25 February 2022: Articles 
Autoimmune Hemolytic Anemia – Rare Complication of Brucellosis in a Saudi Woman: A Case Report and Literature Review
Challenging differential diagnosis, Educational Purpose (only if useful for a systematic review or synthesis), Rare coexistence of disease or pathology
Islam A. IbrahimDOI: 10.12659/AJCR.935187
Am J Case Rep 2022; 23:e935187






Abstract
BACKGROUND: Autoimmune hemolytic anemia and immune thrombocytopenia are rare complications of brucellosis; only a few cases have been reported in the literature. While pancytopenia is common and was reported in Saudi Arabia, the description of autoimmune hemolytic anemia or immune thrombocytopenia has not yet been reported in the kingdom. Hematological complication usually requires supportive treatment, and it is expected to improve with the initiation of antimicrobial therapy for brucellosis. There are few reports on the treatment of patients that fail to improve with conventional therapy.
CASE REPORT: A 46-year-old previously healthy Saudi woman was admitted to our hospital after multiple visits to the emergency department with chief concerns of fever and fatigability for 30 days. The examination was remarkable only for fever of 38.4°C and tender hepatomegaly. Laboratory tests upon admission were significant of pancytopenia, with a white blood count of 3×10⁹/L, hemoglobin of 8.1 g/dL, platelet of 13×10⁹/L, moderate hyponatremia, hypokalemia, and metabolic acidosis. Tuberculosis was ruled out and pan-sensitive brucellosis was diagnosed. She was started on standard antimicrobial therapy without significant improvement. Further testing revealed Coomb’s-positive hemolytic anemia and possible immune-mediated severe thrombocytopenia. She was treated with glucocorticoids and intravenous immunoglobulin, with dramatic response.
CONCLUSIONS: Autoimmune-mediated destruction of blood lines in brucellosis is rare. It should be sought as a potential diagnosis in case of persistent anemia and/or thrombocytopenia that is severe or fails to improve with proper antimicrobial coverage. Early involvement of hematologists and initiation of glucocorticoid with or without intravenous immunoglobulin is crucial.
Keywords: Anemia, Hemolytic, Autoimmune, brucellosis, Immunoglobulins, Intravenous, Thrombocytopenia, Anemia, Hemolytic, Female, Humans, Saudi Arabia
Background
Brucellosis, also known as Malta fever or Mediterranean fever, is a common zoonotic bacterial infection. It is caused by a gram-negative coccobacillus having several species; of them, B. melitensis and B. abortus affect humans most commonly. In 2006, brucellosis was estimated to account for 500 000 new cases each year worldwide [1]. In 2012, it was estimated to affect 12.5 new individuals per 100 000 population in Saudi Arabia alone. Nevertheless, the incidence rate varies from one region to another, with the highest rate reported in Al-Qassim, Aseer, Hail, Northern borders, and Najran. Males are more affected than females in Saudi Arabia [2,3].
Brucella species most commonly isolated in Saudi Arabia include B. melitensis followed by B. abortus; infection from other species in the kingdom has not yet been reported [2,4–6]. Brucellosis more commonly affects individuals of an occupation that revolves around animal handling and/or their products (eg, farmers and veterinarians). It is also considered as an occupational disease in health personnel working in microbiology labs [7]. The clinical presentation of brucellosis is extremely variable and can simultaneously affect many systems of the body. The onset of disease is either acute or insidious. The constitutional symptoms, including fever, appear in both acute and chronic infections; however, they are more frequent in acute infection. Fever occurs during the disease in almost all patients, and the osteoarticular system is most affected overall [8,9]. Hematological complications in the form of anemia, neutropenia, and thrombocytopenia occurring as monocytopenia are commonly observed. Autoimmune hemolytic anemia is a rare complication and tends to improve once proper antimicrobial therapy is initiated [2,10].
This paper presents the case of a 46-year-old Saudi woman who developed Coomb’s-positive brucellosis-induced autoimmune hemolytic anemia with markedly depressed platelet count that failed to improve with conventional antimicrobial therapy.
Case Report
A 46-year-old previously healthy Saudi woman was admitted through the emergency department with chief concerns of fever and fatigability for 30 days. The patient’s symptoms included productive cough with whitish sputum, night sweats, unintentional weight loss, decreased appetite, and joint pain involving both the knees and back. The patient had no history of similar presentations in the past, no history of travel, and no contact with animals or sick persons. The patient, however, gave a history of consuming home-made cheese from a popular local market. No significant past medical or surgical history was noted.
She appeared ill, pale, thin with body-mass-index (BMI) of 20 but did not show any symptoms of jaundice. Although the patient was febrile with a temperature of 38.4°C, her vital signs were stable, and she was breathing well. Head and neck examination revealed multiple petechiae on the lower lip. Cardiovascular examination was normal, the chest was clear to auscultation with no adventitious sounds; abdominal examination revealed right upper quadrant fullness and tender hepatomegaly. Musculoskeletal examination showed normal joints with no swelling or redness. The patient was admitted with fever of unknown origin. The pancytopenia was checked, and tuberculosis (TB) was ruled out.
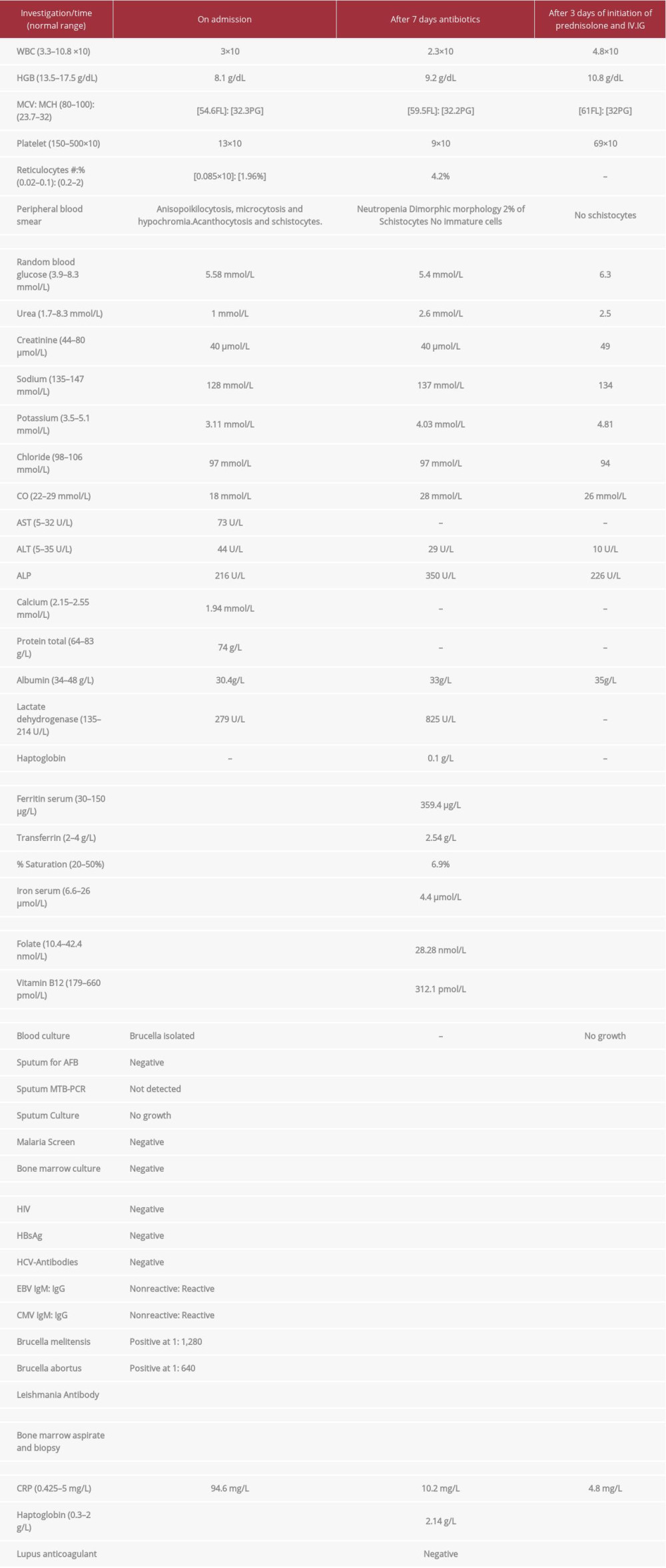
Initial investigations showed a white blood cell (WBC) count of 3×109/L, hemoglobin of 8.1 g/dL, platelet count 13×109/L, reticulocyte 1.96%; metabolic panel was significant for hyponatremia, i.e. sodium concentration was 128 mmol/L, Hypokalemia, i.e. serum potassium level was 3.1 mmol/L; metabolic acidosis with bicarbonate concentration 18 mmol/L; elevated liver enzymes with alanine aminotransferase (ALT) levels of 44 U/L; and aspartate aminotransferase (AST) levels of 72 U/L. A plain chest radiograph (CXR) was unremarkable. Abdominal ultrasound was performed for tender hepatomegaly, and it showed an enlarged liver measuring 21 cm, with decreased echogenicity, and an enlarged spleen measuring 11.3 cm in normal configuration.
Two blood cultures were collected, a sputum sample was subjected to acid-fast bacilli smear and culture, Mycobacterium Tuberculosis polymerase-chain-reaction assay (MTB-PCR), and general culture for bacteria. Malaria testing was done and viral serology for hepatotropic and non-hepatotropic viruses was also performed. The results are summarized in Table 1.
Empiric antibiotics were initiated, and 6 units of platelets were administered due to low platelet count with petechial hemorrhage on admission. The Hematology Department was consulted for the markedly depressed platelet count and methylmalonic acid was initiated. The initial impression was fever without localizing signs complicated with pancytopenia.
The patient continued to be febrile at 38.6°C despite the empiric antibiotics. On the third day of admission, contrast-enhanced CT of head, neck, thorax, abdomen, and pelvis was performed and showed multiple, bilateral, enlarged deep cervical lymph nodes; the largest noted on the left side, measuring about 1.5×0.7 cm; multiple, bilateral subcentimeter axillary lymph nodes; and normal lung tissues, bones, heart, pericardium, and pleura in contrast-enhanced CT-Neck & Thorax (Figure 1). The enlarged liver was 22.5 cm along the long axis, with heterogeneous nodular density. The enlarged spleen was 12.2×8 cm, with homogeneous density. Multiple prominent lymph nodes were noted in portocaval and aortocaval grooves, and mild intra-abdominal free fluid distinguished in the pelvic cavity in contrast-enhanced CT-abdomen (Figure 2).
Brucella serology was positive for B. melitensis and the patient was put on oral doxycycline therapy 100 mg twice daily and gentamicin 250 mg intravenously once daily for the most probable diagnosis.
Over the next few days, the patient showed modest clinical improvement, became more active, and presented a better appetite. The WBC count also showed partial improvement, but the hemoglobin and platelet count dropped to 7 g/dL and 11×109/L, respectively, on the sixth day of admission. Further, 4 units of platelets and 1 unit of packed red blood corpuscles (PRBCs) were transfused. Blood culture and sensitivity testing were done on the same day of the admission, and the culture confirmed pan-sensitive B. melitensis.
Worsening of anemia and thrombocytopenia despite adequate antimicrobial therapy necessitated further evaluation. Investigations revealed reticulocytosis of 4.2% and schistocytes on a peripheral bone smear (PBS). A bone marrow biopsy and aspirate were performed to define the etiology of the anemia and thrombocytopenia, and it demonstrated cellular marrow with increased megakaryocytic and prominent erythropoiesis with normal granulopoiesis, thus suggesting the possibility of peripheral destruction or consumption of cells (Figure 3). Direct Coomb’s test was positive and bone marrow aspirate culture grew pan-sensitive B. melitensis.
Glucocorticoids were initiated at 1 mg/kg/day (Prednisolone 50 mg orally once daily) for Brucella-induced autoimmune hemolytic anemia and possible immune thrombocytopenia. Platelet count and hemoglobin showed modest improvement, with platelets rising to 23x109/L after 3 days. However, the patient’s general condition deteriorated. After reviewing the available literature, a multidisciplinary team comprising physicians from hematology, infectious disease, and internal medicine, decided to replace gentamicin with streptomycin and initiate intravenous immunoglobulin (IVIg) in addition to the corticosteroid. Informed consent was obtained from the patient and her family. Intravenous immunoglobulin 50 gm once daily was initiated in addition to prednisolone 50 mg orally once daily. After 3 days of the combination therapy, the patient’s general condition stabilized, and the platelet count rose to 67×109/L. She was discharged with doxycycline 100 mg orally to be consumed twice daily: streptomycin 500 mg intramuscular to be taken twice daily to complete 14 days: and prednisolone 50 mg orally once daily with tapper after reassessment in the clinic.
The patient reported to the clinic 2 months after finishing the antibiotic course. She showed remarkable clinical improvement, her symptoms had diminished, and she had a good appetite and gained proper weight. Her complete blood count showed stable hemoglobin 13 g/dL, WBC count of 11.4×109/L, and platelet count of 271×109/L. Repeated Brucella serology showed titre of <1: 80 for both the strains, B. melitensis and B. abortus.
Discussion
Brucella continues to be a major health concern, even though its incidence is decreasing steadily. This can be attributed to the mandatory governmental requirement of immunization of cattle against Brucella and control of livestock imported from outside the kingdom. Despite all efforts, it remains an endemic zoonotic disease in Saudi Arabia [11–13]. The varying, non-specific, manifestation of this disease poses a challenge for early and proper diagnosis, which in turn increases the disease burden. Hematological complications like anemia and neutropenia, which are common, have been frequently reported. In contrast, autoimmune hemolytic anemia and severe thrombocytopenia are rare; when they occur, they tend to be the result of a complication of melitensis species, with an estimated frequency of 5.8% to 14.8% [14–17].
The implicated pathophysiology of hematological complications in brucellosis includes hypersplenism, bone marrow suppression, altered iron metabolism secondary to an infection, thrombotic microangiopathy, and autoimmune hemolysis. Another explanation is reactive hemophagocytosis, first described by Zuazu et al in 1979 [16] and also reported in Saudi Arabia by Elzein et al [18] in 2018. Nevertheless, autoimmune hemolysis is considered a rare complication, with very few cases reported with a positive Coomb’s test [19]. The bone marrow aspirate of the patient in the present case was highly suggestive of peripheral destruction and/or consumption, ruling out bone marrow suppression as the primary mechanism for pancytopenia. The patient presented with radiographic splenomegaly – a plainly enlarged spleen in radiograph, with a spleen length of more than 12 cm – but it was not palpable in clinical examination. This made hypersplenism as a cause of pancytopenia unlikely. However, it must be noted that brucellosis is a common infectious cause of splenomegaly and hypersplenism [16].
A positive Coomb’s test made the diagnosis of immune-mediated destruction more likely. Unfortunately, specific anti-platelet antibodies testing could not be performed, even though negative results would not rule out the diagnosis of immune thrombocytopenia. Failure of blood counts to depict characteristic findings of microangiopathic hemolysis made the thrombotic microangiopathy unlikely. Severe anemia that is failing to improve despite adequate antibiotic in the patient could only be explained by the immune-mediated destruction, although the destruction affected platelets more than RBCs.
In general, most brucellosis-induced complications, including hematological complications, usually resolve with the initiation of anti-Brucella treatment [15]. The time needed for improvement of each complication varies. In this case, pancytopenia was expected to show signs of improvement at the end of the induction phase. However, the cell count in this patient failed to increase and, instead, the platelet count and hemoglobin remained extremely low. The decision to initiate corticosteroid (prednisolone) therapy was supported by cases reported by Pappas et al [20], Sari et al [21], Bourantas et al [22], Eskazan et al [23], and Abdallah TM et al [24], who successfully treated autoimmune hemolytic anemia and immune thrombocytopenia associated with Brucella using steroids. The evidence behind the concomitant use of steroids and IVIg for the treatment of autoimmune hemolytic anemia and immune thrombocytopenia associated with Brucella that failed to improve on adequate antimicrobial therapy is scarce but showed an excellent result. The clinical outcomes observed in the case reports and the patient’s enthusiasm to embrace the possibility of improvement with the proposed therapy, encouraged the authors to proceed with this uncommon therapy [20,24–26]. The authors recommend the use of IVIg in addition to corticosteroid and the standard antimicrobial therapy for Brucella-induced autoimmune hemolytic anemia and/or immune thrombocytopenia, which must be initiated right from the time of diagnosis of severe immune thrombocytopenia (<10 000) and/or evidence of severe autoimmune hemolysis.
Conclusions
Brucellosis continues to be an endemic infection in many regions of Saudi Arabia. It should be sought as a potential diagnosis in febrile patients without localizing signs.
Autoimmune destruction of red blood corpuscles and/or platelet, although a rare complication, should be strongly considered in the differential diagnosis of cytopenia in patients with brucellosis that failed to improve with initiation of appropriate antimicrobial therapy.
A multidisciplinary team comprising experts in hematology and/ or tropical medicine specialists must be consulted and corticosteroids along with IVIg should be considered in Brucella-induced autoimmune hemolytic anemia and/or severe immune thrombocytopenia <10 000. In less severe cases where appropriate antimicrobial therapy has failed, corticosteroids and IVIg may be considered.
Figures
References:
1.. Pappas G, Papadimitriou P, Akritidis N, The new global map of human brucellosis: Lancet Infect Dis, 2006; 6(2); 91-99
2.. Aloufi AD, Memish ZA, Assiri AM, McNabb SJN, Trends of reported human cases of brucellosis, Kingdom of Saudi Arabia, 2004–2012: J Epidemiol Global Health, 2016; 6(1); 11-18
3.. Anazi M Al, AlFayyad I, AlOtaibi R, Abu-Shaheen A, Epidemiology of brucellosis in Saudi Arabia: Saudi Med J, 2019; 40(10); 981-88
4.. Kambal1 AM, Mahgoub ES, Jamjoom GA, Chowdhury MNH, Brucellosis in Riyadh, Saudi Arabia. A microbiological and clinical study: Trans R Soc Trop Med Hyg, 1983; 77(6); 820-24
5.. Al-Eissa YA, Brucellosis in Saudi Arabia: Past, present and future: Ann Saudi Med, 1999; 19(5); 403-5
6.. Kiel FW, Yousuf Khan M, Analysis of 506 consecutive positive serologic tests for brucellosis in Saudi Arabia: J Clin Microbiol, 1987; 25(8); 1384-87
7.. Alkahtani AM, Assiry MM, Chandramoorthy HC, Sero-prevalence and risk factors of brucellosis among suspected febrile patients attending a referral hospital in southern Saudi Arabia 2014–2018: BMC Infect Dis, 2020; 20(1); 26
8.. Colmenero JD, Reguera JM, Martos F: Medicine, 1996; 75(4); 195-211
9.. Rizvi Z, Iqbal T, Bokhary H, Chaudhry S, Brucellosis: An elusive backyard agent: Cureus, 2020; 12(5); e8154
10.. Kaya S, Elaldi N, Deveci O, Eskazan AE, Cytopenia in adult brucellosis patients: Indian J Med Res, 2018; 147(1); 73
11.. , Livestock market replete with sheep and cattle for Adahi – Saudi Gazette (accessed October 22, 2021)https://saudigazette.com.sa/article/62836
12.. Jokhdar Habde A, Brucellosis in Saudi Arabia: Review of literature and an alarming case report in a hospital in Jeddah: Med J Cairo Univ, 2009; 77(3); 47-55
13.. Al Ali AM, Alluwaimi AM, The incidents of human brucellosis in Al-Ahsaa area, Saudi Arabia: Scientific Journal of King Faisal University (Basic and Applied Sciences), 2009; 10(2); 115
14.. Karakukcu M, Patiroglu T, Ozdemir MA, Pancytopenia, a rare hematologic manifestation of brucellosis in children: J Pediatr Hematol Oncol, 2004; 26(12); 803-6
15.. Al-Eissa YA, Assuhaimi SA, Al-Fawaz IM, Pancytopenia in children with brucellosis: Clinical manifestations and bone marrow findings: Acta Haematol, 1993; 89(3); 132-36
16.. Lynch EC, McKechnie JC, Alfrey CP, Brucellosis with pancytopenia: Ann Intern Med, 1968; 69(2); 319-22
17.. Akbayram S, Dogan M, Akgun C, An analysis of children with brucellosis associated with pancytopenia: Pediatr Hematol Oncol, 2011; 28(3); 203-8
18.. Elzein FE, Sherbini N Al, Alotaibi MM, Al-Hassan WM, Brucellosis accompanied by haemophagocytic lymphohistiocytosis and multiple splenic abscesses in a patient with depression: BMJ Case Rep, 2018; 2018; bcr2017224018
19.. Meena DS, Sonwal VS, Rohila AK, Meena V, Acute brucellosis presenting as an autoimmune hemolytic anemia: Case Rep Infect Dis, 2018; 2018; 1030382
20.. Pappas G, Kitsanou M, Christou L, Tsianos E, Immune thrombocytopenia attributed to brucellosis and other mechanisms of Brucella-induced thrombocytopenia: Am J Hematol, 2004; 75(3); 139-41
21.. Sari I, Kocyigit I, Altuntäs F, Kaynar L, Eser B, An unusual case of acute brucellosis presenting with Coombs-positive autoimmune hemolytic anemia: Internal medicine (Tokyo, Japan), 2008; 47(11); 1043-45
22.. Bourantas LK, Pappas G, Kapsali E, Brucellosis-induced autoimmune hemolytic anemia treated with rituximab: Ann Pharmacother, 2010; 44(10); 1677-80
23.. Eskazan AE, Dal MS, Kaya S, Dal T, Two cases of autoimmune hemolytic anemia secondary to brucellosis: A review of hemolytic disorders in patients with brucellosis: Intern Med, 2014; 53(11); 1153-58
24.. Abdallah TM, Abd Elbagi OM, OsmanKaroum A, Abdallah Ali AA, Acute brucellosis as unusual cause of immune thrombocytopenia: A case report and review of the literature: Asian Pac J Trop Biomed, 2014; 4(9); 751-54
25.. Sevinc A, Buyukberber N, Camci C, Thrombocytopenia in brucellosis: case report and literature review: J Natl Med Assoc, 2005; 97(2); 290
26.. Xie S, Zhou Y, Zheng R, Brucella-induced thrombocytopenia: A retrospective study of 16 patients: J Int Med Res, 2019; 47(7); 3008
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report  22,760,204
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133