16 January 2022: Articles 
Giant Fibroepithelial Polyps of the Vulva in a Woman with Uterine Myoma and Primary Infertility: A Case Report and Literature Review
Rare disease
Eighty Mardiyan Kurniawati1ABC*, Fauzan Djunaidi1CDF, Nila Kurniasari2AFGDOI: 10.12659/AJCR.933198
Am J Case Rep 2022; 23:e933198






Abstract
BACKGROUND: Reproductive health is closely related to long-term quality of life and maternal well-being in obstetrics. The overall incidence of fibro-epithelial polyps in the general population is about 46%, but a location on the vulva is quite rare, and is very rare when the size is more than 5 cm.
CASE REPORT: A 23-year-old woman reported irregular bleeding and a mass on the vulva. After anamnesis, physical examination, biopsy, and radiology imaging, the patient was diagnosed with uterine myoma, primary infertility, and a large solid and benign mass on the vulva. The mass found on the vulva was apparently unrelated to intra-abdominal organs and urogynecology. After performing an excision accompanied by a laparoscopic myomectomy, the histopathological results showed that the mass on the vulva was a 16×11×6 cm fibroepithelial polyp weighing 700 g. After 7 months of therapy, the submucosal uterine myoma recurred. Submucosal uterine myomas were found rooted into the vaginal canal, so the surgeon performed an extirpation operation. Eight months later, the patient succeeded in having a pregnancy that ended in delivery by cesarean section.
CONCLUSIONS: Giant fibroepithelial polyps are very rare. Management is by excision accompanied by a laparoscopic myomectomy. They affect reproductive health and require appropriate management and diagnosis.
Keywords: Infertility, Myoma, Vulvar Diseases, Adult, Cesarean Section, Female, Humans, Neoplasm Recurrence, Local, Pregnancy, Quality of Life, Uterine Myomectomy, Uterine Neoplasms, Vulva, young adult
Background
Reproductive health is closely related to the quality of life of women and maternal health in obstetrics. Some of the diseases associated with the female reproductive organs are fibroepithelial polyps, uterine myoma, and infertility. Fibroepithelial polyp of the vulva is a very rare and benign disorder that generally occurs in young to middle-aged women [1]. Fibroepithelial polyps also vary in size. The literature contains a report of a 42-cm fibroepithelial polyp [2]. This disease is rare, because it has specific features and often overlaps with other diagnoses, because the stromal cells show a variety of immunophenotypes. This polyp is thought to have a relationship with hormonal problems, because the patient may be pregnant at diagnosis or have a history of hormonal therapy [1].
Uterine myomas are benign tumors that are most commonly found in the female reproductive system and are a major cause of decreased quality of life [3]. They can have a negative impact on the reproductive system and can be single, but more often are multiple, causing significant morbidity and decreased quality of life. Of all hysterectomies, 40–60% are performed due to myomas. Myomas consist mostly of smooth muscle cells and contain a number of distinct fibrous tissues. During growth, the myoma compresses the surrounding structures (myometrium and connective tissue), causing the progressive formation of a pseudocapsule-like, rich in collagen fibers, neurofibers, and blood vessels [4].
Infertility has become a public health problem in women of reproductive age, and worldwide it affects about 10%–15% of couples trying to achieve pregnancy. Several factors can interfere the fertility at any stage. For example, female infertility can have 1 or more reasons related to reproductive health and health in general, such as thyroid disorders and diabetes [5].
We report cases that are rare, complex and require long-term management and are associated with many factors. This case occurs in women who have 3 problems, namely therapy for polyps and myomas to treat infertility. Giant fibroepithelial polyps on the vulva case in Indonesia are quite rare. Journal of case reports at referral hospitals in 2010–2014 contains 9 cases, mostly 6 cases of childbearing age, 3 cases over 45 years of age and 2 cases growing during pregnancy. Not all case reports include immunohistochemical examinations [6].
Case Report
Our patient was a 23-year-old woman known to have primary infertility, who had been married for 18 months and was sexually active. She had not had a preconception check-up. The patient reported that there had been problems with reproductive health such as irregular bleeding about 1 year ago, but when she received treatment at the first facility she visited, she was reluctant to be referred to a larger facility, so the treatment stopped. The patient first came to the Urogynecology Polyclinic, a referral hospital in East Java, Indonesia and told the doctor that she had been having irregular menstrual bleeding for 3 months, bleeding for 20 days, and had a mass in the vulva. After anamnesis, physical examination, biopsy, and radiology imaging, the patient was found to have a benign solid mass on the vulva and had uterine myoma. She reported having disturbances in sexual activity due to menstrual disturbances and prolonged bleeding. The presence of the masses was not reported at first because she considered this situation to be normal and the masses were not large. The patient described having a mass in the vagina since adolescence (age 12 years) but this was ignored because it did not interfere with her daily activity. Figures 1 and 2 show the presence of polyps from the first presentation until after surgery. Figure 3 shows MRI pelvic results, with an intramural lobulated mass in the posterior body of the uterus measuring 8.3×6.47×6.94 cm; it could be a uterine myoma or a soft-tissue mass in the right vulva that is not related to the vaginal ureter and anus. The size is 9×10.4×9.2 cm, and the right and left ovaries appear normal.
Speculum examination showed a mass in the right major labium, +15 cm in diameter, solid, mobile, no tenderness, flux or fluorine albus. Abdomen enlarged 12/14 weeks, myoma features. From the results of blood tests, the patient was diagnosed with anemia with hemoglobin 3.9 g/dL. The results of the initial ultra-sound examination found a mass with a size of 12.4×5.67×6.65 cm, and the fine-needle aspiration biopsy (FNAB) results showed a benign mesenchymal spindle tumor (labium major D). The transvaginal ultrasonography (TVUS) results showed multiple myomas: (1) intramural myomas in the fundus measuring 3.8×3.8 cm and (2) intramural myomas in the fundus measuring 3.2×3.8 cm.
Within 2 weeks, the patient returned to normal. The results showed an increase in the size of the myoma. Prior to surgery, the patient experienced heavy vaginal bleeding and was in weak condition but was conscious. On genital examination, a mass was found in the right labia majora with a diameter of 15 cm; it was solid but mobile, and was closed and slippery. The results of the TVS ultrasound showed multiple myomas: (1) intramural myomas in the fundus measuring 40.8×45.6 mm, and (2) intramural myomas in the fundus measuring 36.9×46.9 mm. The laboratory results showed a hemoglobin level of 7.84 g/dL; therefore, 3 bags of PRC were given, after which the hemoglobin level increased to 10.3 g/dL. Analyses obtained prior to pro-laparoscopic myectomy showed uterine myoma with major labial tumor, anemia, and primary infertility. In the interval examination it was found that there was an increase in size at follow-up 2 weeks later, but these results did not show how much the myoma grew every day.
After performing an excision operation accompanied by laparoscopic myomectomy, the histopathological results showed that the mass on the vulva was a fibroepithelial polyp, and there was uterine myoma in the uterus. The mass of the vaginal tumor in the left major labium was 15×10 cm, 2 submucosal uterine myomas, each measuring 3×4 cm and 1×2 cm, performed myomectomy and myoma mass was removed with a morcellator.
After the operation, the patient was in stable condition. The patient was discharged with the wound treated and without any complaints. In the second control period, 2 weeks after the patient’s surgery, the patient experienced a surgical wound that was still wet. The patient was advised to consume foods containing high protein. On day 20, the stitches had dried and the patient was directed to a fertility clinic. The results of the microscopic and macroscopic anatomical pathology showed the existence of a uterine leiomyoma, requiring major labium surgery with fibroepithelial polyp surgery. Initially it was suspected that this polyp was associated with uterine myoma (hormonal), but the results of immunohistochemical examination showed that the results of immunohistochemistry of estrogen receptors (ER) and progesterone receptors (PR) were negative, and the results of desmin and SMA were also negative and varied. Figure 4 shows the anatomical histopathology of uterine myoma. Figure 5 shows anatomical histopathology of fibroepithelial polyps. The results of estrogen receptors and progesterone receptors are shown in Figures 6 and 7. The results of SMA and desmin are shown in Figures 8 and 9. Figure 4 shows the anatomical histopathology of uterine myoma with sections of tumor growth tissue, consisting of proliferating smooth muscle cells, arranged in bundles that intersect at right angles to each other, with no signs of trauma. Based on Figure 5, the anatomical histo-pathology of fibroepithelial polyps shows a section of benign mesenchymal tissue covered with skin, consisting of a proliferation of spindle-nucleated cells, monotonous, and fine chromatin, loosely arranged between the myxoid stroma. In other areas, cells with flat nuclei are seen, pushed to the edge, with clear wide cytoplasm, and mitosis 0/50 HPF. Figure 6 shows ER immunohistochemistry and Figure 7 shows immunohisto-chemistry PR for fibroepithelial polyps, with negative ER results (positive control) and the PR results are negative (positive control). Based on Figure 8, the negative SMA immunohisto-chemistry for fibroepithelial polyps showed that the results of the block originating from myoma supported a tumor originating from smooth muscle, and the block from the labia major tumor was found to support a tumor originating from non-smooth muscle according to the fibroepithelial polyp. Based on Figure 9, immunohistochemistry was desmin-negative on the fibroepithelial polyp, indicating that the tumor is not derived from muscle cells.
After 7 months, a recurrence of submucosal uterine myomas was found with initial complaints of profuse vaginal bleeding and weakness. A speculum examination showed a mass in the vagina, with an impression of uterine myoma, size 5×6 cm, and a stem length 3-4 cm. The analysis showed a Geburt uterine myoma. The patient underwent extirpation surgery and curettage of endometrial anatomical pathology to resolve the Geburt uterine myoma. During the operation, a 5-cm Geburt uterine myoma was found and destroyed, followed by curettage.
After 1.5 years since the first operation (8 months since the second operation), the patient became pregnant. The pregnancy was planned to end with a primary cesarean section at 39/40 weeks’ gestation. But ultimately, the patient underwent immediate cesarean section due to oligohydramnios, history of myomectomy (sub mucosal myoma) in the fundus region, and history of primary infertility. From the evaluation during surgery, there was a skin incision in the midline, no adhesions were found, and a male baby was born at 21: 23, weighing 3700 g, 56 cm long. The placenta was expelled with light traction and IUD insertion is done. When evaluating the uterus, a submucosal myoma was found, above +2–3 cm from the incision of the lower uterine segment, +2 cm in diameter, not very prominent. There was also a laparoscopic myomectomy scar from 2 years ago, which was still intact and smooth. After delivery, the patient was in good condition. After the puerperium, there was no problem in the menstrual cycle and the duration of menstruation was 5–7 days. In addition, the patient did not complain of a lump anymore.
Discussion
The case took a lot of time in planning a pregnancy and overcoming women’s reproductive health problems. This case takes time due to the lack of awareness of women at the beginning about their reproductive health needs, so many delay the examination procedure even though the symptoms are still early. In addition, there was an error in the initial interpretation of the symptoms, causing the case to not receive the appropriate diagnosis and treatment. Future therapy and results need to be considered. This patient presented with an initial main concern of profuse and prolonged vaginal bleeding (+20 days), related to other reproductive diseases. This case was complicated by the fact that vulvar polyps are rare and the patient felt embarrassed and was reluctant to be examined. Patients will have themselves checked out if there are concerns of pain, wounds/ulcers, pain during intercourse, or difficulty walking, which interfere with activities [7,8].
Our patient had fibroepithelial polyps of the vulva, uterine myoma, and infertility, as well as anemia, requiring several transfusions. In about 30% of cases of uterine myoma, the presence of these tumors causes morbidity due to abnormal uterine bleeding (heavy menstrual bleeding causes anemia) and pelvic pressure (urinary symptoms, constipation, and tenesmus) [9].
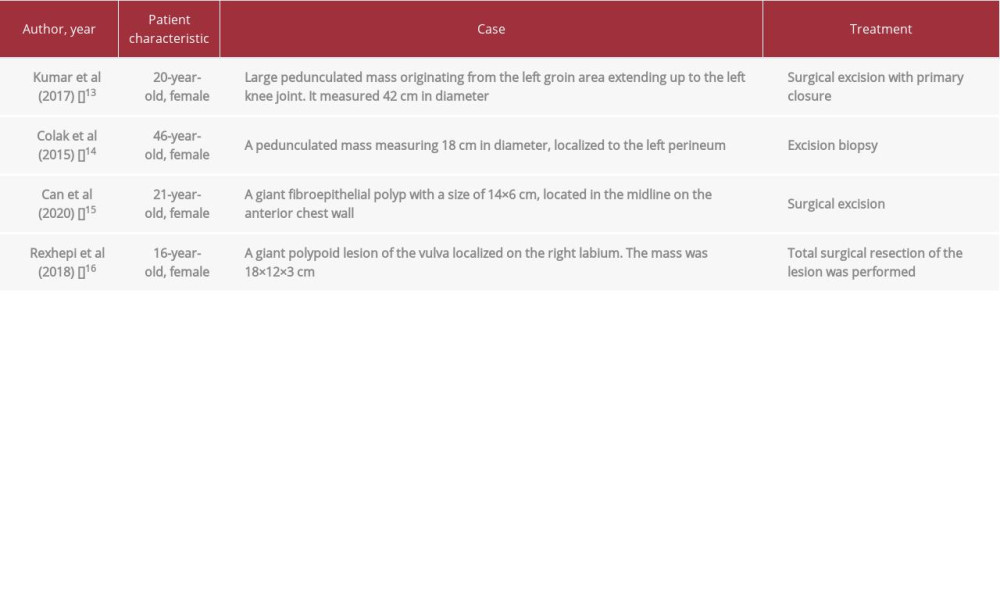
This patient had a fibroepithelial polyp occurring on the vulva. Fibroepithelial polyp (FEP) of the vulva is a very rare and benign disorder that generally occurs in young to middle-aged women. Fibroepithelial polyps growing large in the vulvar area are rare benign tumors that can be misinterpreted as malignant because of their various morphological appearances [10]. The pathophysiology is unclear, and appears to have a hormonal relationship, as patients may be pregnant at diagnosis or have a history of hormonal therapy [11]. There may be a hormone-sensitive epithelial structure, and their incidence increases in women of reproductive age. In the present case, the patient was not taking hormone therapy in an effort to improve the menstrual cycle or family planning program. Fibroepithelial polyps are usually asymptomatic, and are therefore discovered incidentally during routine gynecological examinations, or are reported by patients because of their appearance. When symptomatic, bleeding is a very common presentation, as reported, for example, by the patient in this case report. When ulceration occurs, inflammation secondary to infection may occur [12]. The results of this study are in line with the patient’s reported condition. Table 1 shows the case data for the previous giant fibroepithelial polyp. From various references, it is known that giant fibroepithelial polyps can reach various ages.
In this case the patient underwent a laparoscopic myomectomy. The best option in the management of gynecological cases is myomectomy to increase the chances of conception/ pregnancy [17]. However, after a laparoscopic myomectomy was performed, this patient had a Geburt myoma. This Geburt myoma is a type of myoma that is known after laparoscopic myomectomy because of the presence of a stalk. In the first operation, uterine myoma was found and not Geburt myoma. Prior to the discovery of Geburt myoma, these myomas were simply described as uterine myomas. Geburt myoma, also known as pedunculated submucosal myoma, is a type of submucosal myoma that has a stalk. These tumors can come out of the uterine cavity into the vagina, known as fibroid fibroids or myomas, which are prone to infection, injury, and infarction. Geburt fibroids are submucosal myomas that can grow stems into polyps and then exit through the cervix. The incidence rate of submucosal myoma is about 20–40%, and this disease often occurs in women aged 30–50 years. This incident was associated with uterine leiomyoma patients [18]. Uterine leiomyomas are the most common pelvic tumors in women arising from the smooth muscle of the myometrium. Leiomyomas are classified according to their location within the myometrium. Prolapsed pedunculated submucosal myomas are classified as type 0 submucosal leiomyomas [19].
Uterine myoma recurrence ranges from 15% to 51% [10,11]. After undergoing treatment related to uterine myoma and polyps, the patient was declared pregnant. Pregnancy rates range from 50% to 60% after myomectomy using both laparoscopic and laparotomy approaches. Patients undergo intensive care during pregnancy, although after myomectomy, the risk of uterine rupture during pregnancy is quite low, about 0.002% [9], while other studies report a range of 0.5–1% [1].
The patient finally underwent a cesarean section. Patients who have a history of either laparotomy or laparoscopic intramural uterine myoma incision, especially if the myoma is large and the incision is deep, pregnancy should generally be terminated by cesarean delivery [10]. The patient immediately underwent cesarean section considering oligohydramnios, history of myomectomy (sub mucosal myoma) in the fundus region, history of primary infertility. The relationship between giant vulvar polyps and uterine myoma on this one occasion is still not understood. Despite the fact that the pathophysiology of polyp growth is unclear [12,13] ER and PR result in these tumors also negative, meaning that their growth may not be hormonal [20].
Uterine myoma recurrence in the study was associated with open myomectomy (OM) and laparoscopic myomectomy (LM). The cumulative recurrence rate between the 2 groups was 76.2% (LM) vs 63.4% (OM) at 8 years postoperatively. The results of statistical tests also showed that LM resulted in a higher recurrence rate than OM, possibly due to manual myoma removal in OM, which is a more complete extraction of a smaller myoma mass than that performed in LM [21]. Special attention to recurrence is required for patients with uterine myomas with a diameter of 10 cm, with multiple myomas, and those aged 35 years or older [22]. Patients with multiple uterine leiomyomas and those in the third decade of life should be thoroughly counseled about the risk of recurrence prior to laparoscopic myomectomy [23].
Conclusions
Giant fibroepithelial polyps are very rare. Management is carried out by an excision operation accompanied by a laparoscopic myomectomy. They affect reproductive health and require appropriate management and diagnosis. In the present case of a woman with fibroepithelial polyps of the vulva, uterine myoma, and primary infertility, the procedure carried out by the team was successful and the patient was able to become pregnant and overcome her reproductive health problems. Management of women with fibroepithelial polyps of the vulva, uterine myoma and primary infertility is time-consuming because it depends on the patient’s own awareness of their reproductive health needs, attention to relapsed disease, an accurate diagnosis process, and cooperation in the hospital. In addition, patients must be willing to understand themselves so that there is no delay in diagnosis and management. The factors causing this giant vulva are unclear because the results of laboratory tests found no hormonal indication.
Figures
References:
1.. Lee HJ, Norwitz ER, Shaw J, Contemporary management of fibroids in pregnancy-management update: Rev Obstet Gynecol, 2010; 3(1); 20-27
2.. Can B, Ozluk AY, Giant fibroepithelial polyps: Why do they grow excessively?: Sisli Etfal Hastan Tip Bul, 2020; 54(2); 257-60
3.. Mutiara A, Sharon G, Mulyanusa A, Three years data of uterine fibroids patient characteristics at West Java top referral hospital: Althea Medical Journal, 2017; 4(3); 382-88
4.. Sparic R, Mirkovic L, Malvasi A, Tinelli A, Epidemiology of uterine myomas: A review: Int J Fertil Steril, 2016; 9(4); 424-35
5.. Benksim A, Elkhoudri N, Addi RA, Difference between primary and secondary infertility in Morocco: Frequencies and associated factors: Int J Fertil Steril, 2018; 12(2); 142-46
6.. , Soetomo (Indonesia): Medical Records 2010–2015, 2015, Surabaya, RSUD Dr. Soetomo
7.. Najam RH, Chowdhury H, Awasthi S, A large fibroma polyp of labia majora: J Clin Case Rep, 2013; 3; 297
8.. Armo M, Agrawal S, Minj M, Kavita B, Recurrent vulval fibroepithelial polyp with pregnancy: A rare presentation: Int J Reprod Contracep Obstet Gynecol, 2013; 2(2); 245-47
9.. Jacques D, Marie MD, Uterine fibroid management: From the present to the future: Hum Rep Upd, 2016; 22(6); 665-86
10.. Navada MH, Bhat PR, Rao SV, Large fibroepithelial polyp of vulva: Case Rep Dermatol Med, 2011; 2011; 273181
11.. Lee MH, Hwang JY, Lee JH, Fibroepithelial polyp of the vulva accompanied by lymphangioma circumscriptum: Obstet Gynecol Sci, 2017; 60(4); 401-4
12.. Avila J, Nicol K, Hewitt GD, Matson SC, Vulvar fibroepithelial polyps in a female adolescent: A case report: J Pediat Adolesc Gynecol, 2017; 30(5); 595-97
13.. Kumar A, Hasin N, Sinha AK, Giant fibro epithelial polyp in a young girl: A rare case report: Int J Surg Case Rep, 2017; 38; 83-85
14.. Colak E, Ikinci A, Kucuk GO, Giant fibroepithelial polyp of the perineum: Giant fibroepithelial polyp: Int J Surg Case Rep, 2015; 17; 126-27
15.. Can B, Ozluk AY, Giant fibroepithelial polyps: why do they grow excessively?: Sisli Etfal Hastan Tip Bul, 2020; 54(2); 257-60
16.. Rexhepi M, Trajkovska E, Besimi F, Rufati N, Giant fibroepithelial polyp of vulva: A case report and review of literature: Pril (Makedon Akad Nauk Umet Odd Med Nauki), 2018; 39(2–3); 127-30
17.. Guo XC, Segars JH, The impact and management of fibroids for fertility: An evidence-based approach: Obstet Gynecol Clin North Am, 2012; 39(4); 521-33
18.. Yen LL, Yu LC, Chi AC, Wen FC, Torsion of pedunculated subserous uterine leiomyoma: A rare complication of a common disease: Taiwan J Obstet Gynecol, 2018; 57(2); 300-3
19.. Aydın S, Göksever ÇH, Maraşlı M, Bakar RZ, Clinical predictors of successful vaginal myomectomy for prolapsed pedunculated uterine leiomyoma: J Turk Ger Gynecol Assoc, 2018; 19(3); 146-50
20.. Lianos CA, Rosenberg AE, Fibrous myofibroblastic proliferations of the vulva: Vulvar Pathology, 2013, New York, Springer-Verlag
21.. Kotani Y, Tobiume T, Fujishima R, Recurrence of uterine myoma after myomectomy: Open myomectomy versus laparoscopic myomectomy: J Obstet Gynaecol Res, 2018; 44(2); 298-302
22.. Mitsuru S, Yasushi K, Masahiko U, Recurrence of uterine myoma after laparoscopic myomectomy: What are the risk factors?: Gynecol Minim Invasive Ther, 2012; 1(1); 34-36
23.. Radosa MP, Owsianowski Z, Mothes A, Long-term risk of fibroid recurrence after laparoscopic myomectomy: Eur J Obstet Gynecol Reprod Biol, 2014; 180(35); 9
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,422
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133