31 January 2022: Articles 
Case Report: Rocky Mountain Spotted Fever with Adrenalectomy and a Hard-to-Find Tick
Rare disease
Chenxuan Zhou1BCDEF*, Pace Woods1ABCD, Andrew Abouzeid2BCD, Michelle N. Brooks2EGDOI: 10.12659/AJCR.934505
Am J Case Rep 2022; 23:e934505






Abstract
BACKGROUND: Rocky Mountain spotted fever (RMSF) is a potentially fatal infectious disease caused by the gram-negative intracellular bacterium Rickettsia rickettsii. The classic triad includes fever, rash, and history of tick exposure; however, the triad presents in only 3% to 18% of cases at the initial visit, and the tick bite is often painless and overlooked. RMSF can present with other manifestations, including hyponatremia, lymphopenia, thrombocytopenia, and coagulopathy. Some of these manifestations can be overlooked if they overlap with manifestations of a patient’s pre-existing conditions.
CASE REPORT: A 43-year-old woman with RMSF presented with fever and treatment-resistant hyponatremia before developing a rash. Initially, the cause of her hyponatremia was attributed to adrenal insufficiency and dehydration. After appropriate treatments with hormone replacement therapy and intravenous hydration, her laboratory values remained relatively unchanged. A rash later appeared with an atypical RMSF pattern, warranting a detailed integumentary examination, which uncovered the culprit tick in an unusual location. After starting doxycycline, the patient’s signs and symptoms, including her sodium level, improved.
CONCLUSIONS: We conclude that the diagnosis of RMSF is an empiric diagnosis based on clinical signs, symptoms, and appropriate epidemiologic settings for tick exposures. However, typical clinical signs do not always display at presentation. Other manifestations that a patient’s pre-existing conditions can simultaneously cause should not be overlooked and should be examined holistically with other signs, symptoms, laboratory values, and physical examinations. Early treatment with doxycycline is encouraged as evidence strongly suggests that early treatment is correlated with lower mortality.
Keywords: Adrenalectomy, Hyponatremia, Rocky Mountain Spotted Fever, Adult, Animals, doxycycline, Exanthema, Female, Humans, Ticks
Background
Rocky Mountain spotted fever (RMSF) is a potentially fatal infectious disease caused by the gram-negative intracellular bacterium
Case Report
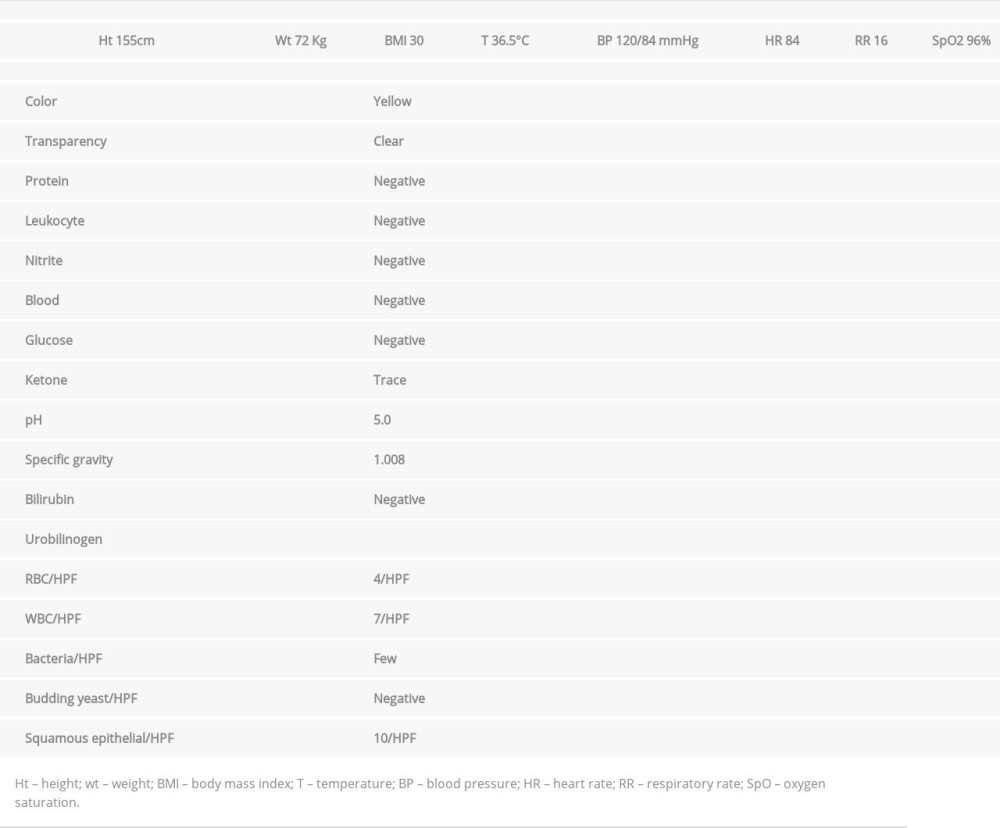
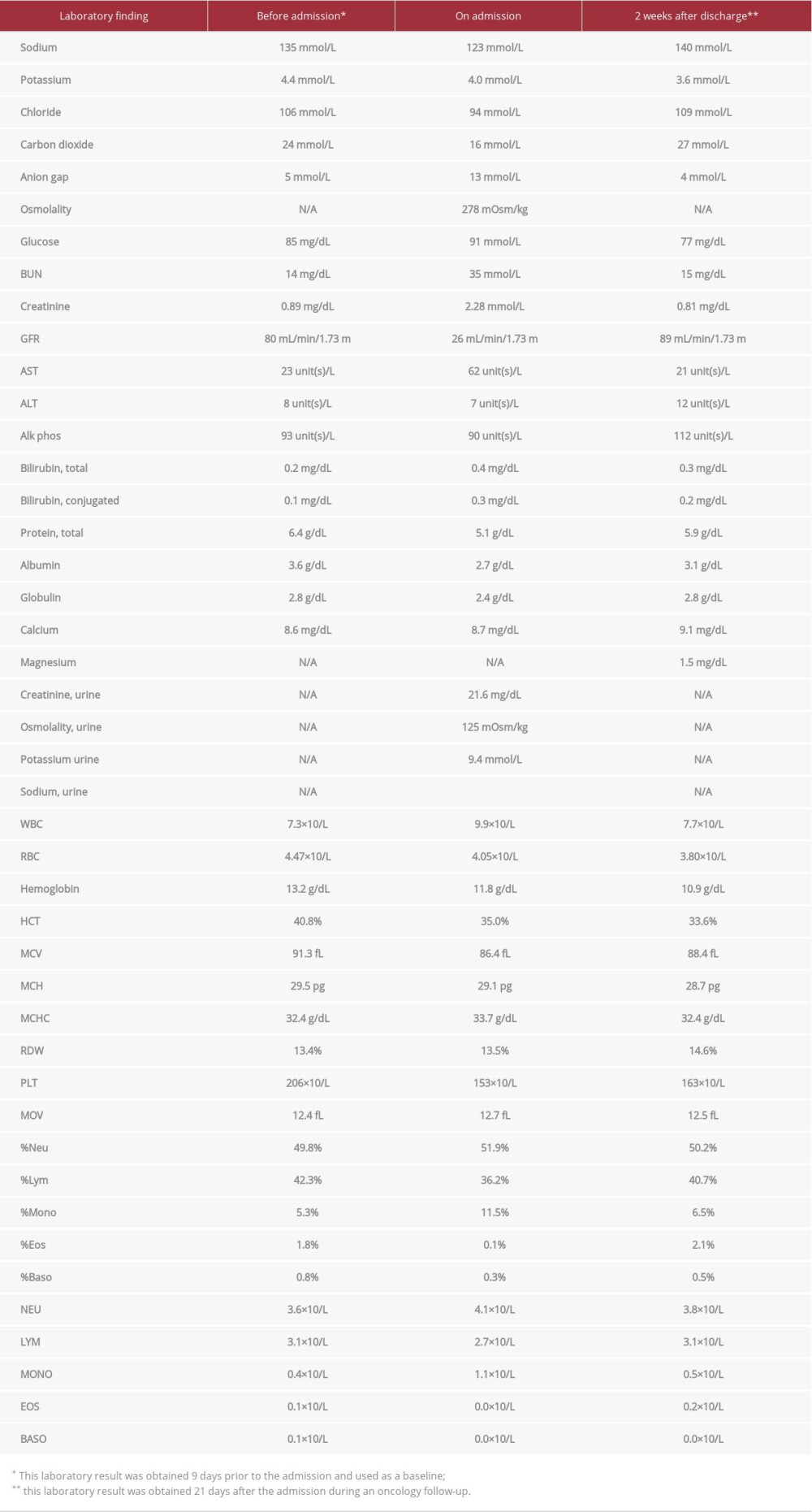
A 43-year-old woman with a past medical history of adrenal cortical carcinoma (pT2NxM0) treated by adrenalectomy on adjuvant mitotane (500 mg 3 tablets 3 times daily), hydro-cortisone (10 mg 2 tablets in the morning 1 tablet in the evening, with double the dose if patient feels sick), and fludrocortisone (0.1 mg half tablet daily), presented to the hospital Emergency Department with general malaise, a subjective fever, and poor tolerance of oral intake for 3 days. The patient was seen at an urgent care facility when she initially felt ill 3 days earlier, and urinalysis results were reportedly suggestive of a urinary tract infection. She was subsequently given an unknown dose of intramuscular ceftriaxone and oral ciprofloxacin. Vital signs and urinalysis taken upon admission are included in Table 1. All other laboratory findings from 9 days before the admission by a clinic, upon admission, and 21 days after the admission during oncology follow-up are included in Table 2; the laboratory results before and after admission are used as the baseline and the recovery reference, respectively. It is worth noting that a complete physical examination was unremarkable, including an integumentary examination showing no signs of rashes or lesions. Her complete metabolic profile revealed hyponatremia (serum sodium of 123 mmol/L), acute kidney injury (creatinine of 2.28 mg/dL), an elevated urine osmolality of 125 mOsm/kg, and low urine sodium <20 mEq/L, which was consistent with acute kidney injury secondary to hypovolemic hyponatremia. Upon questioning, the patient endorsed that her adrenal cortical carcinoma had been well managed by mitotane, hydrocortisone, and fludrocortisone and she denied taking any stress dose of the glucocorticoid after she became ill 3 days earlier. The hyponatremia was attributed to adrenal insufficiency caused by a lack of stress dose of glucocorticoid in her setting of acute illness. Consequently, her home dose of hydrocortisone was doubled, and her mitotane was held. One liter of intravenous (i.v.) lactated Ringer’s solution was also administered, and her sodium level slightly improved to 131 mmol/L. A computed tomography scan was ordered to rule out any malignancy that may have caused a paraneoplastic syndrome of inappropriate antidiuretic hormone secretion, and it came back negative. In addition, the level of white blood cells was non-elevated, and a repeat urinalysis was inconsistent with urinary tract infection. The patient’s overall presentation made an infectious process unlikely, and she was admitted to be monitored for her sodium level.
Unexpectedly, on the next day, the patient’s fever spiked to 39.3°C. On physical examination, newly-developed, diffuse small erythematous blanching papules with some coalescences were noted on the patient’s shoulder, bilaterally extending to the scapula and humerus region, sparing the palmar and plantar surfaces, raising concern for a drug reaction because a rash starting on the shoulder is atypical for RMSF. A dermatology consultation was requested and a complete integumentary examination was performed, showing dissemination of the rash on the back, shoulders, and abdomen; the palmer and plantar surfaces were uninvolved. A tiny 4-legged tick with a central white spot on the dorsum was discovered in the left inframammary fold, likely an
One day later, the patient was discharged as she became hemodynamically stable. She was next seen for an oncology follow-up 21 days after the discharge to discuss the option of restarting her mitotane therapy. Per the clinical notes, she reported a dramatic improvement of her symptoms, including the fever and the rash, except for some residual fatigue. Per laboratory results, her hyponatremia had been resolved completely (Figure 1).
Discussion
RMSF cases have risen steadily, from 495 cases in 2000 to a peak of 6248 cases in 2017, with 5 states (Arkansas, Missouri, North Carolina, Tennessee, and Virginia) accounting for over 50% of the total cases [3]. The etiologic agent for RMSF is
As a result of the vascular injury, if treated late, RMSF can cause severe kidney injury or lead to potentially fatal complications, such as the development of severe cerebral edema [6]. The diagnosis of RMSF is empirically based on consistent clinical signs and an appropriate epidemiologic setting. Early treatment is preferred, and clinicians should not wait for the skin rash to develop before initiating treatment [7].
As an essential piece of social history, camping has been associated with the diagnosis of RMSF; however, our patient did not report any recent history of camping. The principal vector of RMSF in the eastern United States is
However, the diagnosis of RMSF can be challenging even in areas with more frequent cases, especially when the clinical presentations of RMSF can resemble the signs and symptoms of a patient’s pre-existing conditions, which, in our case, was hyponatremia secondary to chronic iatrogenic adrenal insufficiency. When our patient presented in the Emergency Department, her adrenal insufficiency was conveniently believed to be the only cause of her hyponatremia. Further, the repeat urinalysis and non-elevated white blood cell count made an infectious process unlikely. However, it became clear later on that her adrenal insufficiency was not the sole contributor to the hyponatremia, as the sodium level failed to improve appropriately after aggressive i.v. fluid therapy and mineralocorticoid replacement therapy. After she was started on doxycycline, the patient showed a steady improvement of her sodium level, which returned to the normal (140 mmol/L) range upon follow-up. This confirms that an active infection of RMSF was partially responsible for the hyponatremia that the patient presented with.
The routine diagnosis of RMSF is by indirect fluorescent antibody (IFA) testing for the IgM and IgG antibodies to
During an attempt to review the management of this patient, it was believed that obtaining and trending the level of ADH was indicated when the patient presented with a decreased level of sodium. This could be incorporated in the initial work-up of patients presenting with hyponatremia. It was also argued that being a cancer patient with glucocorticoid replacement made the patient prone to infectious disease; however, a literature review suggests that among 7738 cases of patients with RMSF, only 325 (4.2%) cases reported an immunosuppressive condition and only 33 (0.4%) cases were cancer, although immunosuppressed patients are 4.4 times as likely to die from RMSF [13].
Conclusions
In summary, RMSF is an empiric diagnosis based on clinical signs, symptoms, and appropriate epidemiologic settings for tick exposures. Early treatment with doxycycline is encouraged as evidence strongly suggests that early treatment is correlated with lower mortality. Symptoms (in our case, hyponatremia) that a patient’s pre-existing conditions can simultaneously cause should not be overlooked. If a patient fails to respond to treatment, the presenting signs should be examined holistically with other signs, symptoms, and laboratory findings. Last but not least, a thorough physical examination can often unveil more clues for the underlying cause of the patient’s disease. In our case, the culprit tick had always been on the patient’s skin and hiding in the left inframammary fold.
References:
1.. Thorner AR, Walker DH, Petri WA, Rocky mountain spotted fever: Clin Infect Dis, 1998; 27(6); 1353-59
2.. Regan J, Traeger M, Humpherys D, Risk factors for fatal outcome from Rocky Mountain spotted fever in a highly endemic area – Arizona, 2002–2011: Clin Infect Dis, 2015; 60(11); 1659-66
3.. : Rocky Mountain spotted fever (RMSF), Epidemiology and statistics, Centers for Disease Control and Prevention [Cited 2021 Dec 6] Available from URL: https://www.cdc.gov/rmsf/stats/index.html
4.. Rydkina E, Sahni A, Baggs R, Infection of human endothelial cells with spotted fever group rickettsiae stimulates cyclooxygenase 2 expression and release of vasoactive prostaglandins: Infect Immun, 2006; 74(9); 5067-74
5.. Kaplowitz L, Hyponatremia in Rocky Mountain spotted fever: Role of antidiuretic hormone: Ann Intern Med, 1983; 98(3); 334-35
6.. Rhodes S, Teagarden A, Graner B, Brain death secondary to Rocky Mountain spotted fever encephalitis: Case Rep Crit Care, 2020; 2020; 5329420
7.. Walker D, Rocky Mountain spotted fever: A seasonal alert: Clin Infect Dis, 1995; 20(5); 1111-17
8.. Sexton D, McClain M, Clinical manifestations and diagnosis of Rocky Mountain spotted fever, n.d UpToDate. [Cited 2021 December 4], Available from URL: https://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-rocky-mountain-spotted-fever
9.. Kirkland K, Wilkinson W, Sexton D, Therapeutic delay and mortality in cases of Rocky Mountain spotted fever: Clin Infect Dis, 1995; 20(5); 1118-21
10.. Buckingham SC, Marshall GS, Schutze GE, Tick-borne Infections in Children Study Group. Clinical and laboratory features, hospital course, and outcome of Rocky Mountain spotted fever in children: J Pediatr, 2007; 150(2); 180-4(184.e1)
11.. McQuiston J, Dunn J, Morris K, Inadequacy of IgM antibody tests for diagnosis of Rocky Mountain spotted fever: Am J Trop Med Hyg, 2014; 91(4); 767-70
12.. Dantas-Torres F, Rocky Mountain spotted fever: Lancet Infect Dis, 2007; 7(11); 724-32
13.. Dahlgren F, Holman R, Paddock C, Fatal rocky mountain spotted fever in the United States, 1999–2007: Am J Trop Med Hyg, 2012; 86(4); 713-19
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133