06 July 2021: Articles 
Massive Pulmonary Embolism Causing Cardiac Arrest Managed with Systemic Thrombolytic Therapy: A Case Report
Challenging differential diagnosis, Management of emergency care, Rare disease, Clinical situation which can not be reproduced for ethical reasons
Stephanie R. Welle1ABCDEF, Michael F. Harrison123ABCDEF*DOI: 10.12659/AJCR.931215
Am J Case Rep 2021; 22:e931215






Abstract
BACKGROUND: Approximately 290 000 cases of in-hospital cardiac arrest occur annually, the majority of which are due to cardiac or respiratory causes. Cardiac arrest due to acute pulmonary embolism (PE) is associated with a 90% incidence of mortality and, if identified, it can be treated with systemic thrombolytics. Here, we describe a case in which the outcome for such an event was favorable.
CASE REPORT: A 66-year-old woman was admitted with multiple rib and left ankle fractures due to accidental trauma. Before undergoing orthopedic surgery, she experienced a cardiac arrest with pulseless electrical activity, which was witnessed. She had refractory hypoxia and hypotension following intubation and a brief initial return of spontaneous circulation (ROSC) before a second cardiac arrest. A 100-mg bolus dose of systemic thrombolytic therapy was promptly administered, with rapid achievement of sustained ROSC. The results of a subsequent electrocardiogram, echocardiogram, and computed tomography scan further supported the diagnosis of acute PE with right heart strain. Supportive care in the Intensive Care Unit resulted in full neurological recovery and she was discharged to a physical rehabilitation facility 12 days after her cardiac arrest.
CONCLUSIONS: Systemic thrombolytic therapy is beneficial for cardiac arrest due to acute PE.
Keywords: Advanced Cardiac Life Support, Death, Sudden, Cardiac, Pulmonary Embolism, Tissue Plasminogen Activator, Cardiopulmonary Resuscitation, Echocardiography, Fibrinolytic Agents, Heart Arrest, Thrombolytic Therapy
Background
Approximately 290 000 cases of in-hospital cardiac arrest occur annually in the United States [1,2]. Over the past decade, the incidence of in-hospital cardiac arrest in adult patients has been increasing [2], with survival to discharge rates optimistically hovering at approximately 20% to 25% [2]. The majority of these events occur on the general medical and surgical wards and approximately 50% to 60% of them are attributed to cardiac causes (ie, myocardial infarction, arrhythmia, heart failure); the remainder are largely attributed to respiratory insufficiency [1]. Acute pulmonary embolism (PE) that causes an in-hospital cardiac arrest is a cardiopulmonary event associated with a mortality rate of approximately 90% [3,4]. The majority of the deaths occur within 1 h of hemodynamic instability [5]. A recent review highlighted the association between accurately identifying the precipitating cause of a cardiac arrest and providing appropriate and effective resuscitative and post-cardiac arrest care to maximize the chances of favorable outcomes [1].
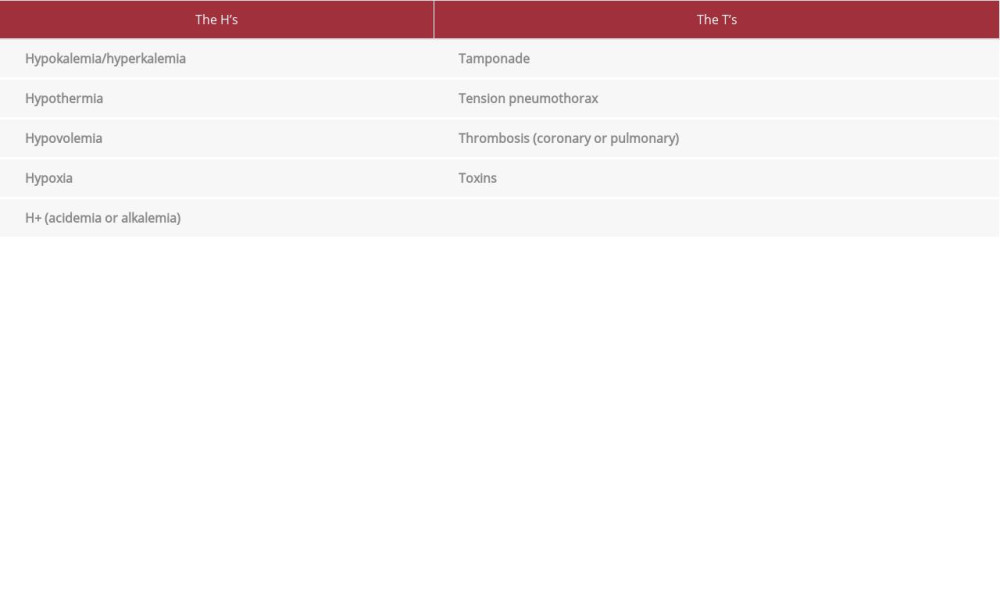
The reversible causes of in-hospital cardiac arrests are commonly referred to as the “H’s and T’s” during advanced cardiac life support (ACLS) education for medical providers. These diagnoses should be used as a list of potential causes (Table 1) to determine the appropriate algorithm to follow during resuscitation and subsequent aftercare [6,7]. Acute PE, as listed under “thrombosis,” is an item to be considered for any in-hospital cardiac arrest, but specific guidance is lacking regarding treatment with thrombolytic therapy [8]. Recommendations based upon the consensus opinion of experts or the results of smaller studies state that treatment with systemic thrombolytics “should” or “may” be “considered” in the appropriate clinical scenario [7–9]. As such, the administration of systemic thrombolytic therapy is dependent upon the clinical practice, experience, and comfort of the individual provider [8]. One source describes thrombolytic therapy for cardiac arrest due to PE as a “last-resort option” [6], which may be a widely held opinion among resuscitation team members. This view may result in hesitation by a clinician in arriving at an early diagnosis of PE, followed by administration of thrombolytics. However, prompt delivery of thrombolytic therapy in the setting of cardiac arrest due to an acute PE can significantly improve post-cardiac arrest outcomes [5,8].
We present the case of a 66-year-old woman with multiple comorbidities who presented to the hospital with multiple rib and left lower-extremity fractures secondary to accidental trauma. While awaiting orthopedic intervention, she experienced an in-hospital cardiac arrest. The etiology of her cardiac arrest, along with clinical clues and the rationale that prompted the interventions, are described to illustrate how prompt identification can lead to delivery of appropriate therapy and patient survival with a favorable neurological outcome.
Case Report
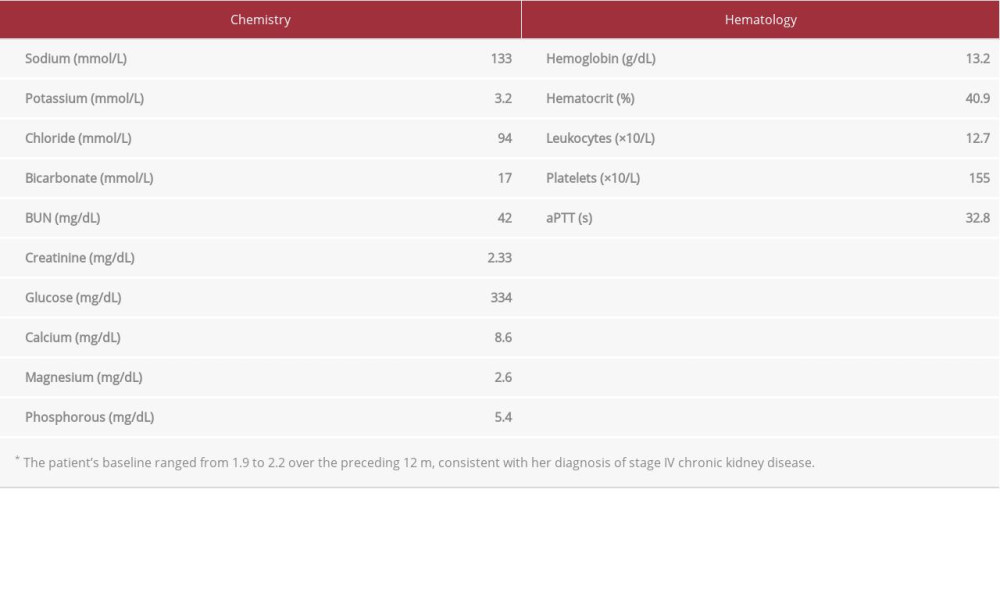
A non-smoking, functionally independent, 66-year-old woman with a history of obesity (body mass index [BMI] 40.0 kg/ m2), stage IV chronic kidney disease (CKD) due to hypertensive and diabetic nephropathy, hypertension, hyperlipidemia, and insulin-dependent type II diabetes mellitus presented to the Emergency Department (ED) after a fall while loading a 4-wheel all-terrain vehicle into the bed of a truck. She was diagnosed with acute nondisplaced fractures of the seventh through eleventh ribs on the left side as well as comminuted fractures of the left calcaneus and distal fibula. She was admitted to the General Medical Ward for management and optimization of her chronic diseases before orthopedic intervention. After an orthopedic consultation, the decision was made to arrange for helicopter transfer to an affiliated tertiary care center for definitive operative management. Initially, the patient’s hospitalization was uneventful and she was hemodynamically stable with no need for supplemental oxygen. The results of her laboratory evaluation on the morning of and preceding her cardiac arrest are presented in Table 2.
Late in the morning on the third day of admission and before aeromedical transfer, the patient experienced acute and rapid clinical deterioration. She was found to be hypoxic (lowest recorded oxygen saturation 76% with a pulse oximeter) and dyspneic (respiratory rate estimated to be 20 to 30). The patient was describing her symptoms to a Rapid Response Team nurse when she lost consciousness (T-0: 00). She had been given no medications recently (>2 h) for management of pain, anxiety, or agitation. She did not have a pulse and the Intensive Care Unit (ICU) resuscitation team was called to the bedside (T+0: 02). Cardiopulmonary resuscitation (CPR) was initiated, as per the ACLS treatment algorithm, and the initial rhythm was pulseless electrical activity (PEA). After less than 4 min of CPR and 2 doses of i.v. epinephrine (1 mg, 1: 10 000 concentration), the patient had return of spontaneous circulation (ROSC) (T+0: 04). She was endotracheally intubated without difficulty on the first attempt (endotracheal tube [ETT] size 7.5, depth 22 cm) (T+0: 05). Following intubation, the patient was persistently hypoxic with oxygen saturations measured in the 69% to 78% range on pulse oximetry. Oxygen was flowing at >15 L/min and the patient was easy to ventilate with a bag-valve device. She had symmetric breath sounds in both lungs but none over the gastric region. While the cause of the patient’s hypoxia was being investigated, she became brady-cardic and had a subsequent cardiac arrest with PEA (T+0: 07). Given the clinical setting of acute hypoxic cardiac arrest in a patient with a recent history of orthopedic trauma, the responding intensivist presumptively determined that massive PE was the most likely diagnosis. The decision was made to administer systemic lytic therapy (T+0: 08) with a 100-mg bolus of tissue plasminogen activator (tPA) (T+0: 11). ROSC was achieved within 4 min of initiation of the second round of CPR (T+0: 13) and the patient had femoral central venous catheter and arterial lines placed for administration of vasopressor therapy and associated hemodynamic monitoring (T+0: 21).
Post-resuscitation evaluation at bedside prior to transfer to the ICU included an electrocardiogram (ECG) (Figure 1) (T+0: 23) and a portable chest X-ray (T+0: 27) with an anterior-posterior exposure (Figure 2). The chest X-ray demonstrated appropriate placement of the ETT, increased displacement of the seventh rib fracture, and a new airspace opacity in the lower left lung field, hypothesized to be a progressive pulmonary contusion. The ECG revealed a tachycardic rhythm (HR=127 bpm), a new right bundle branch block, and diffuse t-wave inversions. The patient was then moved to the ICU for post-resuscitation care (T+0: 33).
On arrival at the ICU, the patient required nasal packing for a brisk hemorrhage from the right nares. She was persistently hypotensive, requiring vasopressor support (norepinephrine, 0.9 µg/kg/min) to maintain mean arterial pressure (MAP) >65 mmHg. The patient also required 100% oxygen to maintain oxygen saturation >90%. Arterial blood gas results obtained immediately following placement of the femoral arterial line were pH 6.97, pCO2 84 mmHg, and pO2 67 mmHg. Her mechanical ventilator settings were a tidal volume of 350 mL (6.2 cc/kg of ideal body weight), respiratory rate of 30 bpm, and positive end expiratory pressure of 8 cmH2O; her lung mechanics revealed a mean airway pressure of 13 cmH2O. The patient was given an i.v. dose of 50 mEq of 8.4% sodium bicarbonate, with transient improvement in hemodynamics as determined by a 4 µg/kg/min reduction in her vasopressor requirements. The intensivist performed a point-of-care ultrasound of the patient’s cardiac function, which revealed hyperdynamic left ventricular function, a dilated right ventricle with hypokinesis, and septal bowing (T+0: 48). Image quality was limited due to body habitus but an emergent formal echocardiogram with i.v. contrast performed by a staff cardiologist approximately 2 h post-ROSC confirmed these findings (Figure 3) (T+2: 00).
In light of the patient’s persistent hemodynamic instability with pre-existing stage IV CKD, her family was updated on the diagnostic and treatment options. They consented to a computed tomography angiogram (CTa) of the chest to evaluate thrombotic burden and suitability for advanced therapy, such as catheter-assisted thrombolysis. The interventional radiologist was present in the radiology suite as the study was obtained and reviewed the images in real time (T+2: 51). The CTa demonstrated multiple acute pulmonary emboli in the segmental and subsegmental right upper and lower lobes and the left lower lobe pulmonary arteries (Figure 4). The patient also had an acute contusion in the presternal region with possible non-displaced buckle fracture of the sternum, which was likely a sequela of CPR. She was deemed to not be a candidate for additional advanced therapies and was returned to the ICU for continuation of the current management plan.
Therapeutic hypothermia was not provided to the patient because of concern about increased risk of coagulopathy in the setting of systemic thrombolytic therapy. Her nasal hemorrhage was stabilized with nasal packing and monitoring was ongoing for possible intrathoracic hemorrhage following CPR at the sites of the sternal fracture and the pre-existing rib fractures.
Over the next 24 h, the patient’s hemodynamic instability resolved and she was titrated off vasopressor therapy. A venous duplex ultrasound identified an acute deep vein thrombosis in the proximal right peroneal veins with no findings in the left lower extremity. She was started on therapeutic anticoagulation with infusion of low-molecular-weight heparin and later transitioned to an oral vitamin K antagonist for long-term anticoagulation. Her oxygenation improved with decreasing requirements for ventilatory support. She was grossly neurologically intact, and 36 h after ROSC she was communicating with her family using written notes while intubated. Approximately 48 h after ROSC, she was taken off mechanical ventilation and no reintubation was needed for the remainder of her hospitalization. The patient required hemodialysis briefly via a temporary dialysis catheter but her renal function recovered to baseline within 7 days of the contrast administration for the CTa. Orthopedics recommended conservative non-operative management of her lower-extremity fractures. On the 12th day after her cardiac arrest, the patient was discharged to an inpatient rehabilitation facility. During the following 12 months, the patient continued to do well and she has not required further evaluation in the ED or admission to the hospital. She completed rehabilitation and has returned to her prehospitalization level of activity.
Discussion
The present case report describes the clinical course of a patient who experienced an in-hospital cardiac arrest caused by an acute PE, which was witnessed, and who fully recovered after treatment with systemic thrombolytics. The resuscitative technique was promptly tailored to address the most likely reversible condition of cardiac arrest, based on the patient’s clinical history and findings. The literature, to be reviewed in the following discussion, demonstrates that systemic thrombolytic therapy for in-hospital cardiac arrest may be safer and more beneficial than widely believed when administered to appropriate patients.
Historically, the administration of systemic thrombolysis during CPR has been associated with survival rates of 55% to 100% despite the perceived contraindication associated with coincident CPR [3,4,8,10–12]. Coagulopathy is one of the most commonly encountered contraindications to systemic thrombolytic therapy [13], but thrombolytic therapy has been provided safely to a small number of patients in cardiac arrest who were being treated with vitamin K antagonists [14]. Bleeding is the most common complication, but is highly associated with preceding operative interventions [3] and independent of the performance or duration of chest compressions [8,10,11,14,15]. The incidence of severe or life-threatening bleeding in patients who have experienced cardiac arrest and been treated with systemic thrombolytic therapy is commonly reported to be <1% [10,14], although in a meta-analysis, the rate was nearly 10% [12]. Regardless, the majority of the bleeding complications documented are manageable, with the exception of catastrophic events such as intracerebral hemorrhage [3,4,8,10,16]. Given that the mortality rate for cardiac arrest in- or out-of-hospital can be >95%, the risk-benefit analysis may favor administration of tPA followed by management of complications such as bleeding, if and when they occur [1,4,8,10,15].
There are no documented randomized controlled trials (RCTs) of the efficacy of systemic thrombolytic therapy as a treatment for in-hospital cardiac arrest due to suspected or confirmed acute PE [3,4,10,14]. A RCT was performed in patients who experienced out-of-hospital cardiac arrest, and although the sample population was very small, systemic thrombolytic therapy appeared to result in an increased rate of ROSC, but the question of survival and disability could not be addressed because of lack of statistical power [17]. A larger follow-up study of out-of-hospital cases was terminated early due to futility [16]. Many other studies [14,15], reviews [3,10], and meta-analyses [12] have demonstrated increased survival rates with minimal disability for in-hospital patients. The rapidity with which our patient recovered and was subsequently extubated is consistent with previously reported findings [14]. Specifically, a large review described the volume of evidence in support of the neuroprotective benefits of thrombolytic therapy but could not definitively identify the mechanism by which this occurs [10]. Cardiac arrest serves to activate the coagulation pathway [11,16] and it is possible that thrombolytic therapy may mitigate the secondary insults resulting from this pathophysiology. Systemic lytic therapy also may be associated with decreased rates of atrial arrhythmias after acute PE [18]. Furthermore, it is hypothesized that chest compressions in a patient with an acute PE cause mechanical fragmentation of the thrombus while augmenting microcirculation reperfusion [3,6]. In our patient, this may have been the mechanism by which subsegmental PE were identified in multiple branches of the pulmonary artery on CTa performed after her cardiac arrest.
Identifying patients with cardiac arrest who would be suitable candidates for systemic thrombolytic therapy remains challenging [17,19]. This is due to the nonspecific presentation associated with acute PE [4] but it is crucial for optimization of the risk-benefit ratio [8]. Factors that increase the risk of acute PE include a history of previous thromboembolism, surgery, or major trauma within the preceding month; active cancer; immobilization; estrogen use; tobacco use; chronic pulmonary disease; and chronic heart failure [20,21]. If thrombolytic therapy is provided to an appropriately selected patient in cardiac arrest, ROSC often occurs within minutes [10,14,19]. Even if prolonged CPR is required prior to achieving ROSC, neurologic function is often well preserved [4,6,10,15]. Our patient was given a 100-mg dose of tPA, but 50 mg has been demonstrated to provide comparable morbidity and mortality benefits to a population of patients with cardiac arrest due to confirmed massive PE [14]. In that particular case series, the 2-year survival rate approached 90% [14]. Alternatively, an out-of-hospital study was terminated for futility when thrombolytic therapy was provided to all patients with a witnessed cardiac arrest for which the presumed etiology was cardiac [16].
Conclusions
While the predominance of evidence supports the use of tPA in appropriately selected patients with cardiac arrest, the high rates of success with manageable complications do suggest a publication bias [10]. The authors of a number of publications have called for prospective RCTs with appropriately selected patient populations [3,4,8,10] while noting the challenges associated with performing such studies, from both ethical and practical perspectives. In conclusion, however, it would appear that clinicians should be aware of this treatment approach in the context of the clinical presentation of the patient they find before them. The location of a patient on the risk-benefit continuum shifts drastically with the occurrence of cardiac arrest; therapies that have previously been described as “last resorts” may now provide more benefit contextually. If the clinical situation strongly suggests acute PE as the most likely cause of a cardiac arrest, the published literature suggests that systemic thrombolytics should be strongly considered and administered as soon as practical. In patients who survive, the evidence suggests that the morbidity and mortality profile will be excellent. Our report describes just such a case with an extremely favorable outcome in an elderly woman with multiple comorbidities.
Figures
References:
1.. Andersen LW, Holmberg MJ, Berg KM, In-hospital cardiac arrest: A review: JAMA, 2019; 321(12); 1200-10
2.. Holmberg MJ, Ross CE, Fitzmaurice GM, Annual incidence of adult and pediatric in-hospital cardiac arrest in the United States: Circulation, 2019; 12(7); e005580
3.. Böttiger BW, Böhrer H, Bach A, Bolus injection of thrombolytic agents during cardiopulmonary resuscitation for massive pulmonary embolism: Resuscitation, 1994; 28(1); 45-54
4.. Laher AE, Richards G, Cardiac arrest due to pulmonary embolism: Indian Heart J, 2018; 70(5); 731-35
5.. Yamamoto T, Management of patients with high-risk pulmonary embolism: A narrative review: J Intensive Care, 2018; 6(1); 1-9
6.. Chenaitia H, Fournier M, Brun JP, Association of mechanical chest compression and prehospital thrombolysis: Am J Emerg Med, 2012; 30(6); 1015 e1–2
7.. Neumar RW, Shuster M, Callaway CW, Part 1: Executive summary: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care: Circulation, 2015; 132(18 Suppl. 2); S315-67
8.. Logan JK, Pantle H, Huiras P, Evidence-based diagnosis and thrombolytic treatment of cardiac arrest or periarrest due to suspected pulmonary embolism: Am J Emerg Med, 2014; 32(7); 789-96
9.. Members ATF, McMurray JJV, Adamopoulos S, ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC: Eur Heart J, 2012; 33(14); 1787-847
10.. Newman DH, Greenwald I, Callaway CW, Cardiac arrest and the role of thrombolytic agents: Ann Emerg Med, 2000; 35(5); 472-80
11.. Böttiger BW, Martin E, Thrombolytic therapy during cardiopulmonary resuscitation and the role of coagulation activation after cardiac arrest: Curr Opin Crit Care, 2001; 7(3); 176-83
12.. Li X, Fu Q-l, Jing X-l, A meta-analysis of cardiopulmonary resuscitation with and without the administration of thrombolytic agents: Resuscitation, 2006; 70(1); 31-36
13.. Fugate JE, Rabinstein AA, Absolute and relative contraindications to IV rt-PA for acute ischemic stroke: Neurohospitalist, 2015; 5(3); 110-21
14.. Sharifi M, Berger J, Beeston P, Pulseless electrical activity in pulmonary embolism treated with thrombolysis (from the “PEAPETT” study): Am J Emerg Med, 2016; 34(10); 1963-67
15.. Janata K, Holzer M, Kürkciyan I, Major bleeding complications in cardiopulmonary resuscitation: The place of thrombolytic therapy in cardiac arrest due to massive pulmonary embolism: Resuscitation, 2003; 57(1); 49-55
16.. Böttiger BW, Arntz H-R, Chamberlain DA, Thrombolysis during resuscitation for out-of-hospital cardiac arrest: N Engl J Med, 2008; 359(25); 2651-62
17.. Fatovich DM, Dobb GJ, Clugston RA, A pilot randomised trial of thrombolysis in cardiac arrest (The TICA trial): Resuscitation, 2004; 61(3); 309-13
18.. Hayıroğlu Mİ, Keskin M, Uzun AO, Long-term antiarrhythmic effects of thrombolytic therapy in pulmonary embolism: Heart Lung Circ, 2017; 26(10); 1094-100
19.. Zhu T, Pan K, Shu Q, Successful resuscitation with thrombolysis of a presumed fulminant pulmonary embolism during cardiac arrest: Am J Emerg Med, 2013; 31(2); 453.e1-e3
20.. Hayıroğlu Mİ, Bozbeyoğlu E, Akyüz Ş, Acute myocardial infarction with concomitant pulmonary embolism as a result of patent foramen ovale: Am J Emerg Med, 2015; 33(7); 984 e5–.e7
21.. Meyer G, Vicaut E, Danays T, Fibrinolysis for patients with intermediate-risk pulmonary embolism: N Engl J Med, 2014; 370; 1402-11
Figures
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133