05 November 2021: Articles 
Posterior Reversible Encephalopathy Syndrome Presenting Atypically as a Non-Convulsive Seizure
Unusual clinical course, Challenging differential diagnosis, Diagnostic / therapeutic accidents
Adebola Oluwabusayo Adetiloye1EF*, Julio Valencia ManriqueDOI: 10.12659/AJCR.933667
Am J Case Rep 2021; 22:e933667






Abstract
BACKGROUND: Posterior reversible encephalopathy syndrome (PRES), also known as reversible posterior leukoencephalopathy, is a neurotoxic state with multiple etiologies characterized by altered mental state, headaches, visual abnormalities, and seizures. This clinico-radiological syndrome is rare, and a high index of suspicion is needed to diagnose, provide adequate treatment, and prevent irreversible neurological sequelae.
CASE REPORT: We present a case of a woman with end-stage renal disease (ESRD) who presented with acute confusion and non-convulsive seizures and was later diagnosed with PRES. In this case, altered mental status was initially thought to be secondary to uremic encephalopathy. A diagnosis of PRES was subsequently made after she had several sessions of HD without significant improvement in her mental state, prompting magnetic resonant imaging (MRI) for further evaluation. Specific risk factors for PRES, including blood pressure fluctuations, were targeted and she made significant clinical recovery but had residual functional impairment.
CONCLUSIONS: This case underscores the need for a high index of suspicion, especially in cases with atypical presentation, as delayed diagnosis can lead to suboptimal outcomes.
Keywords: Hypertension, Posterior Leukoencephalopathy Syndrome, Seizures, Diagnostic Imaging, Female, Headache, Humans, Magnetic Resonance Imaging, Risk Factors
Background
Posterior reversible encephalopathy syndrome (PRES) was first described in 1966 in a group of 15 patients with renal insufficiency, hypertension. and immunosuppression [1]. In these patients, a constellation of symptoms, including headache, decreased level of consciousness, visual changes, and seizures, associated with characteristic neuroimaging findings of posterior cerebral white-matter edema, was observed [1]. PRES has since been described in a number of clinical conditions with different pathophysiology. The exact cause and incidence of PRES is unknown, but an altered blood-brain barrier as a result of elevated blood pressure (BP) and/or endothelial injury seems to be a common denominator [2]. The clinical presentation of PRES is nonspecific and there is no well-defined diagnostic criteria, making for broad differentials; therefore, clinical suspicion needs to be high to ensure proper diagnosis and adequate management [3]. Although generalized tonic clonic seizure is the most commonly reported seizure type, a few cases, as well as the index case, had non-convulsive status epilepticus as a presenting symptom, which can manifest as confusion or psychotic symptoms [4,5].
Case Report
A 59-year-old African American woman with a known history of hypertension, hyperlipidemia, type 2 diabetes mellitus, and end-stage renal disease secondary to diabetes mellitus nephropathy was admitted to our hospital for altered mental status of 8-h duration prior to her presentation in the Emergency Department. Her daughter reported bizarre behavior, which included slow irrational speech with delusions and abnormal movements. She also stated that her mother was more somnolent than usual and had been experiencing headaches and worsening dyspnea for a few days prior to admission. She was scheduled for dialysis at an outside facility on the day of presentation, but the procedure was put on hold due to her altered mental status, agitation, and automatisms in the form of hand, head, and orofacial movements. Her home medications included amlodipine, carvedilol, lisinopril, hydralazine, isosorbide dinitrite, insulin, and methadone, but the daughter could not ascertain if she was complaint with her medications.
At presentation, she was hypertensive (BP 160/63 mmHg). No other abnormalities were noted in the vital signs. On neurological examination, she appeared restless, with stereotypical movement of head turning from side to side, eyes closed, with episodes of staring and nonsensical involuntary movements. She was oriented to person infrequently but not to time or place. She could not follow commands and responded to questions inappropriately, mostly with incomprehensible sounds. Her Glasgow Coma Scale (GCS) was 8/15: eye opening (E) 2, verbal response (V) 2, motor response (M) 4. She had no focal weakness, facial droop, or signs of meningeal irritation. A chest examination revealed bibasilar rales. The initial assessment was altered mental status secondary to metabolic verses toxic encephalopathy. A computed tomography (CT) scan of the head was unremarkable (Figure 1). A chest X-ray showed cardiomegaly and bilateral infiltrates suspicious for pulmonary edema. The toxicology screen from urine did not reveal any evidence of illicit drug use, and her blood ethanol level was <10 mg/dl. A comprehensive metabolic panel revealed sodium 145 mEq/L (136–145 mEq/L), potassium 5.1 mEq/L (3.5–5.1 mEq/L), chloride 102 mEq/L (98–107 mEq/L), bicarbonate 21 mmol/l (22–29 mmol/L), glucose 197 mg/dl (74–109 mg/dl), alkaline phosphatase 102 U/L (35–104 U/L), alanine aminotransferase 76 U/L (0–31 U/L), aspartate aminotransferase 43 mg/dl (0–32 U/L), calcium 9.8 mg/dl (8.6–10 mg/dl), and magnesium 2.3 mg/dl (1.4–2.6 mg/dl). Serum blood urea nitrogen (BUN) and creatinine levels were elevated at 45 mg/dl (6–20 mg/dl) and 8.2 mg/dl (0.7–0.9mg/dl), respectively. A complete blood count revealed white counts of 7800 cell/mcl (4300–11 000 cells/mcl), hemoglobin 12.7 g/dl (12–16 g/dl), platelets 123 000 cells/mcl (150 000–450 000 cells/mcl). Acute-phase reactants were elevated with C-reactive protein 4.99 mg/dl (0–0.4 mg/dl), and ferritin 1581 ng/ml (15–150 ng/ml) but antinuclear antibody (ANA) and other markers of autoimmune disease such as anti-double stranded DNA, antineutrophil cytoplasmic antibody (ANCA), and rheumatoid factor (RF) were unremarkable. Troponin and pro-brain natriuretic peptide were mildly elevated, while electrocardiography showed normal sinus rhythm with occasional premature ventricular complexes.
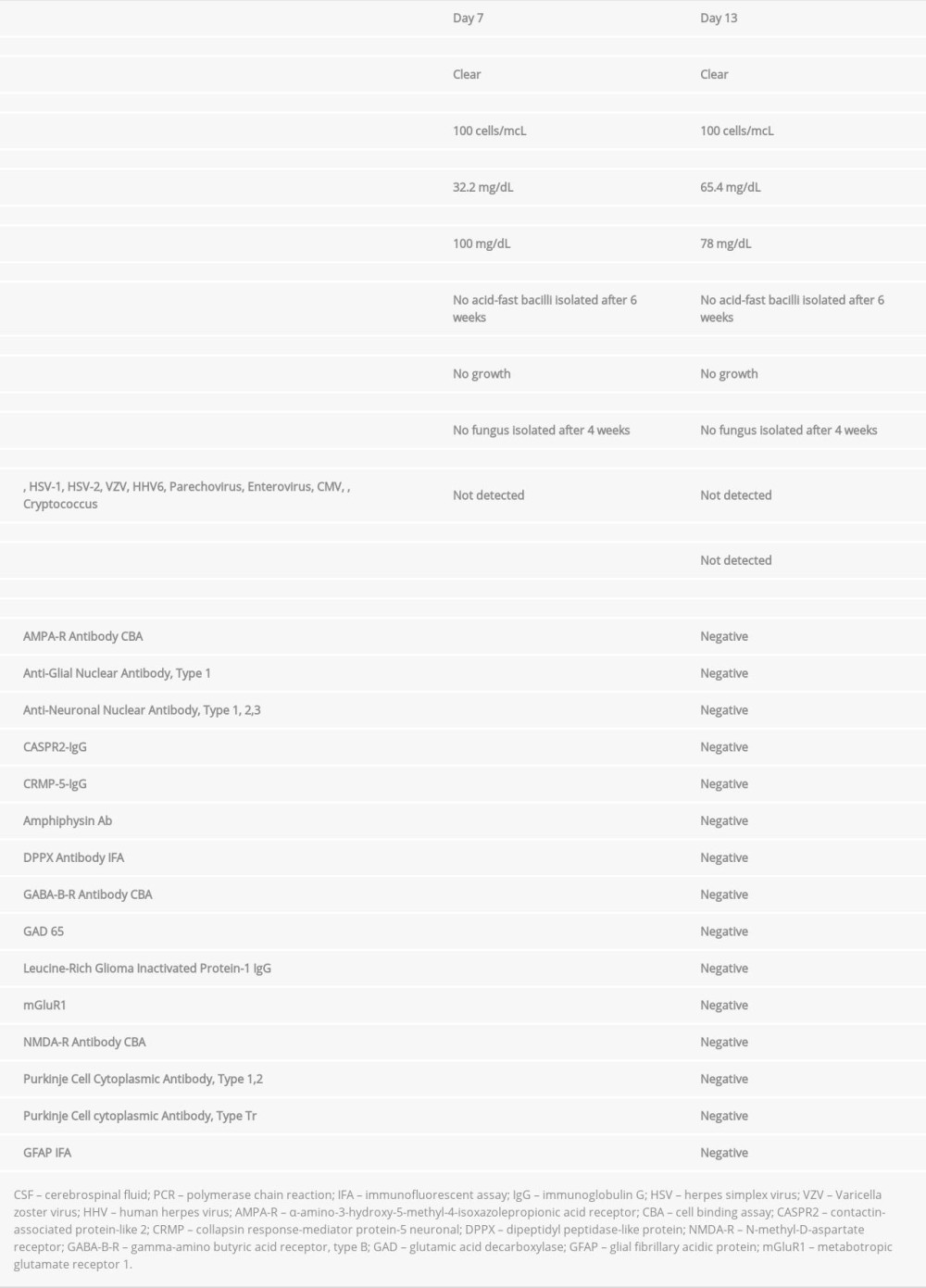
On the second day of admission, the patient was still confused, not obeying commands, and had no purposeful movements, GCS 7/15 15 with eye opening (E) 1, verbal response (V) 2, and motor response (M) 4, and BP ranged from 190–210 to 70–100 mmHg. She also had episodes of severe agitation. Serum BUN and creatinine trended up to 70 mg/dl and 11.0 mg/dl, respectively. A nasogastric tube (NGT) was placed for feeding and medications. She was started on hydralazine and labetalol via NGT and labetalol intravenously as needed to lower the BP to below 150/90 mmHg. The Nephrology Unit was consulted, and she had a session of hemodialysis on day 2 of admission. From day 3 to 10, she received 3 sessions of hemodialysis, but she continued to be in a fluctuating altered mental state. BUN during this period ranged from 17 mg/dl to 63 mg/dL (Table 1). Cardiology was consulted and recommended adding clonidine via NGT to the current antihypertensive regimen; however, BP ranged from 160–210 to 65–120 mmHg, with episodes of hypotension, necessitating withholding antihypertensive medications. A repeat CT scan of the brain on day 7 was unremarkable (Figure 2). Cerebral spinal fluid (CSF) studies showed mildly elevated white counts, mildly elevated protein, and negative oligoclonal band (Table 2). Electroencephalography (EEG) on day 10 showed severe diffuse cerebral dysfunction with frequent to continuous medium-to-high-voltage sharp and slow wave epileptiform discharges, synchronous and asynchronous, with amplitude predominance mainly in the frontal, central parietal, and occipital regions, consistent with epileptic encephalopathy (Figure 3). Based on EEG findings, we commenced intravenous levetiracetam 1 g loading dose, followed by 250 mg twice daily and 250 mg after each section of hemodialysis for maintenance. On day 11, the patient became more alert and oriented, she started following verbal commands, and her GCS improved from 8/15 to 13/15.
However, on day 13, she became lethargic and febrile without an apparent source of infection. Vitals revealed BP of 188/110 mmHg. She had with elevated white counts of 25 000 cells/mcL and neutrophilia. A repeat chest X-ray showed atelectatic changes, but repeat CSF cell count, protein, and glucose contents were not unremarkably different from the prior study (Table 2). Blood, urine, and CSF cultures, CSF viral panel polymerase chain reaction (PCR), and CSF encephalopathy markers were obtained (Table 2). She was transferred to the Intensive Care Unit due to her deteriorating mental status. Intravenous meropenem 1 g every 24 h and acyclovir 220 mg daily (doses adjusted for renal impairment) were commenced pending culture reports. A repeat EEG showed diffuse encephalopathy. At this time, which was day 15 of admission, magnetic resonance imaging (MRI) of the brain was performed, revealing findings in keeping with PRES (Figure 4A ,4B). Over the next few days, she was on continuous cardiopulmonary monitoring and received labetalol by continuous infusion titrated to achieve better BP control with a goal of BP less than 150/90 mmHg and to avoid fluctuations in BP (Figure 5). A repeat CSF viral panel PCR and autoimmune encephalopathy markers came back negative (Table 2); therefore, acyclovir was discontinued but i.v. meropenem was continued for 7 days to treat sepsis. Cultures (CSF, blood, urine) also came back negative, with resolution of leukocytosis in the next 3 days. By day 20, the patient was completely alert and oriented, obeying commands, with GCS of 15/15 and steady blood pressure readings below 150/80. She continued to have regular hemo-dialysis sessions and was started on an outpatient antihypertensive regimen. She was also counseled on the importance of adherence to antihypertensive medications and hemodialysis. A repeat MRI on day 20 of admission showed increased late subacute hemorrhage associated with PRES and areas of developing encephalomalacia (Figure 6). She was subsequently discharged to a subacute rehabilitation facility with a modified Rankin scale of 4. She was followed up by a neurologist 2 months after discharge, with a repeat MRI revealing residual brain abnormalities. As result of persistent neuroimaging abnormalities, patient was maintained on long-term oral levetiracetam to prevent recurrent seizures.
Discussion
The precise incidence of PRES is unknown, but with increasing awareness of its possibility as a differential in various clinical scenarios coupled with more widespread use of MRI, more cases are being reported. In our patient, we hypothesized that elevated blood pressure as well as blood pressure fluctuation in the setting of kidney disease was the major factor predis-posing to the development of PRES. The pathophysiology of PRES is not well understood, but appears to be related to loss of cerebral autoregulation and endothelial dysfunction [1,6].
Hypertension with autoregulatory failure is believed to play a pivotal role in PRES. Normal autoregulation maintains constant cerebral blood flow over a range of systemic BP by means of arteriolar constriction and dilatation, as needed. Loss of auto-regulation occurs at MAP of >150–160 mmHg. In chronic hypertension, it occurs at relatively higher pressures, leading to breakdown of the blood-brain barrier and extravasation of fluid and blood products to brain parenchyma, causing vasogenic edema [7,8]. In addition, the speed of rise of blood pressure or random fluctuations in blood pressure suggests a higher risk of PRES compared to elevated blood pressure itself [6].
Endothelial dysfunction also plays a crucial role in PRES patho-physiology, which could explain the occurrence of PRES in normotensive individuals. Diseases associated with activation of immune system or production of vasotoxic products can lead to abnormal endothelial activation, which in turn leads to production of molecules that triggers cytotoxic edema [9,10].
PRES has been described in series of patients with acute and chronic kidney disease, as well as in those with ESRD. This suggests that abnormal kidney function is an important cause of PRES [11,12]. The association of kidney disease with PRES could be attributed to elevated blood pressure with kidney dysfunction, as well as endothelial dysfunction [9]. Autoimmune disorders such as systemic lupus erythematosus, granulomatosis with polyangiitis, rheumatoid arthritis, and Sjögren syndrome are also present in up to half of patients with PRES [1,8,13]. Some of these diseases have kidney dysfunction as a comorbidity. In addition, some of the medications used in the treatment of autoimmune diseases with kidney involvement, such as cyclosporin and tacrolimus, have been known to induce PRES [14]. Fluid overload in the setting of kidney dysfunction can also contribute to the development of PRES [3].
There are no validated diagnostic criteria for PRES, and its clinical presentation is not unique to the disease, making early diagnosis challenging, especially in patients with atypical presentation. The diagnosis of PRES should always be considered among the differentials in patients with risk factors such as ESRD or hypertension in the setting of acute neurological symptoms with typical neuroimaging findings, especially when unexplained by common etiologies. In our patient, we entertained possible diagnoses of metabolic encephalopathy, toxic encephalopathy, meningoencephalitis, and severe sepsis. However, CSF analysis results were not indicative of central nervous system infection or autoimmune limbic encephalitis. In addition, the toxicology screen was negative, and our patient did not have remarkable electrolyte derangement like hypomagnesemia, which is a documented risk factor for PRES. She continued regular sessions of hemodialysis, ruling out uremic encephalopathy as a cause of her altered mental status. Although our patient developed fever and leukocytosis during the course of hospitalization, raising the suspicion for sepsis, cultures came back negative. However, she was treated for sepsis with unclear etiology with resolution of fever and normalization of white blood cell counts. Moreover, reports have suggested that septic encephalopathy requires the absence of CNS infection, absence of other potential cause of encephalopathy, and nonspecific findings on neuroimaging [15]. Sepsis also a potential cause of PRES, which could have contributed to the severity of PRES in the index case [16].
In most reports, generalized tonic clonic seizure is the most common seizure type in patients with PRES. Nonetheless, the prevalence and clinical significance of non-convulsive seizures is unknown in these patients. Such an atypical presentation can delay the diagnosis of PRES, as seen in our case, leading to poorer outcomes. A high prevalence of non-convulsive seizures was found in critically ill patients with PRES, and an association was found between restricted diffusion on MRI and worse outcome [17]. Moreover, psychosis as a presentation of PRES, as in our patient, is rare and only a few cases of such unusual presentation have been reported in the literature [18].
It is important to note that the syndrome is not always reversible, and it is often not confined to either the white matter or the posterior regions of the brain. Vasogenic edema mostly occurs in the parieto-occipital region, but lesions affecting ‘atypical’ regions such as the frontal lobe, cerebellum, or basal ganglia have also been reported [19]. In the index case, lesions were present in the fronto-parietal regions of the brain in addition to the parieto-occipital regions. A study of 76 patient with PRES reported frontal lobe involvement in almost 80% of patents [20]. Management instituted early has been shown to prevent unfavorable outcomes.
Treatment often involves use of antihypertensive medications to maintain BP in the autoregulatory range and withdrawal or treatment of other precipitating factors [1]. In a report of 15 patient with PRES, 100% of the patients had resolution of neurologic deficits within 2 weeks after timely institution of appropriate management [1]. However, in severe PRES, increased morbidity and mortality has been associated with delayed treatment, preexisting diabetes mellitus, and patients requiring dialysis. Complications include acute hemorrhage, extensive edema, and persistence of MRI abnormalities [6,21,22]. A study of 188 patients with PRES suggested that CSF pleocytosis was associated with cerebral hemorrhage, while elevated CSF protein was corrected with radiographic severity, similar to what was observed in the index case [23]. In our patient, the atypical PRES presentation contributed to delayed diagnosis; however, once PRES was diagnosed, we optimized blood pressure management and treated possible concurrent risk factors such as sepsis and fluid overload, with resolution of fluctuating levels of consciousness.
Conclusions
PRES is an uncommon non-inflammatory vasculopathy, which is not always as reversible as its name suggests. As there is no specific treatment of PRES, the management goal is to control the precipitating factors. Our case underscores the need for a high index of suspicion, timely diagnosis, and management of risk factors to avoid permanent neurological sequelae.
Figures

References:
1.. Hinchey J, Chaves C, Appignani B, A reversible posterior leukoencephalopathy syndrome: N Engl J Med, 1996; 334; 494-500
2.. Bartynski WS, Posterior reversible encephalopathy syndrome, Part 2: Controversies surrounding pathophysiology of vasogenic edema: Am J Neuroradiol, 2008; 29; 1043-49
3.. Sudulagunta SR, Sodalagunta MB, Kumbhat M, Nataraju AS, Posterior reversible encephalopathy syndrome (PRES): Oxford Med Case Reports, 2017; 2017; 43-46
4.. Kozak OS, Wijdicks EFM, Manno EM, Status epilepticus as initial manifestation of posterior reversible encephalopathy syndrome: Neurology, 2007; 69; 894-97
5.. Díaz-Ramírez GS, Salgado-Cifuentes CA, Zúñiga-Escobar G, Morales-Plaza CD, Posterior reversible leukoencephalopathy syndrome associated with psychosis: An unusual presentation: Neurol (Engl Ed), 2019; 34; 549-51
6.. Fugate JE, Rabinstein AA, Posterior reversible encephalopathy syndrome: Clinical and radiological manifestations, pathophysiology, and outstanding questions: Lancet Neurol, 2015; 14; 914-25
7.. Ruland S, Aiyagari V, Cerebral autoregulation and blood pressure lowering: Hypertension, 2007; 49; 977-78
8.. Fischer M, Schmutzhard E, Posterior reversible encephalopathy syndrome: J Neurol, 2017; 264; 1608-16
9.. Marra A, Vargas M, Striano P, Posterior reversible encephalopathy syndrome: The endothelial hypotheses: Med Hypotheses, 2014; 82; 619-22
10.. Chen Z, Shen GQ, Lerner A, Gao B, Immune system activation in the pathogenesis of posterior reversible encephalopathy syndrome: Brain Res Bull, 2017; 131; 93-99
11.. Gavrilovici C, Miron I, Voroneanu L, Bădărau S, Stârcea M, Posterior reversible encephalopathy syndrome in children with kidney disease: Int Urol Nephrol, 2017; 49; 1793-800
12.. Fugate JE, Rabinstein AA, Posterior reversible encephalopathy syndrome: Clinical and radiological manifestations, pathophysiology, and outstanding questions: Lancet Neurol, 2015; 14; 914-25
13.. Gatla N, Annapureddy N, Sequeira W, Jolly M, Posterior reversible encephalopathy syndrome in systemic lupus erythematosus: J Clin Rheumatol, 2013; 19; 334-40
14.. Tam CS, Galanos J, Seymour JF, Reversible posterior leukoencephalopathy syndrome complicating cytotoxic chemotherapy for hematologic malignancies: Am J Hematol, 2004; 77; 72-76
15.. Gofton TE, Young GB, Sepsis-associated encephalopathy: Nat Rev Neurol, 2012; 8; 557-66
16.. Garner O, Ramirez A, Lardino A, A case of posterior reversible encephalopathy syndrome associated with sepsis: BMJ Case Rep, 2018; 2018; bcr2018225128
17.. Bastide L, Legros B, Rampal N, Clinical correlates of periodic discharges and nonconvulsive seizures in posterior reversible encephalopathy syndrome (PRES): Neurocrit Care, 2018; 29; 481-90
18.. Herlimus FT, Wardani IAK, Widyadharma IPE, Unspecified severe mental and behavior disorder associated with puerperium (postpartum psychosis) in posterior reversible encephalopathy syndrome: A case report: Int J Res Med Sci, 2021; 9; 607
19.. Raman R, Devaramane R, Jagadish GM, Chowdaiah S, Various imaging manifestations of posterior reversible encephalopathy syndrome (PRES) on magnetic resonance imaging (MRI): Pol J Radiol, 2017; 82; 64-70
20.. McKinney AM, Short J, Truwit CL, Posterior reversible encephalopathy syndrome: Incidence of atypical regions of involvement and imaging findings: Am J Roentgenol, 2007; 189; 904-12
21.. Hinduja A, Habetz K, Raina S, Predictors of poor outcome in patients with posterior reversible encephalopathy syndrome: Int J Neurosci, 2017; 127; 135-44
22.. Hinduja A, Posterior reversible encephalopathy syndrome: Clinical features and outcome: Front Neurol, 2020; 11; 71
23.. Ellis CA, McClelland AC, Mohan S, Cerebrospinal fluid in posterior reversible encephalopathy syndrome: Implications of elevated protein and pleocytosis: Neurohospitalist, 2019; 9; 58-64
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133