10 April 2022: Articles 
A 60-Year-Old Swiss Woman Presenting with Migratory Radicular Pain Diagnosed with Lyme Disease by Western Blot
Unusual clinical course, Challenging differential diagnosis
Gisela Marcelino1BCDEF*, João Cerveira2DEF, André Teychené1DEF, Armand Eichenberger1DEFDOI: 10.12659/AJCR.935717
Am J Case Rep 2022; 23:e935717






Abstract
BACKGROUND: Many diagnostic guidelines have been established to support the diagnosis of Lyme disease, but a recent meta-analysis did not find that 2-tier tests were better than individual tests. Here, we present the case of a patient who was diagnosed by immunoblot only, a second-line test that is usually not performed if the first-line test is negative.
CASE REPORT: A 60-year-old Swiss woman, without relevant comorbidities, presented to our clinic with 1-week symptoms of migratory radiculitis in the L1, L2, and L5-S1 right dermatomes. Blood analysis and lumbar and brain MRI did not show any significant abnormalities. However, unexpected results were obtained after testing Lyme serologies. They were performed first with LIAISON® test (Diasorin, Italy) then with Borrelia VIRAstripe® immunoblot (Viramed, Germany) and a positive IgM result was only obtained with the latter. Consequently, doxycycline 100 mg 2×/day was initiated and the symptoms completely resolved after 6 weeks of treatment. Ever since, and more than 1 year after the initial presentation, the patient remains symptom-free.
CONCLUSIONS: As shown, it was possible to diagnose this patient and treat her successfully by testing all the available serologies. Furthermore, we were surprised to find out after a review of the literature that the IgM sensitivity in neuroborreliosis with the LIAISON® test is only 43.9-46% versus 90-100% with VIRAstripe®. Hence, clinicians need to understand the pitfalls of these tests before excluding Lyme disease.
Keywords: Blotting, Western, Enzyme-Linked Immunosorbent Assay, Fluorescent Antibody Technique, Indirect, Immunoblotting, Lyme Disease, Lyme Neuroborreliosis, Antibodies, Bacterial, Female, Humans, Immunoglobulin G, Immunoglobulin M, Pain, Switzerland
Background
Switzerland is known to be an endemic region for tick-borne diseases, particularly for Lyme disease, where up to 50% of ticks in certain Swiss regions are infected with
Lyme disease is characterized by 3 stages [3]. The first stage is characterized by the pathognomonic cutaneous rash – the erythema migrans. The second stage leads to symptoms that frequently mimic influenza [3]. The third stage is associated with arthritis, heart disease, acrodermatitis chronica atrophicans, or neurological disease [3]. In Europe, the most frequent neurological presentation of
The diagnosis of Lyme disease is clinical, especially in stage 1, where no serological testing is usually necessary. However, in stages 2 and 3, serological testing may be useful to support its diagnosis. The first recommended serological test is usually the ELISA (enzyme-linked immunoassay) test or, less commonly, the IFA (indirect immunofluorescence assay) test [5]. Both detect antibodies to
Here, we report an unusual case of a patient who presented with peripheral radiculitis secondary to Lyme disease and who was diagnosed by western blot only.
Case Report
A 60-year-old Swiss woman, previously diagnosed with prediabetes and a mitral valve prolapse, without any regular medication, presented to our clinic on 3 June 2020 with symptoms of intermittent migratory polyneuropathy in the L1, L2, and L5–S1 right dermatomes. She reported a feeling like an electrical current that started on her lumbar area and then radiated down her right lower limb over the right inguinal area, proximal antero-lateral region of the thigh, and the lateral part of the lower limb up to the foot. The symptoms had started 1 week earlier, manifested in an intermittent fashion, and the patient did not recall having been bitten by a tick or having had erythema migrans. There was also no history of chronic lumbar pain, recent lumbar traumatism, typical infectious symptoms, B symptoms, symptoms compatible with vasculitis, intermittent claudication, other neurological symptoms, or symptoms of psychological distress. The patient also denied having received a vaccine or any other medication before the start of the symptoms. She also denied having been exposed to toxic chemicals, having had a sexual risk behavior, or having traveled abroad. The patient has a high level of education, works as a magistrate and lives in a rural area of Switzerland.
The clinical examination was unremarkable during the initial and following visits to our clinic.
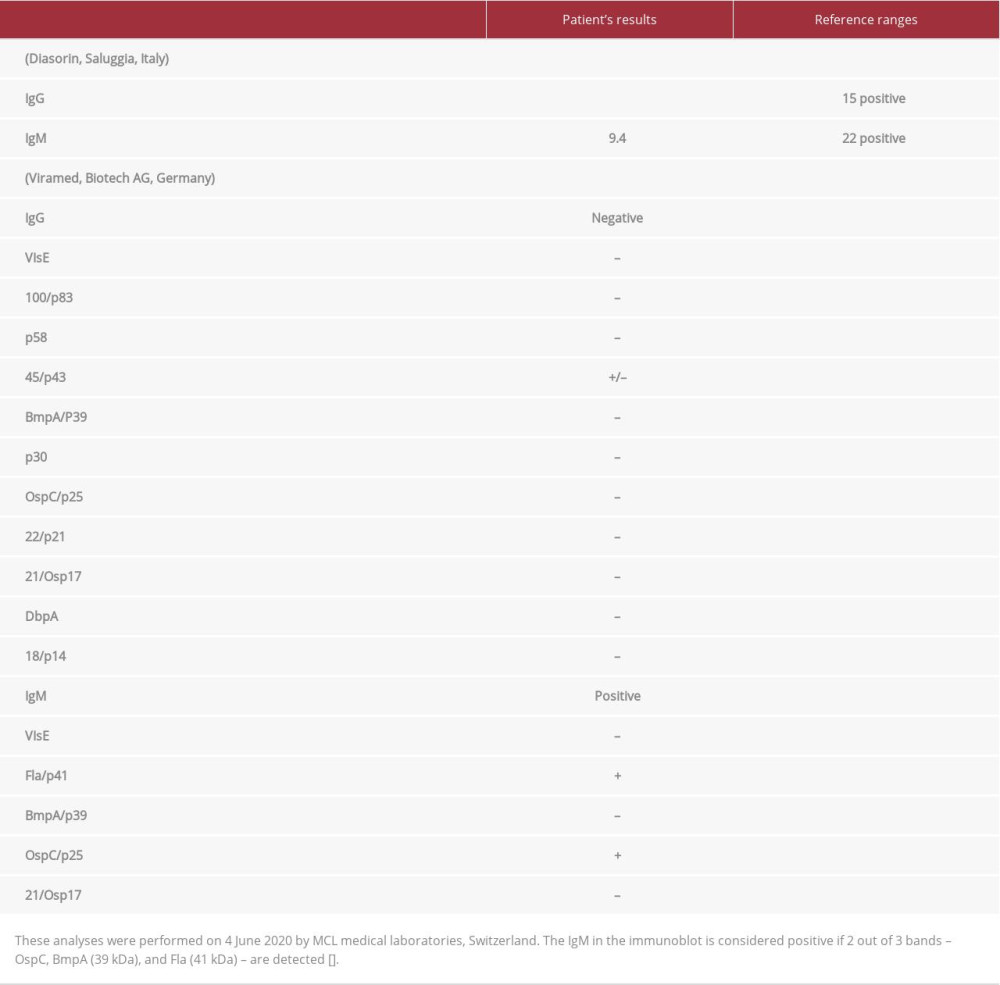
The blood analysis did not show any inflammatory syndrome, as the C-reactive protein was 0 mg/L and the erythrocyte sedimentation rate was 4 mm/h. There were no hematological disturbances. The kidney and the liver tests were normal. A protein electrophoresis was normal without any signs of paraproteinemia. There were also no signs of electrolytical imbalances and a urine test strip result was normal. Since Switzerland is an endemic region for Lyme disease, this disease was therefore screened and the results of the serological tests are presented in Table 1.
A lumbar and brain MRI did not show any signs for a demyelinating or an inflammatory disease and the lumbar MRI excluded significant discopathy. The lumbar MRI reported only a discrete discopathy in D12–L1, no anomaly at the level of L1–L2, a moderate discopathy with a diffuse disk hernia without signs of radicular compression at the level of L2–L3, a discrete discopathy in L3–L4, a lumbar canal stenosis at the level of L4–L5 associated with a diffuse herniated disk and foraminal stenosis of both sides and radicular irritation of L4 on both sides, and finally no abnormality of the L5–S1 disk. The brain MRI reported a little signal anomaly (FLAIR hypersignal) of 3 mm in the deep white matter of the left temporoparietal region, considered as totally unspecified. Of note, the MRI had to be performed without gadolinium because the patient was highly allergic to it.
As the results of the serology for Lyme disease came out positive on 4 June 2020, particularly the immunoblot (Table 1), the patient was started on doxycycline 100 mg 2×/day for 1 month, and the neuropathic symptoms progressively subsided and completely disappeared. On 1 July 2020, the patient reported another and unique episode of pain over the L1 and L2 right dermatomes. Therefore, the antibiotic doxycycline 100 mg 2×/day was empirically continued for another 2 weeks and then stopped. It is also important to mention that the patient did not take any other medication during this period in addition to the antibiotic, and to date the patient is symptom-free.
Discussion
Here, we report a case of peripheral radiculitis secondary to Lyme disease, which is the most frequent neurological manifestation of this disease in Europe [3,4]. It is also known that peripheral radiculitis due to Lyme disease can be the result of a mononeuropathy multiplex, a plexopathy, or a radiculoneuritis. But as an electromyographic study was not performed in our patient, and as the MRI did not show any inflammatory signs compatible with neuritis, we are not able to confirm which 1 of the 3 types of peripheral radiculitis described above our patient presented. However, not all Lyme patients with peripheral neuropathy have abnormal electromyograms, since there are cases reported with normal findings [10]. A spinal tap was not performed since, according to the recommendations of the Swiss Society for Infectious Diseases, a cerebrospinal analysis is not necessary in the case of a peripheral neuropathy secondary to Lyme disease [7]. A demyelinating disease could also be excluded since unenhanced MRI has similar accuracy as gadolinium-based contrast for the diagnosis of demyelinating diseases, including multiple sclerosis [11].
The authors are aware that the western blot test is usually not recommended in current guidelines as a first-line test and neither as a second-line test if the ELISA or the IFA is negative [5–7]. Nevertheless, during our search of the literature, we were surprised to find that the even though the overall sensitivities of those tests are quite good, the individual sensitivities of IgG and IgM according to the stage of Lyme disease are significantly different [12–14]. Moreover, the sensitivities also differ according to the technique employed by the laboratory that performs the tests, which could have a negative clinical impact [12–16]. For instance, the LIAISON® test (Diasorin, Saluggia, Italy), a type of indirect chemiluminescence immunoassay that has been shown to outperform IFA test in Lyme disease [13] and which was performed in our patient by the laboratory MCL® medical laboratories in Switzerland, has an overall sensitivity of 98% in patients with neuroborreliosis, while IgM only has a sensitivity of 43.9–46% for neuroborreliosis [14,16]. Conversely, the sensitivity levels of the
The authors are also aware that positive IgM or IgG may be secondary to cross-reactivity to other circulating antibodies or may be a serological scar secondary to a previous infection with
Conclusions
We demonstrate here that a second-tier test can also be helpful to diagnose Lyme disease even though the first-tier test was negative, particularly in a patient from an endemic region for this disease and in whom there is a high clinical suspicion. Clinicians therefore need to understand the pitfalls of Lyme serological tests, since they have different sensitivities and specificities according to the stage of the disease and to the type of test that is performed.
References:
1.. , [Borreliosis/Lyme disease.] Available from: . Last update 22 November 2019Accessed 15 August 2020. [in French]https://www.bag.admin.ch/bag/fr/home/krankheiten/krankheiten-im-ueberblick/borreliose-lyme-krankheit.html
2.. , [Tick-borne diseases – Situation in Switzerland.] Available from: . Last update 12 August 2019. Accessed 15 August 2020. [in French]https://www.bag.admin.ch/bag/fr/home/krankheiten/ausbrueche-epidemien-pandemien/aktuelle-ausbrueche-epidemien/zeckenuebertragene-krankheiten.html
3.. Marques AR, Strle F, Wormser GP, Comparison of Lyme disease in the United States and Europe: Emerg Infect Dis, 2021; 27(8); 2017-24
4.. Ogrinc K, Lusa L, Lotrič-Furlan S, Course and outcome of early European Lyme neuroborreliosis (Bannwarth syndrome): Clinical and laboratory findings: Clin Infect Dis, 2016; 63(3); 346-53
5.. Talagrand-Reboul E, Raffetin A, Zachary P, Immunoserological diagnosis of human borrelioses: Current knowledge and perspectives: Front Cell Infect Microbiol, 2020; 10; 241
6.. Lantos PM, Rumbaugh J, Bockenstedt LK, Clinical practice guidelines by the Infectious Diseases Society of America (IDSA), American Academy of Neurology (AAN), and American College of Rheumatology (ACR): 2020 Guidelines for the prevention, diagnosis, and treatment of Lyme disease: Arthritis Rheumatol, 2021; 73(1); 12-20
7.. Lyme borreliosis: Epidemiology and . Accessed February 20, 2022https://www.sginf.ch/files/summary_part__1.pdf
8.. Leeflang MM, Ang CW, Berkhout J, The diagnostic accuracy of serological tests for Lyme borreliosis in Europe: A systematic review and meta-analysis: BMC Infect Dis, 2016; 16; 140
9.. Molins CR, Delorey MJ, Sexton C, Schriefer ME, Lyme borreliosis serology: Performance of several commonly used laboratory diagnostic tests and a large resource panel of well-characterized patient samples: J Clin Microbiol, 2016; 54; 2726-34
10.. Halperin JJ, Little BW, Coyle PK, Dattwyler RJ, Lyme disease: Cause of a treatable peripheral neuropathy: Neurology, 1987; 37(11); 1700-6
11.. Eichinger P, Schön S, Pongratz V, Accuracy of unenhanced MRI in the detection of new brain lesions in multiple sclerosis: Radiology, 2019; 291(2); 429-35
12.. , Product Information: Differentiated borrelia diagnostics – all screening and and confirmatory tests from one source. Euroimmun. Medizinische Labordiagnostika AG Available from:. Accessed January 1, 2022https://www.euroimmun.com/documents/Indications/Infections/Borrelia/HI_2132_I_UK_C.pdf
13.. Cerar T, Ruzic-Sabljic E, Cimperman J, Strle F, Comparison of immunofluorescence assay (IFA) and LIAISON in patients with different clinical manifestations of Lyme borreliosis: Wien Klin Wochenschr, 2006; 118; 686-90
14.. , Product Information: Borrelia burgdorferi IgG, IgM fully automated chemiluminescence assays for an accurate detection of IgG and IgM antibodies to Borrelia Burgdorferi. DiaSorin Available from: . Accessed August 27, 2020https://www.diasorin.com/sites/default/files/allegati_prodotti/borrelia_m0870004179_c_borrelia_m0870004177_d.pdf
15.. Marangoni A, Sparacino M, Mondardini V, Comparative evaluation of two enzyme linked immunosorbent assay methods and three Western Blot methods for the diagnosis of culture-confirmed early Lyme borreliosis in Italy: New Microbiol, 2005; 28(1); 37-43
16.. Dessau RB, Diagnostic accuracy and comparison of two assays for Borrelia-specific IgG and IgM antibodies: proposals for statistical evaluation methods, cut-off values and standardization: J Med Microbiol, 2013; 62(Pt 12); 1835-44
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133