30 November 2021: Articles ")
Hydatid Pulmonary Embolism: A Case Report and Literature Review
Challenging differential diagnosis, Rare disease
Adila Aili1AEF, Liqing Peng2A, Jiarui Zhang1B, Yu Liu1B, Lige Peng1B, Qun Yi1A, Haixia Zhou1A*DOI: 10.12659/AJCR.934157
Am J Case Rep 2021; 22:e934157






Abstract
BACKGROUND: Infection with Echinococcus granulosus is endemic in sheep and dogs in Central Asia, including Tibet. In humans, ingested parasites from the gastrointestinal system enter the liver via the portal vein. Rarely, hepatic hydatid cysts can rupture into the portal vein and embolize to the lungs. This report is of a 58-year-old woman with liver cysts and a pulmonary embolism due to hydatid disease.
CASE REPORT: We present a rare case of a pulmonary embolism caused by a hydatid cyst. A 58-year-old woman from the Tibet Autonomous Region of China was admitted to the hospital with symptoms of chest and back pain and shortness of breath within the previous 6 months. She had a 5-year history of hepatic echinococcosis. During hospitalization, the patient reported having aggravated chest and back pain and she developed a new symptom of hemoptysis. A pulmonary embolism was confirmed by computed tomography pulmonary angiography. After a multidisciplinary consultation, and based on the patient’s medical history, clinical manifestations, laboratory test results, and imaging findings, a diagnosis of a pulmonary embolism caused by a hydatid cyst was established.
CONCLUSIONS: This report shows the importance of imaging findings in diagnosing a non-thrombotic pulmonary embolism due to hepatic hydatid disease. In this case, early and accurate diagnosis resulted in appropriate treatment with multidisciplinary patient management.
Keywords: Echinococcosis, Membranous Obstruction of Inferior Vena Cava, Pulmonary Artery, Pulmonary Embolism, Animals, Cysts, Dogs, Echinococcosis, Hepatic, Female, Humans, Liver Diseases, Sheep
Background
Echinococcosis is a parasitic disease caused by a tapeworm and is responsible for affecting human health worldwide. Although it occurs globally, it is found mainly in countries dominated by agriculture and animal husbandry, and in China it occurs mostly in the northwest [1]. Echinococcosis is mainly caused by the larva of
Case Report
A 58-year-old woman from the Tibet Autonomous Region of China was admitted to the hospital with symptoms of chest and back pain and shortness of breath within the last 6 months. The patient reported that she had been diagnosed with hepatic hydatid disease 5 years prior. On physical examination, venous distension along the neck veins and diminished breath sounds of the right lower lung were noted.
On laboratory examination, the eosinophil counts were in the normal range. D-dimer was positive, with an increased value of 1.58mg/L fibrinogen equivalent units. Serologic testing was positive for antibodies against cystic hydatidosis (IgG 3.68 S/ cut-off). No other abnormal laboratory findings were observed.
The patient received an unenhanced computed tomography (CT) scan of the chest at a local hospital, showing pleural effusion in the right lung and ground-glass opacities on both sides of the lung. Abdominal ultrasonography showed an irregular echo zone of about 11.8×10 cm within the parenchyma of the right liver lobe, which was the hepatic echinococcosis. During hospitalization, the patient had aggravated chest and back pain and developed a new symptom of hemoptysis.
Because a pulmonary embolism was suspected, CT pulmonary angiography (CTPA) was performed, showing a filling defect in the trunk of the right pulmonary artery and in the basilar artery of the left lower lobe (Figure 1A, 1B). Cystic solid density shadows with separation inside could also be seen in the right hilum, right lower posterior mediastinum, and left lower lobe, with no obvious enhancement. The boundary between the lower edge of the lesion and the liver was not clear, and similar density shadows were seen in the liver (Figure 2A, 2B). The cystic solid lesion in the liver seemed to extend into the inferior vena cava.
The echocardiography revealed right heart enlargement and severe pulmonary arterial hypertension (78 mmHg). Chest radiography demonstrated an enlarged pulmonary tract and dilation of the right ventricle (Figure 3). Color Doppler ultrasound of the lower extremity vein found no abnormality. After multidisciplinary consultation, which was based on the patient’s medical history, clinical manifestations, laboratory test results, and imaging findings, the patient was diagnosed as having hydatid disease with liver, lung, and mediastinum involvement and a pulmonary embolism caused by hydatid cyst. Surgery was advised, but the patient refused surgery and was therefore discharged with albendazole tablets. The patient died of pulmonary hypertension and right heart failure 6 months later.
Discussion
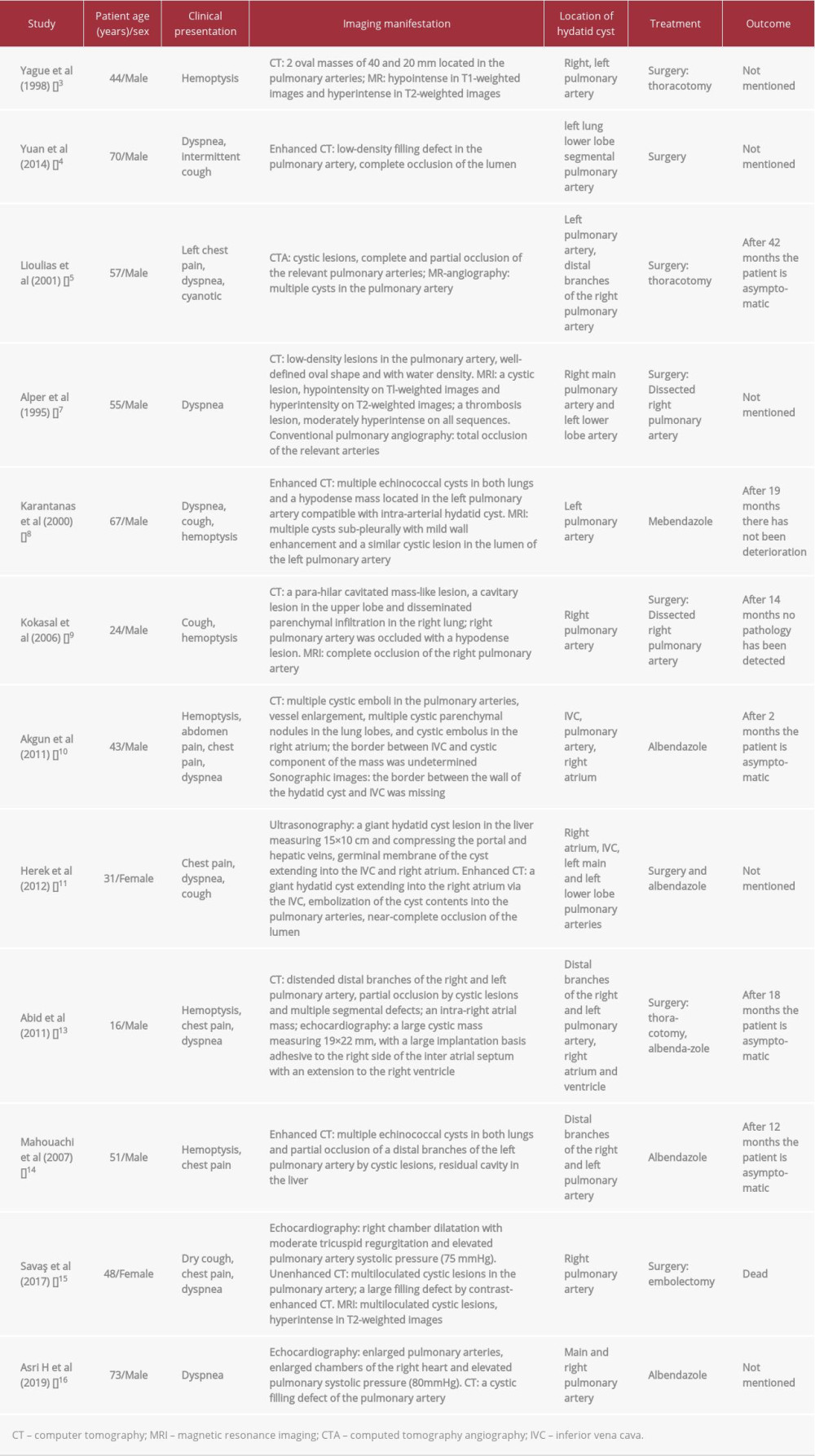
A pulmonary embolism caused by a hydatid cyst is a type of non-thrombotic pulmonary embolism with low morbidity but high mortality. It has been reported that echinococcosis of the pulmonary artery is mainly derived from hepatic hydatid cysts, and when these rupture in the liver or other organs in the abdomen, they invade the inferior vena cava or the hepatic vein. This enables the cyst contents to enter into the blood circulation and cause a pulmonary embolism after entering into the pulmonary artery and its branches through the right atrium and right ventricle [4–6]. By the time this situation occurs, the hydatid cyst is not usually seen in the right atrium or right ventricle, and most patients will have a history of hepatic hydatid disease. In our patient, as determined by the CTPA, cystic solid lesion in the liver extended into the inferior vena cava. Furthermore, echocardiography failed to detect a hydatid cyst in the right atrium or right ventricle. Taken together, these findings suggest it is possible that such a mechanism occurred in our patient, which could also have been the situation for 7 of the 12 cases we reviewed. Another less common mechanism of a pulmonary embolism caused by a hydatid cyst is the complication of cardiac hydatid disease, which occurs when hydatid cysts parasitizing the right atrium and the right ventricle fall off or rupture, and the contents within the cysts enter the pulmonary artery and its branches [7]. Three of the 12 cases reviewed here were confirmed to have cardiac hydatid disease. The rarest condition is when this parasite within the pulmonary artery wall or in the nearby lung parenchyma gradually grows and ruptures the arterial wall and then enters and blocks the pulmonary artery [8,9]. The pulmonary emboli caused by a hydatid cyst in 2 of the 12 cases we reviewed probably developed through this mechanism.
The clinical manifestations of a pulmonary embolism caused by a hydatid cyst are not specific, and relevant symptoms occur only when hydatid worms develop to block or puncture blood vessel walls. Hemoptysis may be the earliest and most common symptom for patients with the disease. In addition to hemoptysis, dyspnea, chest pain, and coughing, expecto-ration and allergic reactions can occur [10]. In the 12 cases we reviewed, hemoptysis was present in 6 cases, chest pain was presented in another 6 cases, and dyspnea was presented in all cases. There are mainly 3 outcomes of a pulmonary embolism caused by a hydatid cyst: (1) sudden death due to massive embolization; (2) death within 1 year due to pulmonary hypertension; and (3) long-term pulmonary hypertension [11,12]. Most patients appear to have chronic pulmonary hypertension accompanied by an acute pulmonary embolism. In some acute cases, hemorrhagic shock due to massive hemoptysis, hemorrhage due to rupture of a vessel wall, or anaphylactic shock because of the material in the cysts entering the bloodstream were the common causes of sudden death. In our case, the patient reported having chest and back pain and dyspnea 6 months previously, and the patient’s echo-cardiography showed severe pulmonary hypertension. While hospitalized, her chest pain was aggravated, and hemoptysis occurred. All these symptoms suggested that the patient may have had chronic pulmonary hypertension accompanied by an acute pulmonary embolism, both caused by hydatid cyst, and the patient died of pulmonary hypertension and right heart failure 6 months later.
Early diagnosis of a pulmonary embolism caused by a hydatid cyst is critical for early treatment and reduction of mortality. However, it is often difficult to diagnose due to the absence of specific symptoms or symptoms that do not support a pulmonary embolism. The disease tends to be confirmed only when the patient develops the relevant symptoms or experiences acute episodes, and, in some patients, it is only confirmed on autopsy. Laboratory tests for a pulmonary embolism caused by echinococcosis are not specific. However, the blood test for anti-hydatid antibodies is usually positive and the number of eosinophils tends to increase significantly [7,13]. In terms of imaging examinations, a chest X-ray is not helpful. Ultrasonography can show hydatid emboli in the blood vessels, atria, and ventricle, as well as hydatid cysts in major organs. Upon CT, non-complicated cysts usually show low levels of attenuation and well-defined limits, with the possible presentation of calcium on the periphery, depending on their developmental state. When using enhanced CT with contrast, only the wall is highlighted, whereas the appearance of the hydatid cyst on magnetic resonance imaging (MRI) is usually characteristic and can be observed as an oval lesion, which is hypointense on T1-weighted images and hyperintense on T2-weighted images. A typical image is represented by a peripheral ring and hypointense T2-weighted images, which represent the pericyst (a dense fibrous capsule from the reactive host tissue) [3,8]. Unfortunately, in our case, the patient refused MRI for economic reasons. At present, CTPA is the most commonly used method for the diagnosis of a pulmonary embolism. It can accurately show the blocked pulmonary artery and filling defect at corresponding vascular segments but cannot discern the part below the blocked vascular segment, and when the vessel is completely blocked, it is sometimes difficult to distinguish the type of pulmonary embolism. Therefore, a diagnosis of pulmonary embolism caused by a hydatid cyst should be based on a comprehensive consideration of medical history, clinical manifestations, and imaging results. The patient in our case had a 5-year history of hepatic echinococcosis and presented 3 typical signs of pulmonary embolism with chest pain, dyspnea, and hemoptysis. Also, a CTPA revealed filling defects in some pulmonary arteries, and a hydatid cyst lesion extended into the inferior vena cava. Thus, a pulmonary embolism caused by a hydatid cyst was considered, based on this comprehensive analysis.
Pulmonary embolism caused by a hydatid cyst generally has a poor prognosis, and surgery remains by far the best treatment option. The specific surgical method is selected according to the location of the hydatid embolus in the vascular lumen and its anatomical position. Thrombectomy is the most common surgical method, but the risk of perioperative death is relatively high. During surgery, hydatid cysts or arteries can rupture and lead to severe complications, such as anaphylactic shock, aneurysm, new embolus formation, or hydatid dispersion to other tissues and organs [9,14]. In the cases reviewed here, 8 of 12 received surgery. Among the 4 cases whose outcome was mentioned, 3 patients survived and 1 patient died after surgery. Medication is not very effective for pulmonary emboli due to the presence of hydatid cysts. However, it can be used in the following circumstances: (1) recurrent echinococcosis, (2) disseminated disease, including secondary lung or pleural hydatidosis, and (3) contraindication of surgery or high risk of hydatid fluid leakage during surgery. For medication, mebendazole and albendazole are mainly used and these medications can prolong survival time and improve quality of life of patients [13,14]. In the cases reported here, 4 out of 12 patients received only medication and after several months of follow-up, 3 patients were asymptomatic, and the outcome from 1 case was not recorded. In our case, the patient refused surgical and anticoagulation treatment and was discharged with albendazole tablets. Unfortunately, the patient died of pulmonary hypertension and right heart failure 6 months later.
Conclusions
For the diagnosis of pulmonary embolism caused by a hydatid cyst, careful evaluation of clinical manifestations and regular laboratory test results are necessary because of the lack of specific symptoms. However, the history of the parasite exposure in endemic areas and findings from imaging analyses can provide strong supporting evidence for a diagnosis. This report has shown the importance of imaging findings in diagnosing a non-thrombotic pulmonary embolism due to hepatic hydatid disease. In this case, early and accurate diagnosis resulted in appropriate treatment with multidisciplinary patient management.
Figures
References:
1.. , Echinococcosis May 17, 2021 Available from: https://www.who.int/news-room/fact-sheets/detail/echinococcosis
2.. Polat P, Kantarci M, Alper F, Hydatid disease from head to toe: Radiographics, 2003; 23(2); 475-94
3.. Yagüe D, Lozano MP, Lample C, Bilateral hydatid cyst of pulmonary arteries: MR and CT findings: Eur Radiol, 1998; 8(7); 1170-72
4.. Yuan Z, Maihesuti M, Wenya L, Rare reason for pulmonary embolism: One case of pulmonary hydatid cyst and review of the literature: J Thromb Thrombolysis, 2015; 40(1); 126-29
5.. Lioulias A, Kotoulas C, Kokotsakis J, Acute pulmonary embolism due to multiple hydatid cysts: Eur J Cardiothorac Surg, 2001; 20(1); 197-99
6.. El Hadj Sidi C, Mgarrech I, Alimi F, Four pathways for hydatid pulmonary embolism: J Card Surg Aug, 2020; 35(8); 1877-84
7.. Alper H, Yünten N, Scsener RN, Intramural hydatid cysts of pulmonary arteries: CT and MR findings: Eur Radiol, 1995; 5(6); 666-68
8.. Karantanas AH, Bitsios G, Karaiskou E, Echinococcus of the pulmonary artery: CT, MRI and MRA findings: Comput Med, 2000; 24(4); 265-67
9.. Koksal C, Baysungur V, Okur E, A two-stage approach to a patient with hydatid cysts inside the right pulmonary artery and multiple right lung involvement: Ann Thorac Cardiovasc Surg, 2006; 12(5); 349
10.. Akgun V, Battal B, Karaman B, Pulmonary artery embolism due to a ruptured hepatic hydatid cyst: Clinical and radiologic imaging findings: Emerg Radiol, 2011; 18(5); 437-39
11.. Herek D, Karabulut N, CT demonstration of pulmonary embolism due to the rupture of a giant hepatic hydatid disease: Clin Imaging, 2012; 36(5); 612-14
12.. Kardaras F, Kardara D, Tselikos D, Fifteen year surveillance of echinococcal heart disease from a referral hospital in Greece: Eur Heart J, 1996(8); 1265-70
13.. Abid L, Laroussi L, Abdennadher M, A cardiac hydatid cyst underlying pulmonary embolism: A case report: Pan Afr, 2011; 8(1); 12
14.. Mahouachi R, Berraies A, Taktak S, Pulmonary hydatid cyst embolization successfully treated with albendazole: Respir Med Extra, 2007; 3(4); 192-94
15.. Savaş G, Coşgun MS, Karabıyık U, A rare cause of pulmonary embolism: hydatid cyst: Am J Respir Crit Care Med, 2017; 196(3); 386
16.. Asri H, Zegmout A, Abid A, A rare cause of chronic pulmonary embolism: Hydatid cyst: Arch Bronconeumol, 2018; 55(2); 101
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133