Clin J Gastroenterol, 2009; 2(2); 96-102
14.. Poddar N, Avezbakiyev B, He Z, Hepatocellular carcinoma presenting as an incidental isolated malignant portal vein thrombosis: J Gastrointest Cancer, 2012; 43(3); 486-89
15.. Shan G-D, Xu G-Q, Chen L-H, Diffuse liver infiltration by melanoma of unknown primary origin: One case report and literature review: Intern Med, 2009; 48(24); 2093-96
Figures
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953068
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133