29 August 2021: Articles 
Effectiveness of Saireito, a Traditional Japanese Kampo Herbal Medication, on Pacemaker-Related Pleural Effusion: A Case Report
Unusual or unexpected effect of treatment
Hiroyuki Mataki1ABCDEF*, Masamichi Yasutomi1E, Yuya Makino1E, Ayako Kunimura1E, Kenzo Fukuhara1E, Masafumi Takeda1E, Akira Kimata1E, Sonoko Hirayama1E, Toru Ozawa1E, Teruki Shin2E, Takayuki Yoshioka2E, Nobutaka Inoue1AEFDOI: 10.12659/AJCR.931247
Am J Case Rep 2021; 22:e931247






Abstract
BACKGROUND: Post-cardiac injury syndrome, including pleural effusion as a delayed complication of permanent pacemaker implantation, has rarely been reported. To resolve pleural effusion, prolonged chest tube placement is often required. Anti-inflammatory agents combined with diuretics are also often prescribed. Saireito, a Japanese herbal medication, which is a combination of Goreisan and Shousaikoto, has both anti-inflammatory and water-modulation properties and has been used for edema (lymph edema, cerebral edema) and inflammation (chronic nephritis).
CASE REPORT: We describe a 71-year-old woman with a history of syncope and bradycardia who underwent dual permanent pacemaker implantation (placed in the right chest because of a persistent left superior vena cava) without complications. Two months later, she came to the hospital as an outpatient with a dry cough, and was diagnosed with right-sided pleural effusion. A pleural fluid analysis revealed exudative effusion, according to Light’s criteria. The fluid was negative for infectious etiology. Chest X-ray, computed tomography, and echocardiography revealed no signs of pericardial effusion or perforation of the pacemaker lead to outside the heart. The pleural effusion persisted despite use of anti-inflammatory medication for several weeks and diuretics for a short period. Saireito was administered with good response; the pleural effusion resolved completely and there was no deterioration of renal function.
CONCLUSIONS: The present case highlights the clinical significance of Saireito as an effective therapeutic agent for late-onset pacemaker-related pleural effusion, without adverse effects such as renal dysfunction.
Keywords: Drugs, Chinese Herbal, Pacemaker, Artificial, Pleural Effusion, Female, Humans, Japan, Medicine, Kampo, Vena Cava, Superior
Background
Pacemaker implantation is a standard and safe therapeutic strategy for patients of all ages with bradyarrhythmia. Various complications associated with pacemaker implantation are common, but late-onset pacemaker-related pleural effusion is rarely reported [1]. Recently, Xiong et al reported 6 consecutive elderly patients with pleural effusion who had undergone a new pacemaker implantation and evaluated the clinical characteristics and therapeutic courses of pleural effusion [2]. According to their report, cases of late-onset pacemaker-related pleural effusion were treatment-resistant; patients had to be hospitalized repeatedly with thoracentesis because conventional treatments including diuretics and anti-inflammatory agents had only short-term effects, similar to a case reported by Shaukat et al [3].
Saireito (TJ-114) is a combination of 2 herbal medications, Shousaikoto and Goreisan. Shousaikoto is known as a remedy for hepatitis, and previous investigations have reported that Shousaikoto has potential as an anti-inflammatory drug [4]. In addition, Goreisan has been reported to be effective for hydrostatic modulation via the suppression of aqua-porin 4 [5]. Therefore, Saireito has both anti-inflammatory and water-utilization benefits. Saireito is composed of 12 crude drugs: 7 g of saiko, 5 g of takusha, 5 g of hange, 3 g of ougon, 3 g of soujutu, 3 g of taisou, 3 g of chorei, 3 g of ninjin, 3 g of bukuryo, 2 g of kanzo, 2 g of keihi, and 1 g of shoukyou. Takusha, soujutu, chorei, and bukuyrou, the main components of Goreisan, have an effect on regulating the amount of water in the body. Saiko and ougon, components of Shousaikoto, have anti-inflammatory effects. Saireito has been used in the treatment of chronic kidney disease, diarrhea, acute gastritis, and various edematous disorders, such as subdural hematoma, chronic lymphedema, cirrhosis, and general edema. Saireito has also widely been used to treat various inflammatory diseases, such as rheumatoid arthritis [6,7]. Recently, herbal medications have been attracting attention for their effectiveness in circulatory disease; however, the association between the use of herbal medication and pleural effusion has not been well documented. We had a case in which Saireito was effective for the treatment of late-onset pacemaker-related pleural effusion.
Case Report
A 71-year-old woman who had been previously well and had no significant past medical history was admitted to our hospital for a syncope attack after a meal. On admission, she regained consciousness, but her blood pressure was elevated to 212/76 mm Hg and her heart rate was 63 beats/min. She did not have a heart murmur. The laboratory tests showed no abnormalities (Table 1).
The electrocardiogram on admission showed normal sinus rhythm, with a left branch anterior bundle block, and high voltage of the left ventricle, with secondary ST-T changes (Figure 1A). The chest X-ray exhibited cardiomegaly. There was no indication of pneumonia or heart failure (Figure 1B). The electrocardiogram monitoring in the hospital revealed a prolonged R-R interval of 6040 ms, associated with fainting (Figure 2). From these findings, she was diagnosed with sick sinus syndrome type II. Echocardiography conducted 6 days before pacemaker implantation revealed normal function with mild left hypertrophy and mild to moderate mitral regurgitation.
A previous venography of the subclavian vein revealed a persistent left superior vena cava. Therefore, a permanent dual chamber pacemaker was implanted under fluoroscopic guidance in the right chest. Venous access was achieved by puncture of the subclavian vein, and both leads were endocardial screw-in leads. The setting rate of the implanted pacemaker was 60 to 130 pulses per min. Chest X-rays on the day of implantation, 1 day after implantation, and 6 days after implantation revealed no pleural effusion. She was discharged in 13 days without any complications.
Two months after pacemaker implantation, the patient visited the hospital as an outpatient, presenting with a dry cough. The chest X-ray and computerized tomography revealed right-sided pleural effusion (Figure 3). An echocardiogram showed no sign of pericardial effusion or perforation of the myocardium and was nearly identical to a previous echocardiogram. Thoracentesis was performed, and the fluid composition was exudative effusion, according to Light’s criteria (Table 2). A pleural fluid analysis was negative for infectious etiology, including mycobacteria, and there were no findings of malignancy. After thoracentesis, right-sided pleural effusion remained almost the same as before (Figure 4A). A pacemaker interrogation revealed no abnormality. We considered that the pleural effusion was a manifestation of a pacemaker-associated injury.
Therefore, we initiated an oral anti-inflammatory agent (acetaminophen 600 mg/day), and oral diuretics (furosemide 40 mg/day) as an initial dose, then as needed for a short period. With these treatments, the pleural effusion decreased somewhat; however, persistent right pleural effusion was present 2 months later (Figure 4B, 4C). Furthermore, the patient’s renal function deteriorated slightly (Figure 5).
To decrease pleural effusion and prevent further deterioration of renal function, we prescribed oral Saireito (an herbal substitute for anti-inflammatory agents and diuretics) at an initial dose of 9 g/day, because long-term use of anti-inflammatory agents and diuretics often causes renal damage. We also wanted to avoid the use of steroids, considering her age. Right pleural effusion completely disappeared 1 month after the administration of Saireito (Figure 4D). The patient’s renal function was also maintained (Figure 5). The patient has been followed as an outpatient and has been well and free from recurrent pleural effusion.
Discussion
In the present case, Saireito, a Japanese traditional herbal medication, played an important role in reducing pleural effusion that occurred 2 months after the implantation of a dual chamber pacemaker, without deterioration of renal function. Various drugs used in modern medicine can have adverse effects, such as renal dysfunction. Therefore, in some medical situations, traditional herbal medication is often used as an alternative to prevent adverse events [8]. Aquaporin (AQP) is a water channel and is composed of at least 13 types of isoforms. Goreisan strongly inhibits AQP3, AQP4, and AQP5 [9,10]. Interestingly, unlike western diuretics, Goreisan induces an increase of urine volume in an edematous state, but not in a dehydrated state. The precise pharmacological mechanisms of traditional herbal medications, such as Saireito and Goreisan, remain to be elucidated [11]. The use of herbal medications has attracted more attention in recent years [12]. To treat congestive heart failure, Mokubouito or Shakannzouto have often been used in addition to standard therapy, and Goreisan has been used to treat edematous states [13]. Saireito has been used for diarrhea, chronic renal disease, lymphedema, and cerebral edema. In addition, according to Takei et al, Saireito and Boiogito can improve hypertension [14].
Shousaikoto has potential as an anti-inflammatory treatment, and has been used for pneumonia, bronchitis, lymphadenitis, and chronic hepatitis. Therefore, we hypothesized that Saireito, being a combination of Goreisan and Shousaikoto, might be effective in both edematous and inflammatory states, such as in the present case [15].
Late-onset pacemaker-related pleural effusion is rare and often difficult to treat. Conventional medical treatment, including anti-inflammatory agents, colchicine, and diuretics often have little effect on late-onset pacemaker-related pleural effusion. Therefore, repeated therapeutic thoracentesis is unavoidable in some cases. In the present case, pleural effusion persisted after 2 months of an anti-inflammatory agent and diuretics. Considering not only its effectiveness, but also its renal protective properties, Saireito was administered, and the pleural effusion disappeared completely, without deterioration of renal function (Figure 5). It is worth noting that Saireito attenuates renal damage induced by diuretics. In the present case, renal protection was one of the reasons for selecting Saireito versus alternative traditional anti-inflammatory agents or diuretics. Our patient’s pleural effusion completely resolved, and renal function was maintained.
Conclusions
In conclusion, our experience indicates that the use of Saireito could resolve treatment-resistant pleural effusion as a delayed complication of pacemaker implantation, without deterioration of renal function. Whether Goreisan or Shousaikoto alone have the same effect as Saireito remains to be evaluated. Further study is required to examine the use of these agents alone for pleural effusion as a delayed complication of permanent pacemaker implantation.
Figures
Tables
Table 1.. Laboratory data on patient’s first admission revealed only mild hypokalemia. On second admission, mild hypokalemia still existed, and brain natriuretic peptide (BNP) was slightly elevated.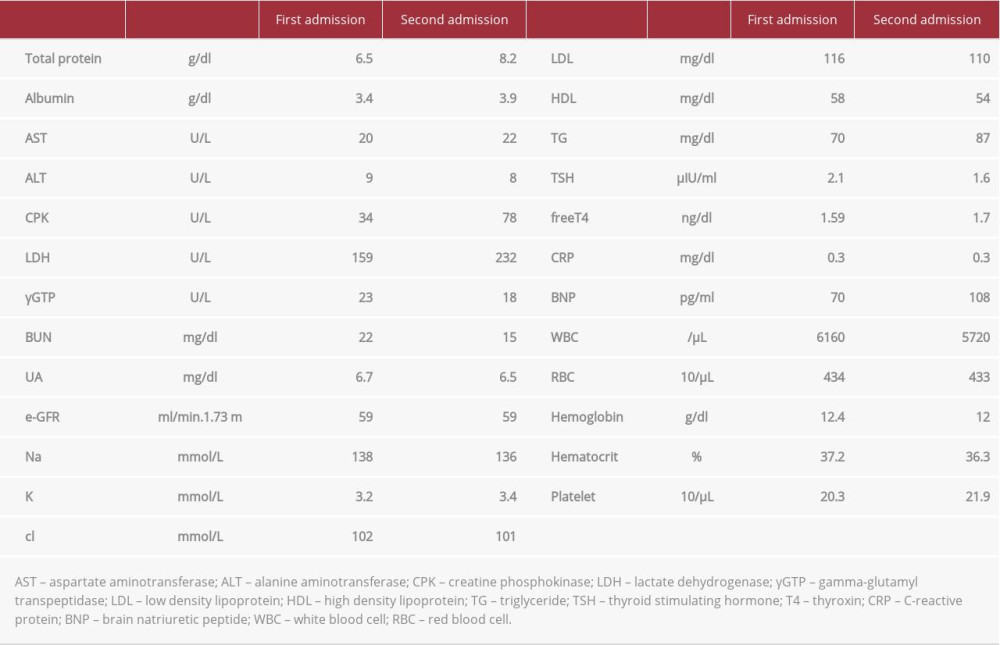 Table 2.. Pleural effusion analysis. Lactate dehydrogenase (LDH) concentration in effusion >200 IU; LDH concentration divided by serum LDH concentration >0.6. According to the Light criteria, the effusion is exudative.
Table 2.. Pleural effusion analysis. Lactate dehydrogenase (LDH) concentration in effusion >200 IU; LDH concentration divided by serum LDH concentration >0.6. According to the Light criteria, the effusion is exudative.
References:
1.. Ludwig S, Theis C, Wolff C, Complications and associated health-care costs of transvenous cardiac pacemakers in Germany: J Com Eff Res, 2019; 8(8); 589-97
2.. Xiong M, Zhang Z, Hu K, Dong M, Hu W, Recurrent, late-onset pleural effusions in elderly patients receiving pacemaker therapy: Case Rep Med (Baltimore), 2018; 97(43); e12915
3.. Shaukat MHS, Shabbir MA, Mookherjee S, Peredo-Wende R, Successful use of anakinra for colchicine-intolerant, corticosteroid-dependent recurrent pericarditis secondary to postcardiac injury syndrome after pacemaker placement: BMJ Case Rep, 2019; 12(4); e229117 4
4.. Kim A, Im M, Ma JY, Sosiho-tang ameliorates cachexia-related symptoms in mice bearing colon 26 adenocarcinoma by reducing systemic inflammation and muscle loss: Oncol Rep, 2016; 35(3); 1841-50
5.. Nakano T, Nishigami C, Irie K, Goreisan prevents brain edema after cerebral ischemic stroke by inhibiting aquaporin4 upregulation in mice: J Stroke Cerebrovasc Dis, 2018; 27(3); 758-63
6.. Morimoto N, Kakudo N, Mitsui T, The effectiveness of Saireito, a traditional Japanese herbal medicine, in reducing postoperative edema after acquired ptosis surgery: A prospective controlled trial: Evid Based Complement Alternat Med, 2018; 2018; 4742305
7.. Nagai A, Shibamoto Y, Ogawa K, Therapeutic effects of Saireito (Chai-Ling-Tang), a traditional Japanese herbal medicine, on lymphedema caused by radiotherapy: A case series study: Evid Based Complement Alternat Med, 2013; 2013; 241629
8.. Liu L, Liu C, Wang Y, Herbal medicine for anxiety, depression and insomnia: Curr Neuropharamacol, 2015; 13(4); 41-93
9.. Inada R, Miyamoto K, Tanaka N, Oryeongsan (Goreisan) ameliorates experimental autoimmune encephalomyelitis: Intern Med, 2020; 59; 55-60
10.. Goto S, Kato K, Yamamoto T, Effectiveness of Goreisan in preventing recurrence of chronic subdural hematoma: Asian J Neurosurg, 2018; 13; 370-74
11.. Sasaki H, Kimizuka Y, Ogata H, Successful control of dasatinib-related chylothorax by the Japanese herbal medicine “Goreisan”: Intern Med, 2019; 58(21); 3139-41
12.. Wagner L, Cramer H, Klose P, Herbal medicine for cough: A systemic reviews and meta-analysis: Forsch Komplementmed, 2015; 22; 359-68
13.. Yano Y, Yano H, Takahashi H, Goreisan inhibits upregulation of aqua-porin 4 and formation of cerebral edema in the rat model of juvenile hypoxic-ischemic encephalopathy: Evid Based Complement Alternat. Med, 2017; 2017; 3209219
14.. Takei H, Nakai Y, Hattori N, The herbal medicines Saireito and Boiogito improve the hypertension of preeclamptic rats induced by nomega-nitoro-L-arginine methyl ester: Phytomedicine, 2007; 14(9); 591-600
15.. Fitzgerald DB, Waterer GW, Read CA, Steroid therapy and outcome of parapneumonic pleural effusions (STOPPE): Study protocol for a multi-center, double-blinded, placebo-controlled randomized clinical trial: Medicine (Baltimore), 2019; 98(43); e17397
Figures
Tables
Table 1.. Laboratory data on patient’s first admission revealed only mild hypokalemia. On second admission, mild hypokalemia still existed, and brain natriuretic peptide (BNP) was slightly elevated.Table 2.. Pleural effusion analysis. Lactate dehydrogenase (LDH) concentration in effusion >200 IU; LDH concentration divided by serum LDH concentration >0.6. According to the Light criteria, the effusion is exudative.Table 1.. Laboratory data on patient’s first admission revealed only mild hypokalemia. On second admission, mild hypokalemia still existed, and brain natriuretic peptide (BNP) was slightly elevated.Table 2.. Pleural effusion analysis. Lactate dehydrogenase (LDH) concentration in effusion >200 IU; LDH concentration divided by serum LDH concentration >0.6. According to the Light criteria, the effusion is exudative. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133