04 January 2022: Articles 
Isolated Perianal Endometrioma: A Case Report and Literature Review
Unusual clinical course, Challenging differential diagnosis
Riyadh HakamiDOI: 10.12659/AJCR.934745
Am J Case Rep 2022; 23:e934745






Abstract
BACKGROUND: Endometriosis, a common condition among women of reproductive age and infertile women, occurs when the endometrium extends outside the uterus. When this endometrial tissue grows and sheds, symptoms will develop. The presentation varies depending on the site involved; however, cyclical pain is among its most common symptoms, along with bleeding and cramping. It is frequently observed in the ovaries and fallopian tubes; in contrast, the anal canal is rarely involved. Here, we report a very unusual presentation of the disease.
CASE REPORT: A 33-year-old woman with a history of episiotomy presented to the Emergency Department reporting perianal swelling in the previous year. The swelling was associated with intermittent pain and difficulty passing stool. She reported no fever. On examination, there was a 3×4 cm palpable tender perianal mass extending to the anal sphincter at the 11 o’clock position. Bedside ultrasound revealed a mass. Magnetic resonance imaging showed a hemorrhagic 3×4 cm mass in the right perianal region pressing on and indenting the right aspect of the distal external sphincter. The mass was excised completely with local perianal incision over the mass at 11’o clock. Surgical pathology revealed an isolated endometrioma in the perianal area.
CONCLUSIONS: Isolated perianal endometrioma is a rare disease, with only 21 published cases. Its diagnosis is difficult to establish, and a wide range of tests is often needed. Laparoscopic or surgical intervention may be required in cases of rectal endometriosis for an accurate diagnosis. Careful history taking and examination along with a high index of suspicion are necessary to diagnose perianal endometrioma.
Keywords: Anal Canal, Colorectal Surgery, Endometriosis, Adult, Anus Diseases, Episiotomy, Female, Humans, Infertility, Female, Perineum, Pregnancy
Background
Endometriosis occurs when the lining of the uterus, the endometrium, grows in other places such as the fallopian tubes, along the pelvis, or in the ovaries [1]. When this lining breaks down, it usually has nowhere to go, causing heavy menstrual periods and severe cramps. Endometriosis affects approximately 10–15% of women of reproductive age [2]. It most commonly affects women aged 25–35 years. Its incidence increases to as much as 25–50% in infertile women [3]. The criterion standard diagnostic modality is histopathology obtained from laparoscopic tissue biopsy of endometriotic implants. It most commonly occurs in the ovaries, anterior or posterior cul-de-sac, the broad and uterosacral ligaments, uterus, fallopian tubes, sigmoid colon, or appendix [4].
This report describes a case of isolated perianal endometrioma. Written informed consent was obtained from the patients for future research and publication.
Case Report
A 33-year-old woman with no known medical illnesses visited the Emergency Department reporting a 1-year history of swelling in the perianal area associated with intermittent pain and difficulty defecating. Upon further questioning, she realized that her pain mainly occurred during her menstrual cycle. She denied any history of fever, discharge, or bleeding. She was a para 2 with a history of 2 normal deliveries. The first delivery was 13 years ago and the last delivery was 8 years ago. Both deliveries required an episiotomy. She started to notice the symptoms and the mass 1 year ago. She had no history of contraceptive use, and she takes paracetamol, with minimal relief.
A physical examination revealed a 3×4 cm palpable tender perianal mass extending to the anal sphincter at the 11 o’clock position. No redness or discharge was observed. Magnetic resonance imaging (MRI) revealed a 3×4 cm mass in the right perianal region pressing on and indenting the right aspect of the distal external sphincter. This mass showed mixed intermediate and high signal intensity on T2W1, attributed to the hemorrhagic component. There was an associated diffusion restriction but no avid enhancement after intravenous contrast administration. No fatty components were observed. The exact nature of this mass was indeterminate. The incidental finding of a 2×2 cm anorectal polyp with stalk was seen at the right posterolateral aspect. No signs of invasion beyond the muscularis propria were noted. This polyp was seen approximately 3.1 cm above the anal verge. No mesorectal lymphadenopathy was noted.
The patient was counseled to undergo an examination under anesthesia and possible surgical excision of the mass along with anal polyp removal. She agreed to undergo surgery under general anesthesia. For the surgery, she was placed in the prone position. Examination of the anal canal showed 3 polyps, which were excised. The mucosal defect was closed using 3-0 Vicryl. Attention was then given to the perianal area, in which a cyst was found in the right ischioanal fossa. An elliptical incision was made that was very close to the external anal muscle; with careful dissection, it was separated and the cyst wall was excised. The mass was completely excised with intact capsule and a less than 1-cm margin. She was shifted back to the day surgery unit in stable condition and discharged later the same day in good condition.
A histopathological examination of the perianal cyst excision revealed a 4×4 cm endometrioma (Figures 1–3). Surgical pathology gross examination showed brown-tan skin tissues with underlining subcutaneous tissue, and the cut section revealed heterogeneous yellowish-brown fatty tissue. The anal mucosal polyps were hyperplastic. The patient was seen in the clinic, and the wound healed well. The patient was referred to the Gynecology Department for further assessment and treatment. A gynecological ultrasound revealed a retroverted uterus with no ovarian endometrioma. She was then started on a course of combined oral contraceptive pills to prevent endometriosis recurrence.
Discussion
Perianal endometriosis is extremely rare. It usually occurs in episiotomy scars, and can involve the septum that separates the vagina and anal canal, with an incidence of approximately 0.2% [5,6]. A clinician might fail to diagnose perianal endometriosis if there is no visible scar in the perineum and the patient has never undergone an episiotomy. In addition, it might be difficult to make a diagnosis if the patient does not report feeling cyclical pain; thus, it might be treated as a perianal abscess [5].
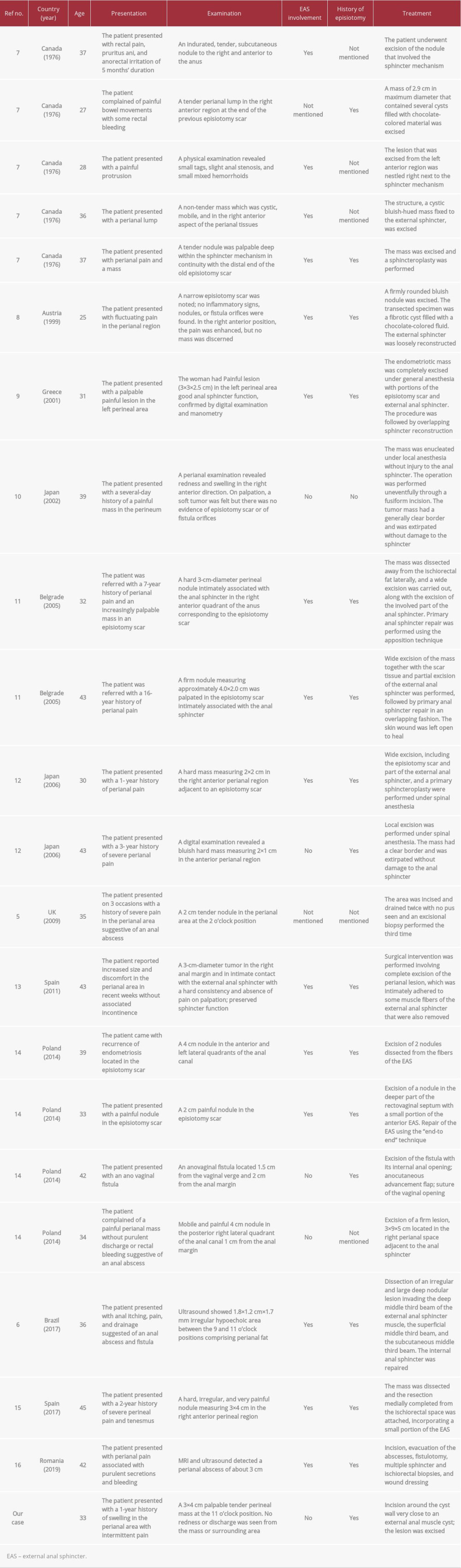
As of this writing, 21 these rare cases have been published (Table 1) [5–16]. Our case brings the grand total to 22. In the review of these cases, perianal endometriosis affected child-bearing women following obstetric or gynecological procedures, which might transplant the endometrial tissue to uncommon sites. Three reported cases revealed that perianal endometriosis mimicked the presentation of a perianal abscess located in the episiotomy scar [5,6,14]. Fifteen of 21 cases involved endometriosis attached to the anal sphincter, and 8 cases required sphincter repair during surgical removal. Because perianal abscesses are usually handled by junior surgeons, the unusual presenting features of perianal endometriosis may go unnoticed. This can lead to unnecessary operations or an inappropriate diagnosis. It is important to be highly suspicious when making a diagnosis, especially when a patient suffers from recurrent perianal pain and no pus is found. Fine-needle aspiration cytology can help make the correct diagnosis [17]. Transanal ultrasonography can aid in accurately gauging the exact endometrioma’s anatomical location and involvement of the external sphincter. Thus, painful perianal abrasions are indicative of a perianal abscess; when they recur, Crohn’s disease is usually suspected [5].
Anal endometriosis cannot be diagnosed by physical examination, and imaging techniques must be utilized. Although some patients with anal endometriosis may be asymptomatic, many develop stomach problems [18]. There are no clear guidelines for evaluating patients suspected of having the condition, but the most common presenting medical features include infertility and pelvic pain [19]. However, various techniques have been advocated for its diagnosis, such as double-contrast barium enema, transvaginal ultrasonography, MRI, rectal endoscopic ultrasonography, and multislice computed tomography enteroclysis. The regularity of rectal endometriosis is unknown, but among cases of bowel permeation, approximately 90% are contained in the rectum or sigmoid colon [19], while the rest are present in the ileum, appendix, and cecum [18]. This results in changes in bowel habits, such as diarrhea, constipation, rectal bleeding, and dyschezia. When the disease is moderate or severe, intestinal symptoms may be present that may differ depending on the location and menstrual cycle [20]. The symptoms of the condition may overlap with those of others, thus delaying diagnosis or treatment. Perianal endometriosis can result from painful vulvar lumps with cyclic swelling that form subcutaneous masses with inner hemorrhaging. Although this condition is rare, patients with a history of lesions in response to the menstrual cycle should be diagnosed with endometriosis [21]. The presence of endometrial tissue in a perianal site indicates perianal endometriosis. Retrograde menstruation is considered a cause of this condition. During vaginal delivery, feasible endometriotic cells become embedded in the perineum, including the episiotomy site, which leads to endometriotic lacerations. Coelomic metaplasia and transplantation of the exfoliated endometrium may also lead to perianal endometriosis. Anal endometriosis can be successfully managed laparoscopically, as it is both safe and effective [22]. Rectal resection improves symptoms but may result in complications such as rectovaginal fistula or anastomotic leakage [23]. Management of the condition remains tentative, necessitating expert management between symptom severity and extended follow-up viability [18]. Some patients show markedly enhanced quality of life after broad surgery. Anal nodules can become detached by nodulectomy, segmental resection, mucosal skinning, and full-thickness disc resection [18]. Indications for colorectal resection are currently debated, but statistics suggest that hard-line surgery improves patient symptoms. Helpful investigations into endometriosis reported an average time of 6.7 years from the commencement of symptoms of endometriosis to surgical diagnosis [24]. Each affected woman loses many hours of work per week because of reduced effectiveness while working under this debilitative disease. Thus, it is necessary to discover and identify new endometriosis-associated biomarkers while validating existing biomarkers. This will help in the development of more accurate and noninvasive methods for the diagnosis of anal endometriosis. In addition, the varying clinical classifications of endometriosis must be considered in the assessment of prognostic and diagnostic biomarkers [24]. Several methods to diagnose and image preoperative endometriosis have been investigated, including ultrasound, MRI, and computed tomography [25]. An ideal endometriosis test would have high sensitivity to ensure that it does not miss a diagnosis or another pelvic condition that could benefit from diagnostic or operative laparoscopy. Techniques in resolution imaging continue to improve, but their accuracy at this time is inferior to that of direct laparoscopic visualization. In addition, more training in the use of imaging for endometriosis is required to achieve higher sensitivity and specificity rates. Additionally, the cost of using these procedures as a selection tool must also be considered. Therefore, the development of imaging techniques must be examined for use in diagnosis of anal endometriosis.
Data could be collected and evaluated across female populations for the phenotypic manifestation of the condition, its symptomatology, and a method found to finely characterize the differences between patients [25]. Well-designed and adequately powered controlled trials and long-term studies are also critical for the comparison of different treatment options alongside definite outcome measures. These trials could concentrate on results that are highly relevant to women, such as quality of life and live birth [25]. Genomics research will also help researchers further comprehend genetic expression in the endometrium of those who have the condition versus controls. Diet is also important in the etiology of the condition; therefore, studies should focus on diet and endometriosis risk to clarify the function of diet in changing the symptoms and underlying disease. The management of perianal endometriosis includes both surgical and medical treatments. Wide local excision that spares the anal sphincter can cure the condition, with the addition of hormonal treatment if the sites are multiple [5]. Narrow excision near the edge of the endometrioma and primary sphincteroplasty can be successfully used to manage these conditions. However, early diagnosis and treatment are important to preventing progressive involvement in the surrounding tissues, most notably the anal sphincter, to decrease the risk of postoperative fecal incontinence.
Conclusions
Isolated perianal endometrioma is difficult to diagnose and is easily missed by perianal elliptical incision. The presentation may include cyclic pain along with perianal mass. Treatment options for abdominal and pelvic locations of endometriosis range from medical to laparoscopic intervention or even laparotomy. The patient should be treated postoperatively to prevent reoccurrence. Early intervention can significantly improve patient quality of life, and the diagnosis can only be confirmed by histopathological examination.
Figures
References:
1.. Brosens I, Benagiano G, Endometriosis, a modern syndrome: Indian J Med Res, 2011; 133; 581-93
2.. Olive DL, Pritts EA, Treatment of endometriosis: N Engl J Med, 2001; 345(4); 266-75
3.. Verkauf BS, Incidence, symptoms, and signs of endometriosis in fertile and infertile women: J Fla Med Assoc, 1987; 74(9); 671-75
4.. Macer ML, Taylor HS, Endometriosis and infertility: A review of the pathogenesis and treatment of endometriosis-associated infertility: Obstet Gynecol Clin North Am, 2012; 39(4); 535-49
5.. Iqbal M, Thumbe V, Dhange R, Perianal endometriosis mimicking recurrent perianal abscess: Case Rep Gastroenterol, 2009; 3(3); 414-17
6.. Rodrigues BD, Alves MC, da Silva AL, Reis IG, Perianal endometriosis mimicking recurrent perianal abscess: Case report and literature review: Int J Colorectal Dis, 2016; 31(7); 1385-86
7.. Gordon PH, Schottler JL, Balcos EG, Goldberg SM, Perianal endometrioma: Report of five cases: Dis Colon Rectum, 1976; 19(3); 260-65
8.. Schweiger W, Bacher H, Cerwenka H, Mischinger HJ, Perianal endometriosis with involvement of the external anal sphincter: Eur J Surg, 1999; 165(6); 615-17
9.. Kanellos I, Kelpis T, Zaraboukas T, Betsis D, Perineal endometriosis in episiotomy scar with anal sphincter involvement: Tech Coloproctol, 2001; 5(2); 107-8
10.. Watanabe M, Kamiyama G, Yamazaki K, Anal endosonography in the diagnosis and management of perianal endometriosis: Report of a case: Surg Today, 2003; 33(8); 630-32
11.. Barisic GI, Krivokapic ZV, Jovanovic DR, Perineal endometriosis in episiotomy scar with anal sphincter involvement: Report of two cases and review of the literature: Int Urogynecol J Pelvic Floor Dysfunct, 2006; 17(6); 646-49
12.. Toyonaga T, Matsushima M, Tanaka Y, Endoanal ultrasonography in the diagnosis and operative management of perianal endometriosis: Report of two cases: Tech Coloproctol, 2006; 10(4); 357-60
13.. Maturana Ibanez V, Ferrer Marquez M, [Extrapelvic endometriosis: A diagnosis to consider in the patient with a perianal tumour]: Cir Esp, 2011; 89(9); 619-20 [in Spanish]
14.. Kolodziejczak M, Sudol-Szopinska I, Santoro GA, Ultrasonographic evaluation of anal endometriosis: Report of four cases: Tech Coloproctol, 2014; 18(11); 1099-104
15.. Gonzalez-Longoria G, Mejia-Ovalle RR, Salinas-Aragon E, [Perineal endometriosis with anal external sphincter involvement: A case-report]: Rev Gastroenterol Mex, 2011; 76(2); 173-77
16.. Andrei LS, Popisteanu RS, Andrei A, Rare case of perianal endometriosis complicated with perianal fistula: Case report: Modern Medicine, 2019; 26(2); 89-91
17.. Simsir A, Thorner K, Waisman J, Cangiarella J, Endometriosis in abdominal scars: A report of three cases diagnosed by fine-needle aspiration biopsy: Am Surg, 2001; 67(10); 984-86
18.. Remorgida V, Ferrero S, Fulcheri E, Bowel endometriosis: Presentation, diagnosis, and treatment: Obstet Gynecol Surv, 2007; 62(7); 461-70
19.. Wolthuis AM, Meuleman C, Tomassetti C, Bowel endometriosis: Colorectal surgeon’s perspective in a multidisciplinary surgical team: World J Gastroenterol, 2014; 20(42); 15616-23
20.. Kaufman LC, Smyrk TC, Levy MJ, Symptomatic intestinal endometriosis requiring surgical resection: Clinical presentation and preoperative diagnosis: Am J Gastroenterol, 2011; 106(7); 1325-32
21.. Nasu K, Okamoto M, Nishida M, Narahara H, Endometriosis of the perineum: J Obstet Gynaecol Res, 2013; 39(5); 1095-97
22.. Nezhat C, Nezhat F, Pennington E, Laparoscopic disk excision and primary repair of the anterior rectal wall for the treatment of full-thickness bowel endometriosis: Surg Endosc, 1994; 8(6); 682-85
23.. Koh CE, Juszczyk K, Cooper MJ, Solomon MJ, Management of deeply infiltrating endometriosis involving the rectum: Dis Colon Rectum, 2012; 55(9); 925-31
24.. Rogers PA, D’Hooghe TM, Fazleabas A, Defining future directions for endometriosis research: Workshop report from the 2011 World Congress of Endometriosis In Montpellier, France: Reprod Sci, 2013; 20(5); 483-99
25.. Chamie LP, Blasbalg R, Pereira RM, Findings of pelvic endometriosis at transvaginal US, MR imaging, and laparoscopy: Radiographics, 2011; 31(4); E77-100
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133