20 December 2021: Articles 
Pleural Empyema as a Complication of Pyogenic Liver Abscess: Can the Minimum Achieve the Optimal? A Comparison of 3 Approaches
Rare coexistence of disease or pathology
Zeead M. AlGhamdi1ADEF*, Dhuha N. Boumarah2ADEF, Shadi Alshammary2ADEF, Hatem ElbawabDOI: 10.12659/AJCR.935169
Am J Case Rep 2021; 22:e935169






Abstract
BACKGROUND: Pyogenic liver abscess is an uncommon entity that is potentially lethal. Pleural empyema and mediastinal collection are 2 rare complications of hepatic abscess that negatively impact the prognosis.
CASE REPORT: Herein, we report 3 cases of pyogenic liver abscesses complicated by pleural empyema, each approached differently, along with a succinct review of the literature. Case 1: A 29-year-old man diagnosed with Crohn’s disease presented with Crohn’s disease-associated hepatic abscess complicated by pleural empyema and concurrent mediastinal collection. The patient demonstrated significant improvement after administration of intrapleural fibrinolytic therapy. Case 2: A 42-year-old man with unremarkable past medical history presented with abdominal pain and dyspnea. Upon investigation, he was found to have massive pleural empyema secondary to liver abscess. In contrast to case 1, case 2 required pleural debridement via video-assisted thoracoscopic surgery followed by formal decortication through a posterolateral thoracotomy. Thereafter, a dramatic clinical improvement was observed. Case 3: A 26-year-old man with history of brucellosis 6 months before was transferred to our facility as a case of pleural empyema secondary to transdiaphragmatic extension of liver abscess. Unlike case 1 and 2, this patient was managed by drainage of hepatic and pleural collections under radiological guidance only, without the need for intrapleural fibrinolytic therapy or surgical intervention.
CONCLUSIONS: The current paper sheds light on one of the uncommon complications of hepatic abscess and contributes to this scant literature by summarizing pertinent publications. Adequate drainage remains the cornerstone of any pus collection management despite the complexity of some encountered cases.
Keywords: Crohn Disease, Empyema, Pleural, Liver Abscess, Pyogenic, Adult, Humans
Background
Pyogenic liver abscess (PLA) is recognized as an uncommon entity, with an estimated incidence ranging between 0.5% and 0.8% [1]. Although mortality and morbidity rates have decreased tremendously with recent advances in diagnostic and therapeutic modalities, PLA remains a potentially life-threatening condition, with an overall mortality rate reaching up to 30% [2]. This is mainly attributed to the associated broad spectrum of sequelae, including sepsis, hepatic failure, and extension to adjacent structures [3]. Pleural empyema and mediastinal collection, in particular, are 2 of the rare complications of liver abscess [4]. Surprisingly, it has been reported that PLA-related empyema has a fatality rate of 100% when left untreated, leading to inevitable death [5]. Therefore, when similar rare complications present, they significantly worsen the prognosis and represent a significant challenge for physicians [4]. Herein, we report 3 cases of pyogenic liver abscess complicated by pleural empyema and present a succinct review of the literature.
Case Reports
CASE 1:
A 29-year-old man diagnosed with Crohn’s disease (CD) 2 months prior presented to the emergency room (ER) with a 1-week history of right upper quadrant (RUQ) abdominal pain. The pain was associated with subjective fever, constipation, abdominal distension, and exertional dyspnea. He also reported a history of unintentional weight loss of 9 kg within the previous 2 months. When the CD diagnosis was established, the patient was started on immunosuppressive medications, namely, prednisolone and mesalamine. Furthermore, he was an occasional alcohol consumer and tobacco smoker for 11 years. The patient also gave a history of daily cannabis consumption, but he had no history of recent travel or contact with sick patients, and he was not an intravenous (i.v.) drug user. Upon examination, the patient was noted to be slightly tachycardic and tachypneic. Diminished air entry over the right lung base with stony dullness note on percussion were evident on chest examination. An abdominal examination showed mild RUQ tenderness and hepatomegaly, with a liver span of approximately 20 cm.
Laboratory results revealed microcytic anemia, leukocytosis (21 800/μL), hyperbilirubinemia, elevated alkaline phosphatase (ALP), and gamma-glutamyl transferase (GGT). Prothrombin time (PT) was found to be prolonged and all inflammatory markers were high. To further investigate his symptoms, chest X-ray (CXR) and contrast-enhanced computed tomography (CT) scan of the chest and abdomen were performed. As demonstrated in Figure 1, CXR revealed evidence of right-sided pleural effusion, with opacification preserving the upper lobe. CT scans identified multiple hypodense lesions occupying the liver and extending to the pleural cavity and mediastinum, as illustrated in Figure 2. In addition, the terminal ileum wall was noted to be thickened with subsequent luminal narrowing, indicating a disease activity.
The diagnosis of pyogenic liver abscess with empyema and mediastinal cystic collection secondary to transdiaphragmatic and transhiatal extension was established, after isolating the organism
Multiple pigtail catheters were inserted under image guidance to drain pleural effusion and hepatic abscesses. Thereafter, the patient’s clinical status significantly improved and a marked decrease in abscess size was noted. However, several days later, the drain showed evidence of bile leakage, with more than 700 ml of fluid being drained for several consecutive days. A percutaneous transhepatic cholangiogram (PTC) showed evidence of hepatic abscess extension into the intrahepatic biliary ducts. Endoscopic retrograde cholangiopancreatography (ERCP) was then performed where the common bile duct (CBD) was cannulated and a 7×7 mm stent was inserted to reduce the pressure within the biliary tree. The follow-up CT scans of the chest and abdomen during week 3 of admission were obtained and, as Figure 3 illustrates, liver abscess and empyema exhibited a considerable reduction in size. Nevertheless, a chest tube was inserted and intrapleural fibrinolytic therapy was initiated when the patient developed dyspnea again with evidence of loculations on CXR. After 3 doses of tissue plasminogen activator (tPA), septations started to disappear except for 1 resistant loculation that had a thick wall. The patient’s clinical status significantly improved and he was discharged in good condition after 42 days of hospitalization.
CASE 2:
A 42-year-old man with unremarkable past medical history presented to the ER with abdominal pain and dyspnea of 1-day duration. At presentation, the patient was severely tachycardic, tachypneic, febrile, and hypertensive, necessitating immediate admission to the Intensive Care Unit (ICU) to restore his hemodynamic stability. Absence of air entry along with stoney dullness all over the right side of the chest were present on physical examination. Laboratory investigations revealed leukocytosis with WBCs exceeding 29 000/μL and lac-tate level of 9.67 mmol/L, indicating severe tissue hypoper-fusion. Inflammatory markers were markedly elevated, with C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) of 19.22 mg/dl and 106 mm/h, respectively. Additionally, a liver function test showed increased levels of direct bilirubin (1.3 mg/dL), ALP (612 U/L) and GGT (265 U/L). Acute renal failure was evident, with elevated serum creatinine and blood urea nitrogen (BUN) approaching 1.70 and 30 mg/dL, respectively. Moreover, his random blood glucose was 452 mg/dL.
CXR was performed and showed massive right-sided pleural effusion, with contralateral mediastinal shift, as shown in Figure 4. To explore the characteristics and etiology of pleural effusion, CT of the chest (Figure 5) was obtained, wherein the massive pleural effusion was found communicating with multiple multiloculated hepatic abscesses and causing complete collapse of the right lung. CT of the abdomen revealed details regarding the liver abscess, with the multiseptated hypodense lesions occupying segment IV, VII, and VIII of the liver, the largest measuring around 11.5×4.47 cm (Figure 6). These findings were suggestive of liver abscess with transthoracic extension resulting in empyema thoracis. Drainage of pleural and hepatic fluids yielded a purulent material that grew Klebsiella pneumoniae on culture, thus confirming the diagnosis of PLA. Hydatidosis, amebiasis, hepatitis, HIV, and tuberculosis were all ruled out. Further investigations regarding his persistent hyperglycemia confirmed the diagnosis of diabetes mellitus (DM), with a glycosylated hemoglobin of 11%.
Similarly, pleural collection and liver abscess were drained under radiological guidance. Pleural pigtail drained around 1 L of suppurative material on a daily basis within the first 10 days. Attempts to drain the pleural empyema via tube thoracostomy failed due to the presence of loculations. Therefore, the decision was made to perform surgical debridement via video-assisted thoracoscopic surgery (VATS). Upon exploration of the pleural cavity, extensive blood clots were found mixed with fresh blood. Complete drainage and debridement were performed and 2 chest tubes were inserted apically and basally. Fortunately, the patient demonstrated clinical improvement and was extubated 3 days postoperatively and was shifted to the general ward. However, his respiratory function did not return to baseline due to the presence of a fibrotic layer limiting maximum expansion of the right lung. Therefore, formal decortication through a posterolateral thoracotomy was carried out to free the lung. The patient improved dramatically thereafter and was discharged on postoperative day 5. Several days after discharge, he developed cholecystitis and underwent cholecystectomy.
CASE 3:
A 26-year-old man with a history of brucellosis 6 months before was transferred to our facility as a case of pleural empyema secondary to transdiaphragmatic extension of liver abscess. He initially presented with a 1-month history of progressive right-flank and RUQ pain associated with fever, chest pain, and shortness of breath. The patient also reported a history of unintentional weight loss of more than 20 kg since being diagnosed with brucellosis, which was treated with a full course of antibiotics. Moreover, his past medical history was significant for type 2 DM, hypertension, and dyslipidemia. A subcapsular hepatic collection was detected on CT and drained through a pigtail by the referring team. Following drainage, the patient developed hydropneumothorax and was managed via chest tube insertion. His clinical status failed to improve despite multiple antibiotic regimens and several drainage attempts; therefore, he was transferred to our facility to be managed by a specialized multidisciplinary team. Upon presentation, the patient was vitally stable apart from slight tachycardia and tachypnea. A physical examination revealed mild RUQ tenderness and a stoney dullness note of percussion over the right side of the chest.
His laboratory investigations revealed microcytic anemia and thrombocytosis along with elevated hepatic parameters and mild hypoalbuminemia. Inflammatory markers were significantly high, with CRP of 7.32 mg/dl and ESR of 114 mm/h. Some electrolyte abnormalities were also present, including hyperkalemia (5.6 mmol/L) and hyponatremia (125 mmol/L). As similarly encountered with case 2, the patient had uncontrolled DM with random blood glucose exceeding 430 and glycosylated hemoglobin of more than 11%.
A right hemithorax opacification was evident on a CXR performed upon admission. Furthermore, a contrast-enhanced CT of the abdomen showed a multiloculated hepatic lesion located along the posterior surface of the liver, measuring around 7.2×8.6 cm with thickening of the diaphragm and extension to the right pleural space. As shown in Figure 7, a contrast-enhanced CT of the chest confirmed the presence of a massive right-sided pleural effusion with multiple septations and subsequent atelectasis of the right lung, supporting the diagnosis of right-sided pleural empyema secondary to transdiaphragmatic extension of hepatic abscess. Echinococcus granulosus and Entamoeba histolytica titers were both low. A brucella-related collection was initially suspected based on elevated serological parameters, but the culture result did not support the diagnosis. Additionally, cultures of other bacterial pathogens were negative, probably due to initiation of empirical antimicrobial therapy before obtaining the sample.
After administering a broad-spectrum antibiotic and correcting electrolytes and blood glucose abnormalities, hepatic and pleural collection were performed. Unlike case 1 and 2, the management plan consisted of drainage of hepatic and pleural collections under radiological guidance only, without the need for intrapleural fibrinolytic therapy or surgical intervention. His condition significantly improved 3 days after drainage. A follow-up CT of the chest demonstrated marked regression in size of both hepatic and pleural collections. He was discharged in satisfactory condition after 10 days of admission, having the shortest hospital stay among the 3 discussed patients.
Discussion
Liver abscess is defined as a localized collection of suppurative material within the hepatic parenchyma [6]. As exemplified in the present cases, a clear male predominance exists among hepatic abscess patients, with males accounting for 72% of cases [7]. Based on the causative organism, hepatic abscess can be broadly classified into pyogenic and amebic entities. Although the 2 categories have some overlapping features, it is crucial to differentiate between them as the management and prognosis markedly differ [8]. Pyogenic forms, for example, tend to present as multiple lesions and have a polymicrobial origin [2,8].
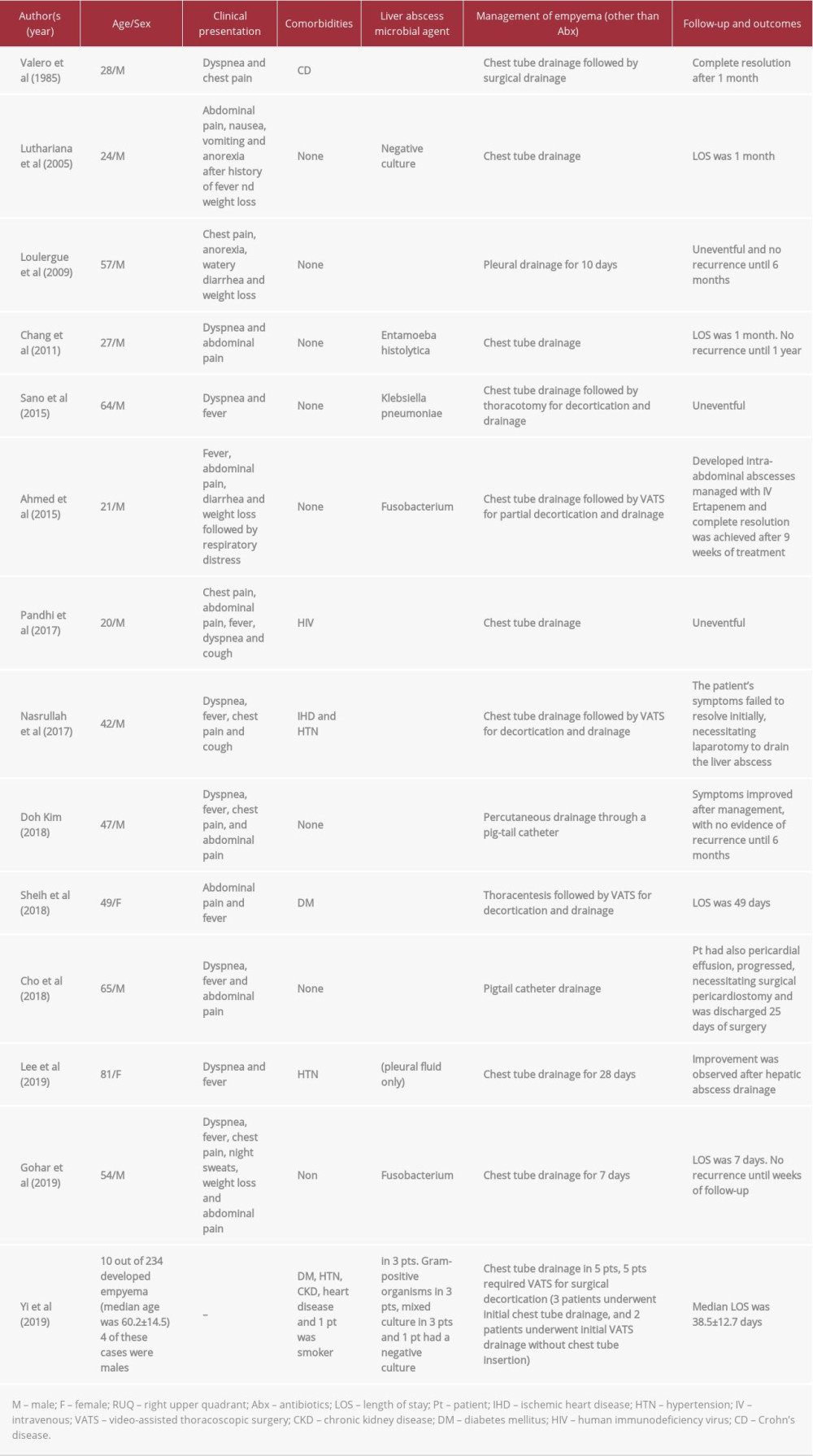
Anatomically, hepatic abscess has a right lobar preference, with 65% of cases involving the right lobe of the liver [12]. This observed preponderance can be simply explained by the rich blood supply delivered to the right hepatic lobe. The close proximity of hepatic lesions to diaphragmatic muscle makes extension of liver abscess and subsequent development of pleural empyema a possible complication, as demonstrated in the presented cases. Interestingly, an extensive review of the English literature revealed a total of 23 cases of pleural empyema secondary to transthoracic extension of liver abscess; only 1 of them was documented to be in a Crohn’s disease patient and none had concurrent mediastinal collection, highlighting the uniqueness of our first case. Table 1 compares the included cases in terms of patient presentation, causative agent, management approach, and outcome after intervention [4–6,13–23]. Another rare yet devastating complication of liver abscess was reported by Cho et al, where a 65-year-old man was diagnosed with pericarditis secondary to intrathoracic extension of left lobe hepatic abscess. Endophthalmitis, manifesting in a form of blindness and eye inflammation, has also been reported as one of the metastatic complications of PLA, with an incidence of 0.84–1.92% [24].
The etiology of pleural empyema varies widely and includes a range of benign and malignant conditions. Parapneumonic pleural effusion constitutes about 60% of all causations, followed by iatrogenic and traumatic cases [25]. Transdiaphragmatic extension of hepatic abscess is an extremely rare causative factor [20]. The evolving pattern of empyema has been represented in 3 distinctive stages to facilitate the decision regarding extent of intervention. The exudative stage is the first to appear and is characterized by the presence of fluid with low cellular content. This is followed by a fibrinopurulent phase which, as the name indicates, consists of fibrin deposits with apparent loculations. Last is the organized stage, where a pleural cortex presents, resulting in lung entrapment that subsequently jeopardizes the respiratory process, as encountered with our second case [26]. It is worth noting that pleural empyema was found to exert a negative impact on the prognosis of hepatic abscess; therefore, early detection and management are of paramount importance [4].
Several factors have been identified as predictors of development of metastatic infections secondary to liver abscess, including chronic alcoholism and DM, all of which were present among the 3 cases reported here [4]. Diabetes mellitus, in particular, was not only recognized as a significant predictor but also as a poor prognostic factor [22]. This might be attributed to the fact that diabetic patients are more prone to develop
It is not uncommon for Crohn’s disease to manifest with hepatobiliary-related complications [28]. The fistulizing, abscess-forming nature of CD, along with the induced immunocom-promised status, make CD patients 10–15 times more likely to develop hepatic abscess compared to the general population [29]. Translocation of the intestinal flora and subsequent dissemination through portal circulation is one of the hypothesized mechanisms of infection [30]. One of our cases was diagnosed with CD 2 months prior to the manifestation of liver abscess and had a classical picture of CD-associated hepatic abscess. Streptococcus species, specifically
Antimicrobial therapy and adequate drainage are the cornerstones of any pus collection treatment. The last decade has witnessed a paradigm shift in the management of hepatic abscess and pleural empyema, with surgery currently being the last resort. Studies addressing the management of pleural empyema as a transdiaphragmatic extension of liver abscess, in particular, are lacking. Based on our experience, we suggest percutaneous drainage with the help of interventional radiology, whenever feasible, as the initial method to manage thoracic empyema, combined with targeted antimicrobial therapy whenever applicable. Interventional radiology plays a pivotal role in managing similar cases, with valuable diagnostic and therapeutic applications. Pigtail catheter drainage is a safe, less invasive, alternative to the use of large-bore chest tubes [32]. A study by Jain et al showed comparable efficacy of pigtail catheter drainage to large-bore chest tube, with lower rates of morbidity [33]. Additionally, to achieve excellent prognosis, drainage of both hepatic and pleural collections is recommended. Despite the fact that both pus cavities might have direct communication, it is essential to drain thoracic empyema and hepatic abscess separately. Lee et al reported that empyema drainage alone was not sufficient to attain complete resolution [22]. When loculations are present, administration of intrapleural fibrinolytics can be an option. Growing evidence suggests the use of intrapleural fibrinolytic agents to reduce the requirement of surgical intervention, as in our first case. However, findings regarding the effectiveness of each substance remain controversial [34]. Generally, failure of standard therapy validates the decision of surgical intervention; therefore, management should be individualized based on the patient and treating physician [26]. When surgery is indicated, according to the American Association of Thoracic Surgery, VATS is preferred over open thoracotomy. The superiority of VATS stems from the associated lower rates of mortality and morbidity along with its cost-effectiveness compared to the open approach [35]. Future research should explore long-term outcomes related to the suggested approach to further assess its effectiveness.
Conclusions
Pleural empyema secondary to transdiaphragmatic extension of pyogenic liver abscess is a rare yet potentially lethal complication. The current report sheds light on one of the uncommon complications of liver abscess and contributes to this scarce field by summarizing pertinent literature. Early detection of thoracic empyema is essential to reduce rates of associated mortality and morbidity. Effective treatment requires a multidisciplinary, patient-tailored approach in which combined therapeutic modalities are utilized. Significantly, adequate drainage remains the cornerstone of any pus collection management despite the complexity of some encountered cases.
Figures
References:
1.. Togashi J, Sugawara Y, Akamatsu N: J Med Case Rep, 2013; 7; 36
2.. Heneghan HM, Healy NA, Martin ST, Modern management of pyogenic hepatic abscess: A case series and review of the literature: BMC Res Notes, 2011; 4; 80
3.. Malik AA, Pyogenic liver abscess: Changing patterns in approach: World J Gastrointest Surg, 2010; 2(12); 395-401
4.. Yi E, Kim TH, Lee JH, Evaluation of clinical risk factors for developing pleural empyema secondary to liver abscess: BMC Gastroenterol, 2019; 19(1); 215
5.. Cho E, Park SW, Jun CH, A rare case of pericarditis and pleural empyema secondary to transdiaphragmatic extension of pyogenic liver abscess: BMC Infect Dis, 2018; 18(1); 40
6.. Ahmed Z, Bansal SK, Dhillon S, Pyogenic liver abscess caused by Fusobacterium in a 21-year-old immunocompetent male: World J Gastroenterol, 2015; 21(12); 3731-35
7.. Kaplan GG, Gregson DB, Laupland KB, Population-based study of the epidemiology of and the risk factors for pyogenic liver abscess: Clin Gastroenterol Hepatol, 2004; 2(11); 1032-38
8.. Gaut D, Shull H, Bejjani A, Kahn D, Hepatic abscess in a returning traveler with Crohn’s disease: Differentiating amebic from pyogenic liver abscess: Case Rep Med, 2018; 2018; 9593865
9.. Pang TCY, Fung T, Samra J, Pyogenic liver abscess: An audit of 10 years’ experience: World J Gastroenterol, 2011; 17(12); 1622-30
10.. Neill L, Edwards F, Collin SM, Clinical characteristics and treatment outcomes in a cohort of patients with pyogenic and amoebic liver abscess: BMC Infect Dis, 2019; 19(1); 490
11.. Yin D, Ji C, Zhang S, Clinical characteristics and management of 1572 patients with pyogenic liver abscess: A 12-year retrospective study: Liver Int, 2021; 41(4); 810-18
12.. Serraino C, Elia C, Bracco C, Characteristics and management of pyogenic liver abscess: A European experience: Med (United States), 2018; 97(19); e0628
13.. Valero V, Senior J, Watanakunakorn C, Liver abscess complicating Crohn’s disease presenting as thoracic empyema. Case report and review of the literature: Am J Med, 1985; 79(5); 659-62
14.. Luthariana L, Lesmana L, Rubangi S, Management of pyogenic liver abscess and empyema as its complication: Indonesian Journal of Gastroenterology, Hepatology, and Digestive Endoscopy, 2005; 6; 22-26
15.. Loulergue P, Mir O, Pleural empyema secondary to amebic liver abscess: Int J Infect Dis, 2009; 13(3); 135-36
16.. Chang HR, Lee JJ, Bin Lin C, Pleural empyema secondary to rupture of amoebic liver abscess: Intern Med, 2012; 51(5); 471-74
17.. Sano A, Tsuchiya T: Pleura December, 2015; 2; 237399751559674
18.. Pandhi N, Gupta S, Singh A, Pandhi A, Amoebic liver abscess presenting as left empyema thoracis: Int J Curr Res Med Sci, 2017; 3(7); 52-55
19.. Nasrullah A, Haq S, Ghazanfar H, A unique case of empyema secondary to amoebic liver abscess: Cureus, 2017; 9(6); e1377
20.. Kim DH, Empyema caused by transdiaphragmatic extension of pyogenic liver abscess: Clin Case Reports, 2019; 7(1); 240-41
21.. Sheih YT, Wang CC, Empyema secondary to transdiaphragmatic extension of pyogenic liver abscess: Am J Med Sci, 2019; 357(1); e3
22.. Lee EJ, Lee KH, Kim JH: Medicine (Baltimore), 2020; 99(16); e19869
23.. Gohar A, Jamous F, Abdallah M, Concurrent fusobacterial pyogenic liver abscess and empyema: BMJ Case Rep, 2019; 12(10); e231994
24.. Park IH, Jun CH, Wi JW, Prevalence of and risk factors for endogenous endophthalmitis in patients with pyogenic liver abscesses: Korean J Intern Med, 2015; 30(4); 453-59
25.. Grijalva CG, Zhu Y, Nuorti JP, Griffin MR, The emergence of parapneumonic empyema in the United States: Thorax, 2011; 66(8); 663-68
26.. Redden MD, Chin TY, van Driel ML, Surgical versus non-surgical management for pleural empyema: Cochrane Database Syst Rev, 2017; 2017(3); CD010651
27.. Chuang C, Fan WC, Lin YT, Wang F: Gut Pathog, 2016; 8(1); 46
28.. Fousekis FS, Theopistos VI, Katsanos KH, Hepatobiliary manifestations and complications in inflammatory bowel disease: A review: Gastroenterol Res, 2018; 11(2); 83-94
29.. McGreal S, Sayers R, Wurm P, West K, Crohn’s disease presenting with pyogenic liver abscess: A case report: Case Rep Gastrointest Med, 2012; 2012; 762480
30.. Lin JN, Lin CL, Lin MC, Pyogenic liver abscess in patients with inflammatory bowel disease: A nationwide cohort study: Liver Int, 2016; 36(1); 136-44
31.. Margalit M, Elinav H, Ilan Y, Shalit M, Liver abscess in inflammatory bowel disease: Report of two cases and review of the literature: J Gastroenterol Hepatol, 2004; 19(12); 1338-42
32.. Rosenstengel A, Pleural infection-current diagnosis and management: J Thorac Dis, 2012; 4(2); 186-93
33.. Jain S, Deoskar RB, Barthwal MS, Rajan KE, Study of pigtail catheters for tube thoracostomy: Med J Armed Forces India, 2006; 62(1); 40-41
34.. Altmann ES, Crossingham I, Wilson S, Davies HR, Intra-pleural fibrinolytic therapy versus placebo, or a different fibrinolytic agent, in the treatment of adult parapneumonic effusions and empyema: Cochrane Database Syst Rev, 2019; 2019(10); CD002312
35.. Shen KR, Bribriesco A, Crabtree T, The American Association for Thoracic Surgery consensus guidelines for the management of empyema: J Thorac Cardiovasc Surg, 2017; 153(6); e129-46
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133