04 May 2021: Articles 
COVID-19 Presentation in Patients with Sickle Cell Disease: A Case Series
Rare coexistence of disease or pathology
Amber Chen-Goodspeed1ABCDEF*, Modupe Idowu2ADEFGDOI: 10.12659/AJCR.931758
Am J Case Rep 2021; 22:e931758






Abstract
BACKGROUND: Certain health conditions have been proven to have an effect on the severity of COVID-19, the disease caused by SAR-COV-2. The list of identified comorbid conditions includes hematological diseases, with sickle cell disease (SCD) falling into this category.
CASE REPORT: This case series examines the history, presentation, and clinical course of 5 patients with SCD who tested positive for SAR-COV-2 during the spring and summer of 2020. These patients experienced COVID-19 severities ranging from a mild cough and congestion to 8-day hospitalizations requiring blood transfusions.
CONCLUSIONS: While there is still a great amount of research on the interaction between COVID-19 and SCD needed, from this study we have concluded that patients with SCD do not always present with the classic COVID-19 triad of cough, shortness of breath, and fever. Often, these patients present with symptoms of vaso-occlusive crisis (VOC), including severe leg, flank, and chest pain, as was seen in 4 of 5 of our patients. We, and several other researchers, believe that this association between COVID-19 and VOC could be due to COVID-19 triggering inflammatory cytokines (notably IL-6) leading to system-wide inflammation, which induces sickling of the red blood cells. Based on this report, we recommend that SCD patients presenting with VOC who have had exposure to SAR-COV-2 be promptly tested for SAR-COV-2 to guide treatment and reduce mortality and morbidity in this vulnerable population.
Keywords: Anemia, Sickle Cell, COVID-19, Hemoglobin, Sickle, Sickle Cell Trait, Blood Transfusion, COVID-19, Chest Pain, Cytokines, Flank Pain, SARS-CoV-2
Background
COVID-19 disease, which is caused by SARS-COV-2 infection, has been shown to cause severe negative health effects in people with a number of comorbidities, one of which is sickle cell disease (SCD), a disease in which red blood cells (RBCs) convert to a sickle shape when carrying inadequate oxygen. Patients with SCD are at a higher risk of developing respiratory infections and pulmonary complications such as acute chest syndrome (ACS), pulmonary embolisms, and asthma, making their risk of respiratory complications from COVID-19 higher [1,2]. Furthermore, other published cases of COVID-19 in patients with SCD have shown that COVID-19 can trigger a vaso-occlusive crisis (VOC), a common complication of SCD in which sickled RBCs block vessels, leading to ischemia and severe pain [2]. Here, we present a case series of 5 patients with SCD who presented with symptoms ranging from the classic COVID-19 triad of dyspnea, cough, and fever to patients who required weeklong hospitalizations due to VOC, despite being clinically asymptomatic for COVID-19.
Case Reports
CASE 1: 30-YEAR-OLD MAN WITH HBSS:
The first case is that of a 30-year-old man with hemoglobin SS (HbSS), a past medical history of recurrent sickle cell pain crises requiring hospitalizations, sepsis with acute hypoxic respiratory failure, a cholecystectomy, multiple VOCs, and an 11-year history of cigarette use. His current medications included cyclobenzaprine 10 mg as needed (p.r.n.) daily for muscle spasm, hydroxyurea 1000 mg daily, oxycodone 30 mg every 4 h p.r.n. for pain, and oxycodone 80 mg extended-release every 12 h.
The patient presented to the emergency department (ED) with right lower extremity (LE) pain following a minor motor vehicle collision. In the ED, the patient was noted to have a pulse oximetry (SpO2) of 89% on room air, blood pressure (BP) of 106/61 mmHg, heart rate (HR) of 100 beats per min (bpm), respiratory rate (RR) of 18 breaths per min, hemoglobin (Hgb) of 8.9 g/dL, and a reticulocyte count of 9.5%. A chest X-ray performed in the ED showed no acute cardiopulmonary findings, and the patient was discharged. The next day, the patient went to a local hospital for assessment of continued right LE and new onset right groin pain. A urinalysis was performed and showed no abnormalities, and the patient was discharged the same day as arrival.
On day 3 of his clinical course, the patient came to our clinic for continued right LE pain. The patient’s wife expressed concern for possible COVID-19 due to the patient’s ongoing pain and decreased oxygen saturation. The patient denied fever, cough, and upper respiratory symptoms at the time of arrival. In the clinic, the patient had a temperature of 36.7oC, HR of 77 bpm, RR of 18 breaths per min, BP of 106/55, and SpO2 of 96%. His lungs were clear to auscultation, and his respirations were non-labored. The remainder of the patient’s physical exam showed no abnormalities.
The significant laboratory findings from the clinic visit included a total bilirubin of 5.4 mg/dL, hematocrit (Hct) of 24.9%, Hgb of 8.9 g/dL, monocyte count of 1.2 K/CMM, platelet count of 369 K/CMM, lymphocyte count of 10.4 K/CMM, neutrophil count of 3.5 K/CMM, RBC count of 3.05 M/CMM, and a white blood cell (WBC) count of 12 K/CMM. A chest X-ray was performed and showed no acute cardiopulmonary findings, a ventilation/perfusion scan showed no evidence of pulmonary embolism, and a computed tomography (CT) scan without contrast showed basilar atelectasis bilaterally with some plate-like atelectasis in the bases without consolidation and cardiomegaly, indicative of chronic SCD [3]. An ultrasound of the leg was negative for deep vein thrombosis (DVT), and it was concluded that the patient’s pain was likely due to a VOC. The patient was admitted for observation and pain management. He was started on prophylactic enoxaparin for DVT prevention. On day 2 of his hospital stay, the patient’s laboratory test results were significant for a WBC count of 14.1 K/CMM, Hgb of 6.7g/dL, Hct of 17.6%, monocyte count of 2.1 K/CMM, platelet count of 309 K/CMM, lymphocyte count of 12.7 K/CMM, and neutrophil count of 1.4 K/CMM. The patient received a simple trans-fusion of 1 unit of packed RBCs for treatment of his hypoxia and VOC. The patient remained in the hospital for a total of 4 days before his hypoxia and pain improved. On the day of discharge, the patient received the SARS-COV-2 RT-PCR test, which was positive, indicating current COVID-19. The patient was released and asked to self-quarantine and to return if he had increased work of breathing or dyspnea.
Two weeks following discharge from the hospital, the patient was seen in the hematology clinic and confirmed improvement of pain. During this visit he denied fever, cough, or other respiratory symptoms.
CASE 2: 30-YEAR-OLD MAN WITH HBSS:
Case 2 is that of a 30-year-old man with a medical history significant for HbSS, complicated by 3 to 4 pain crises per year, which had increased over the past year. He denied a history of ACS or cerebral vascular accident. At the time of presentation, the patient’s medications included hydroxyurea 1500 mg daily and folic acid 1 mg daily.
The patient presented to the ED for fever, cough, sinus congestion, and generalized body pain over the previous 2 days. Owing to his constellation of symptoms and his medical history, he was tested for SARS-COV-2 in the ED. The result of the SARS-COV-2 RT-PCR test was positive. Significant findings upon arrival at the ED were high temperature of 37.5°C, high total bilirubin of 3.1 mg/dL, low Hct of 28.1%, low Hgb of 9.2 g/dL, high lymphocyte count of 10.4 K/CMM, low RBC count of 4.15 M/CMM, reticulocyte of 4.2%, and high WBC count of 15 K/CMM. The patient was admitted to the hospital for observation. A chest X-ray was performed upon admission and showed no significant clinical findings indicative of COVID-19, pneumonia, or ACS. The patient remained in the hospital for 2 days. During his stay, he never experienced acute respiratory distress, dyspnea, or high-grade fever. Also during his hospitalization, his sickle cell pain crisis was managed with intravenous (i.v.) morphine, and a second chest X-ray performed at discharge showed no infiltrates or consolidation in the lungs concerning for ACS or COVID-19 pulmonary involvement.
CASE 3: 49-YEAR-OLD WOMAN WITH HBSC:
The third case is that of a 49-year-old woman with hemoglobin SC disease with a past medical history of right avascular necrosis of the hip, rheumatoid arthritis, daily chronic musculoskeletal pain, and bilateral retinopathy. The patient denied ACS and stroke and had only 1 lifetime blood transfusion. Her medications included baclofen 5 mg orally every 8 h p.r.n. for muscle spasm, ergocalciferol 1.25 mg weekly, folic acid 1 mg daily, hydrocodone-acetaminophen 10 to 325 mg every 8 h p.r.n. for pain, promethazine HCl 25 mg twice daily p.r.n. for nausea or vomiting, and tofacitinib XR 11 mg daily.
The patient was seen via telemedicine for a 2-day history of cough, fever, pains in the arms and chest wall, consistent with those felt during a VOC, and a positive SARS-COV-2 RT-PCR test. No shortness of breath (SOB) was reported by the patient at the visit, and her temperature was unable to be assessed by telemedicine. One week prior to her telemedicine visit, the patient had a fever with a temperature of 38.1°C, diarrhea, and loss of taste and smell, which progressed to a cough and constant 10/10 severity pain in both arms, both legs, and chest wall. Her cough progressed from dry to productive, and she developed SOB at rest.
The patient was advised to go to the ED after her telemedicine visit for assessment of the SOB and cough. In the ED, the patient’s pulse oximetry reading was 98%, and she was treated with albuterol MDI. She continued dextromethorphan 20 mg every 4 h as needed for cough, was given a lidocaine patch p.r.n. for pain management, and was discharged. She followed up 2 days after ED discharge at the outpatient hematology clinic via telemedicine and reported having persistent cough but denied SOB or development of new symptoms.
CASE 4: 23-YEAR-OLD MAN WITH HBSS:
The fourth case is that of a 23-year-old man with HbSS disease and a past medical history significant for 3 to 4 pain crises per year requiring hospitalization, multiple episodes of ACS (most recently 4 months prior, which required a packed RBC transfusion), priapism, avascular necrosis of the bilateral humeral heads, hypertension, and major depressive disorder. His medications included hydroxyurea 1500 mg daily, lisinopril 10 mg daily, duloxetine 60 mg daily, naproxen 500 mg every 8 h p.r.n. for pain, and hydromorphone HCl 4 mg orally (p.o.) every 6 h p.r.n. for severe pain.
The patient was seen via telemedicine due to recent exposure to someone with COVID-19. His chief symptoms were chronic low back pain and pain in both arms that started 4 to 5 days prior to his clinic visit. At the time of his visit, he denied cough, SOB, vomiting, diarrhea, or changes in smell or taste. His only pertinent physical examination finding was icteric sclera, and he was instructed to receive a SARS-COV-2 test. The patient was advised to use hydromorphone HCl 4 mg every 6 h p.r.n. for severe pain and to go to the ED if his pain did not respond to the medication.
Fifteen minutes after the telemedicine visit ended, the patient’s pain escalated to a severity of 9 out of 10, and he developed SOB and a cough, prompting him to go to the ED. His vital signs on arrival to the ED were significant for tachycardia at 124 bpm, 88% O2 saturation on room air, temperature of 39.4°C, RR of 26 breathes per min, chest X-ray that was consistent with ACS and showed multifocal airspace opacities most consistent with pneumonia, and a positive on-site SARS-COV-2 RT-PCR test. Physical examination findings included dry mucosal membranes and rales bilaterally with normal respiratory effort. The labs drawn in the ED were significant for a total bili-rubin of 7.3 mg/dL, a D-dimer level of 10.12 µg/mL, C-reactive protein level of 171 mg/L, Hgb of 7.8 g/dL, platelet count of 237 K/CMM, lymphocyte count of 3.8 K/CMM, and neutrophil count of 10.4 K/CMM. The patient received 4 L O2 via nasal cannula; azithromycin, ceftriaxone, morphine, and dexamethasone to treat and prevent infection; i.v. morphine for pain management; and enoxaparin 80 mg for 12 h for thrombosis prophylaxis because of his high D-dimer level. He was admitted to the hospital for continued treatment.
On day 1 of hospitalization, the patient received a transfusion of 1 unit of packed RBCs, his Hgb level increased to 8.8 g/dL, his D-dimer levels began down-trending, and he was switched from i.v. morphine to his home pain medication regimen of oral morphine immediate-release 15 mg every 4 h and ibuprofen 600 mg every 8 h. His laboratory results and vital signs were significant for a temperature of 38.8°C, SpO2 of 94%, Hct of 25.5%, RBC count of 2.94 M/CMM, WBC count of 14.8 K/CMM, lymphocyte count of 2.2 K/CMM, monocyte count of 2.2 K/ CMM, platelet count of 267 K/CMM, and neutrophil count of 12 K/CMM. On day 2 of hospitalization, the patient had been afebrile for 24 h, with a maximum temperature of 37°C; however, his VOC pain levels increased, and i.v. morphine was administered again for pain control. The patient continued to have a cough and SOB. On day 3 of hospitalization, he continued to cough without SOB, and was weaned down to 1 L of O2 via nasal cannula. He returned to his home oral pain management regimen, and was switched from therapeutic dosing of enoxaparin to a prophylactic dosage of 40 mg subcutaneous injection daily, per published COVID-19 anticoagulation precautions [5]. His labs were significant for an increase in Hbg level to 9.2 g/dL, which later began down-trending over the course of the day, decrease in D-dimer level to 3 µg/mL, platelet count of 278 K/CMM, lymphocytes count of 2.4 K/CMM, and neutrophil count of 17.5 K/CMM. The patient remained in the hospital for 5 more days, during which time his pain levels fluctuated, requiring frequent adjustments to his pain management regimen. However, his breathing status remained normal, his cough did not change in characteristics, and he remained afebrile. On the final day of his hospitalization, he was weaned to oral pain medications of acetaminophen 325 mg-hydrocodone 10 mg p.o. every 8 h p.r.n. for pain and morphine immediate-release 15 mg p.o. every 4 h p.r.n. for severe pain, then was discharged on a prophylactic dose of low-molecular-weight heparin (enoxaparin 40 mg/0.4 mL subcutaneous) with instructions to return if the dyspnea or chest pain recurred.
CASE 5: 25-YEAR-OLD WOMAN WITH HBSS:
This is the case of a 25-year-old woman with HbSS disease who was seen via telemedicine by the hematology clinic to establish care. Her medical history was significant for an appendectomy, cholecystectomy in 2009, pain crises (with the most recent in December 2014), migraine headaches, and a benign cyst in the left breast. She had no history of stroke or ACS. Her current medications included hydroxyurea 1000 mg daily. During her clinical visit, she reported nasal congestion, loss of taste, intermittent frontal headache that started 3 to 4 days prior, and intermittent musculoskeletal pain, which she managed with over-the-counter analgesic medications. The patient denied having fever, cough, chills, diarrhea, chest pain, or SOB. A SARS-COV-2 RT-PCR test was ordered owing to symptoms aligning with the standard presentation of COVID-19, and the result was positive. No further progression of symptoms or new symptoms were reported at the 1-week or 3-week outpatient clinic follow-up visits.
Discussion
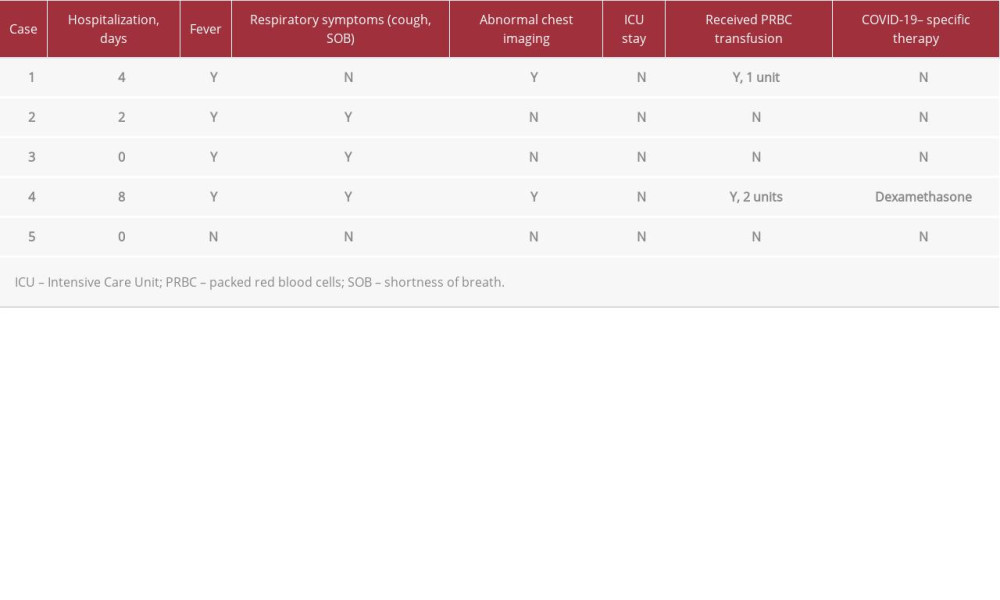
COVID-19 disproportionally causes severe complications in patients with SCD as well as in patients with diseases affecting respiratory function. As shown in the 5 cases presented here, the clinical presentation of COVID-19 in an SCD patient is not always the typical COVID-19 triad of cough, fever, and SOB that clinicians have been taught to recognize. The patients described in this series presented with symptoms ranging from fever, cough, and/or upper respiratory symptoms, which were able to be handled in an outpatient setting, to musculoskeletal pain and VOC, which required hospitalization (see Table 1). Recent case reports on patients with SCD have indicated that COVID-19 can trigger VOCs in patients with SCD due to COVID-19’s ability to increase inflammatory cytokines such as interleukin-6 (IL-6), which can induce VOCs in SCD patients with and without COVID-19 [4]. There have been recent studies on the use of drugs that target IL-6 receptors, such as such as tocilizumab, an IL-6 receptor blocker, in COVID-19 treatment [5]. One randomized study performed on patients with COVID-19 pneumonia not requiring mechanical ventilation showed that treatment with 8 mg/kg i.v. tocilizumab reduced the likelihood that these patients progressed to requiring mechanical ventilation or death [5]. However, the study did not show that tocilizumab improved survival in these patients [5]. Based on these findings and our knowledge of the likely involvement of IL-6 in the triggering of VOCs in SCD patients with COVID-19, it may be worth considering further research into the use of IL-6 blockers such as tocilizumab in the treatment of patients with SCD and COVID-19. COVID-19 has also been shown to induce endothelial and microvascular dysfunction through complement-mediated processes [6]. Activation of complement in the body, as is happening in COVID-19, increases the risk for SCD complications such as VOC and hemolysis [7]. For SCD patients and clinicians, this means that patients with SCD and COVID-19 can present with a VOC rather than typical COVID-19 symptoms, which was true for 4 out of 5 of the cases presented above.
Furthermore, as seen in this series, the findings on CT scan and chest X-ray for this subset of patients can also differ from the typical presentation of the COVID-19 radiologic findings. On CT scans, COVID-19 pulmonary involvement presents as bilateral and peripheral ground glass and consolidative pulmonary opacities [8]. In one of the present cases, a chest CT scan showed findings typical of SCD patients, which caused us to falsely dismiss the possibility of COVID-19 in this case. In another case, the chest X-ray showed both signs of COVID-19 and ACS. Therefore, it must be acknowledged that because the impact of COVID-19 on patients with SCD can be the induction of a VOC crisis rather than direct respiratory damage from the virus itself, CT scans and chest X-rays cannot be used alone to rule out COVID-19 in these patients.
It is also important to note that while our case series had a 60% hospitalization rate, 0% intensive care unit (ICU) admission rate, and 0% mortality rate, these outcomes are far better than those seen in larger SCD COVID-19 studies. A 178-patient study on COVID-19 in patients with SCD performed by the Medical College of Wisconsin demonstrated a 69% hospitalization rate, 11% ICU admission rate, and 7% mortality rate [9]. This mortality rate contrasts with that of the general United States population as reported by Johns Hopkins, which indicated a mortality rate of 1.8% [10]. This difference in hospitalization rate, ICU admission rate, and mortality between our study and the Medical College of Wisconsin study is likely due to the relative study sizes, and thus the Wisconsin study should be referred to as a better representation of these rates.
Based on the present cases, we also recommend that patients with SCD and COVID-19 who have hypoxia associated with abnormal radiographic findings on imaging studies should be treated early and similarly to patients with moderate to severe ACS, namely with a transfusion of packed RBCs. Moreover, if the patient develops severe respiratory dysfunction or respiratory failure, then an RBC exchange transfusion should be considered promptly. Packed RBC transfusion was used successfully in our case and in the case published by Hussain et al in the British Journal of Haematology [2].
We acknowledge that this case series was limited by the small number of patients, limited patient age range (23–49 years old), lack of chest CT imaging available for most of the patients, and limited long-term follow-up of the patients studied. We also did not examine the socioeconomic and social factors that led to differences in outcomes for these patients with SCD, a factor which has been seen to impact SCD severity and number of complications [11].
Conclusions
In conclusion, we recommend that all patients with SCD with a noted risk of SARS-COV-2 exposure or who present with worsening musculoskeletal pain or VOC, even in the absence of the typical clinical picture of COVID-19, be tested for SARSCOV-2. If this information had been known at the presentation of our first patient, SARS-COV-2 testing would have occurred on the day of presentation to the health care facility rather than upon discharge, thus preventing possible transmission of infection to clinical staff and other patients during the course of the patient’s hospitalization. Recognizing the different clinical scenarios of COVID-19 in patients with SCD is imperative for therapeutic measures to be initiated promptly. Individuals with SCD likely have preexisting multiorgan dys-function and delicate immune systems, which put them at an increased risk for COVID-19-related morbidity and mortality, especially when the infection is unrecognized and improperly treated. SCD impacts millions of people globally and over 100 000 people in the United States [12]. Despite its prevalence, until very recently, SCD was a vastly understudied disease [12]. Continued research on SCD and on its interaction with major infectious diseases and determinants of health is imperative to provide the best care and outcomes to those with SCD.
References:
1.. Beerkens F, John M, Puliafito B, COVID-19 pneumonia as a cause of acute chest syndrome in an adult sickle cell patient: Am J Hematol, 2020; 95(7); E154-56
2.. Hussain FA, Njoku FU, Saraf SL, COVID-19 infection in patients with sickle cell disease: Br J Haematol, 2020; 189(5); 851-52
3.. Mekontso Dessap A, Deux JF, Habibi A, Lung imaging during acute chest syndrome in sickle cell disease: Computed tomography patterns and diagnostic accuracy of bedside chest radiograph: Thorax, 2014; 69(2); 144-51
4.. Nur E, Gaartman AE, van Tuijn CFJ, Tang MW, Biemond BJ, Vaso-occlusive crisis and acute chest syndrome in sickle cell disease due to 2019 novel coronavirus disease (COVID-19): Am J Hematol, 2020; 95(6); 725-26
5.. Salama C, Han J, Yau L, Tocilizumab in patients hospitalized with COVID-19 pneumonia: New Engl J Med, 2021; 384; 20-30
6.. Kreuziger LB, Lee A, Garcia D, COVID-19 and VTE/anticoagulation: Frequently asked questions. American Society of Hematology: COVID-19 Resources [Accessed 18 December 2020] https://www.hematology.org/covid-19/covid-19-and-vte-anticoagulation
7.. Gavriilaki E, Brodsky RA, Severe COVID-19 infection and thrombotic micro-angiopathy: Success does not come easily: Br J Haematol, 2020; 189; e227-30
8.. Tampaki A, Gavriilaki E, Varelas C, Complement in sickle cell disease and targeted therapy: I know one thing, that I know nothing: Blood Rev, 2021 [Online ahead of prin]
9.. Panepinto JA, Brandow A, Mucalo L, coronavirus disease among persons with sickle cell disease, United States, March 20–May 21, 2020: Emerg Infect Dis, 2020; 26(10); 2473-76
10.. , Johns Hopkins Coronavirus Resource Center [cited 2021 February 27]; https://coronavirus.jhu.edu/data/mortality
11.. Okany CC, Akinyanju OO, The influence of socio-economic status on the severity of sickle cell disease: Afr J Med Sci, 1993; 22(2); 57-60
12.. Minniti CP, Zaidi AU, Nouraie M, Clinical predictors of poor outcomes in patients with sickle cell disease and COVID-19 infection: Blood Adv, 2021; 5(1); 207-15
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133