02 April 2022: Articles 
Infective Endocarditis Caused by in a Pediatric Patient: A Case Report and Literature Review
Rare disease
Abdulbary Ali Alhalimi1EF, Lateefah Talal AlShammari2BE, Ahmed Khalid Al-QuraynDOI: 10.12659/AJCR.935743
Am J Case Rep 2022; 23:e935743






Abstract
BACKGROUND: Pseudomonas luteola (P. luteola) is a Gram-negative, oxidase-negative is an environmental organism that is isolated from soil, water, and damping areas, and is rarely found as a human pathogen. Most infections in which P. luteola is implicated are associated with a breach in immune barrier, such as indwelling catheters, prosthetic devices, immunocompromised conditions and surgical wounds.
CASE REPORT: A 9 years old girl, known case of Chron’s disease and recurrent urinary tract infections on prophylactic antibiotics, presented with an acute-onset abdominal pain associated with fever reaching 40C and vomiting. She was placed on a peripherally inserted central line for total parenteral nutrition and developed sepsis on the 30th day of admission. Septic workup revealed P. letuola infection with right atrial vegetation. Treatment with Piperacillin/tazobactam yielded an uneventful recovery.
CONCLUSIONS: P. luteola can be involved in serious infections in susceptible individuals. Serious outcomes may be associated with infective endocarditis especially on a background of valvular prosthesis and central lines. The definitive treatment of catheter related infective endocarditis caused by P. leuteola is the removal of the lines along with an appropriate antibiotic regimen-based AST result.
Keywords: Endocarditis, Bacterial, Piperacillin, Tazobactam Drug Combination, Pseudomonas luteola, central venous catheters, Child, Endocarditis, Female, Humans, Pseudomonas
Background
Case Report
PAST HISTORY:
A nine-year-old girl known to have Crohn’s disease with enteroenteric and entero-vesical fistulae presented to the Emergency Department reporting acute onset of lower abdominal pain accompanied with fever and non-bilious vomiting. The pain was mainly in the left iliac fossa, scoring 9/10 in severity. She had a documented history of chronic on-off abdominal pain. There was no change in bowel habits or change in urine frequency or any genitourinary tract symptoms. No upper respiratory tract symptoms were documented. She was diagnosed with Crohn’s disease 1 year prior to her current presentation; her first presentation was in 2018 in the form of acute appendicitis, for which she underwent a laparoscopic appendectomy complicated by a polymicrobial pelvic abscess (
The patient was doing well until her 14th day of admission, when a PICC line was inserted to initiate total parenteral nutrition (TPN) due to Crohn’s disease flare.
PRESENT ILLNESS:
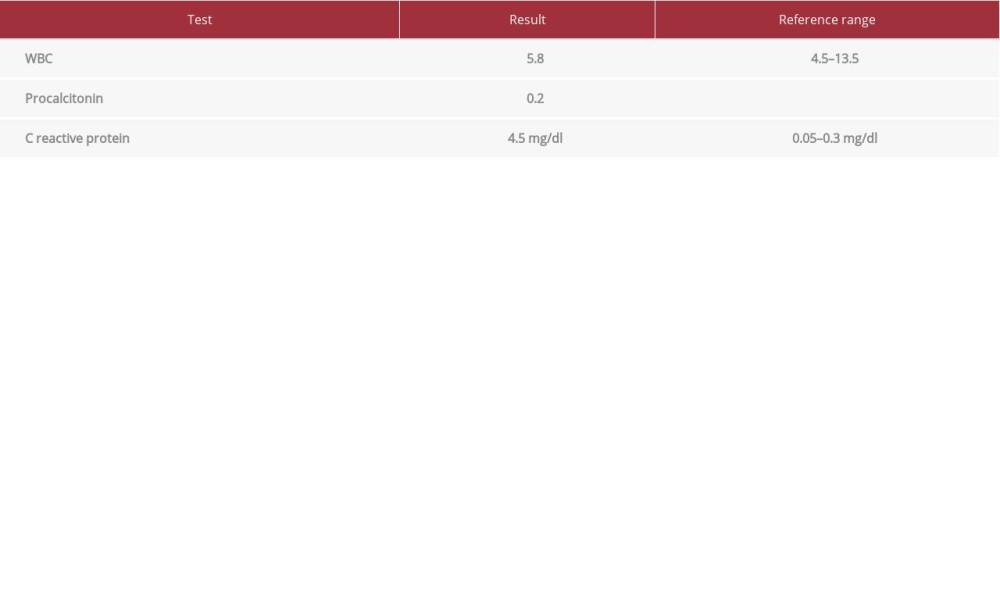
On the 30th day of admission, her temperature rose to 40°C with marked pallor, tachycardia, and tachypnea, associated with malaise and fatigue. A septic workup was done (results are shown in Table 1). Furthermore, 3 sets of blood cultures collected from the PICC line and a catheter tip culture were sent for laboratory analysis on 3 consecutive days.
MICROBIOLOGY LABORATORY FINDINGS:
All of the 3 sets of blood cultures vials were incubated in the BacT/Alert Virtuo system (BioMérieux, France) for a total of 5 days, and the PICC line tip culture was inoculated by rolling the tip technique across a sheep blood agar and incubating at 37°C, according to the internal policies and procedures of the microbiology laboratory at King Fahd Hospital of the University. After 24 h of incubation of the blood culture sets, all blood culture vials flagged positive, and direct gram stain showed Gram-negative bacilli. Subsequently, blood vials were sub-cultured to sheep blood agar, MacConkey agar, chocolate agar, and anaerobic blood agar. Overnight incubation showed heavy growth of wrinkled small yellow colonies in the sheep blood agar and non-lactose-fermenting colonies in MacConkey agar. The gram stain from cultured colonies showed small Gram-negative rods. Results of the oxidase test were negative. The isolate was identified as
TREATMENT AND OUTCOME:
The regimen was shifted to piperacillin/tazobactam 2.3 g i.v. every 8 h and continued for 6 weeks. Upon discharge, repeated echo showed resolved vegetation; the patient clinically improved with stable vital signs and the recovery was uneventful.
Discussion
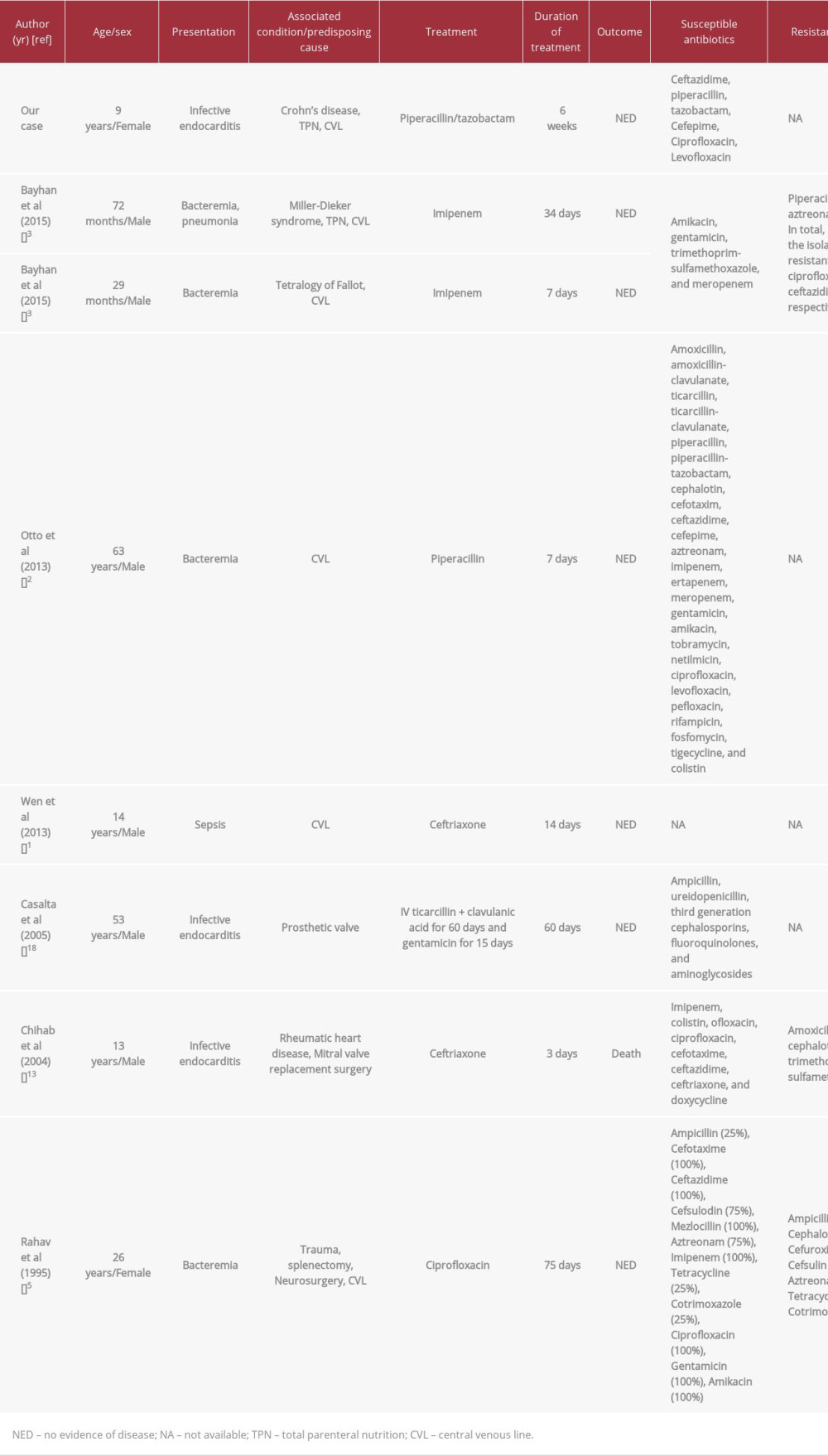
Most cases involving P. luteola are found in individuals with predisposing factors such as the presence of a PICC line [1–3], TPN [3], continuous ambulatory peritoneal dialysis (CAPD) [4–7], trauma [5,8,9], mechanical ventilation [MV] [3,10,11], surgery [12–15], or immunocompromised state [10,13,14,16,17]. As presented in Table 2, reports on infective endocarditis were associated with the presence of a central venous line (CVL), prosthetic heart valve, rheumatic heart disease, or previous heart surgery [1–3,5,13,18]. Out of 8 cases of P. luteola infection connected with CVL, 3 were of infective endocarditis, including the case reported in this article, and only 1 case (reported by Chihab et al) was fatal [1–3,5,18].
In the present case, the definitive treatment was piperacillin/tazobactam, which was given based on the susceptibility tests. Different antibiotic regimens were reported in other cases, including imipenem, ceftriaxone, ticarcillin, gentamicin, and ciprofloxacin. This difference may be due to varying clinical approaches, antimicrobial susceptibility patterns, or the availability of antibiotics in each facility.
The median duration of treatment of patients with infective endocarditis who had uneventful recovery was 34 days (minimum of 7 days, maximum of 75 days) [1–3,5,18]. Rahav et al and Casalta et al found that patients with valvular prosthesis had a longer duration of recovery (average of 67.5 days), compared to patients with CVL (20.8 days), and Chihab et al reported a case with a prosthetic valve that resulted in death [5,13,18], which might be a prognostic factor for cases with a prosthetic valve. Furthermore, the definitive treatment of cases with positive cultures of the CVL tip, besides the appropriate antibiotics, was removal of the catheter regardless of type. In our case, PICC line tip culture showed a significant growth of P. luteola (>15 CFU/plate by roll plate method [19]), which was similarly presented by Otto et al and Dharmayanti et al [2,11]. In the present case and previous cases, the removal of the CVL along with the appropriate antibiotics regimen lead to excellent outcomes.
An outstanding finding in the present case is the 0.8–1.0 mm vegetation in the heart valve that was discovered by echo. Similar findings were found in 2 other cases. The first case was presented by Chihab et al, in which echo revealed mitral valve deficiency without vegetation, but vegetation appeared on the prosthetic mitral valve after 6 days of admission [13]. The second case was presented by Casalta et al, in which echo revealed a 3-cm vegetation with grade 4 valvular regurgitation of the prosthetic aortic valve [18].
The present case showed a vegetation of the right side of the heart, while the other 2 cases, presented by Chihab et al and Casalta et al, had vegetations of the left side of the heart. This means that the side of the heart involved can differ according to the predisposing factor, as in the present case right heart in which involvement could be explained by the long-term use of a CVL, while the other 2 cases with left heart involvement were predisposed by the presence of a prosthetic mitral valve and a rheumatic heart disease in the case presented by Chihab et al, and prosthetic aortic valve alone as presented by Casalta et al [13,18]. Regarding the cases associated with CVL or infective endocarditis, it was found that cases with heart valve involvement required more aggressive treatment and longer duration compared to cases of CVL without heart valve involvement. Cases with heart valve involvement required a mean of 67.5days of treatment, while recovery in cases without documented valvular pathology only took a mean of 20.8 days. Also, even though infective endocarditis with valvular vegetation was present in 3 cases only, 1 case was fatal, making
Conclusions
References:
1.. Wen AY, Weiss IK, Kelly RB, Chryseomonas luteola bloodstream infection in a pediatric patient with pulmonary arterial hypertension receiving intravenous treprostinil therapy: Infection, 2013; 41(3); 719-22
2.. Otto MP, Foucher B, Dardare E, Gérôme P: Med Mal Infect, 2013; 43(4); 170-71
3.. Bayhan GI, Senel S, Tanir G, Ozkan S: Jpn J Infect Dis, 2015; 68(1); 50-4
4.. Connor BJ, Kopecky RT, Frymoyer PA, Forbes BA: J Clin Microbiol, 1987; 25(6); 1113-14
5.. Rahav G, Simhon A, Mattan Y, Infections with chryseomonas luteola [cdc group ve-1] and flavimonas oryzihabitans [cdc group ve-2]: Med [United States], 1995; 74(2); 83-88
6.. Gabaldon D, Wiggins B, Tzamaloukas AH: Int Urol Nephrol, 2013; 45(6); 1827-28
7.. Su SY, Chao CM, Lai CC: Perit Dial Int, 2014; 34(1); 137-38
8.. Roberts W, Roessler C, Francis PJ: Cureus, 2018; 10(10); e3441
9.. Jayagopal S, Berry MG, Ross G, Howcroft AJ, Hand infection caused by Chryseomonas luteola: Br J Plast Surg, 2004; 57(7); 693-94
10.. Ngoh E, Zohoun A, Ghazouani M: Med Mal Infect, 2011; 41(7); 399-400
11.. Dharmayanti A, Astrawinata D, Ventilator-associated pneumonia [VAP] in a patient with Guillain-Barre syndrome: Acta Med Indones, 2017; 49(2); 151-57
12.. Freney J, Hansen W, Etienne J: J Clin Microbiol, 1988; 26(6); 1241-43
13.. Chihab W, Alaoui AS, Amar M: J Clin Microbiol, 2004; 42(4); 1837-39
14.. Uy HS, Leuenberger EU, De Guzman BB, Natividad FF: Ocul Immunol Inflamm, 2007; 15(4); 359-61
15.. Naik AU, Prakash VJ, Susvar P: Indian J Ophthalmol, 2017; 66(8); 1200-2
16.. Ghosh SK: J Infect, 2000; 41(1); 109-10
17.. Ottonello G, Dessì A, Pinna AP, luteola infection in paediatrics: Description of a rare neonatal case and review of the literature: J Chemother, 2013; 25(6); 319-23
18.. Casalta JP, Fournier PE, Habib G: BMC Infect Dis, 2005; 5; 82
19.. Maki DG, Weise CE, Sarafin HW, A semiquantitative culture method for identifying intravenous-catheter-related infection: New England Journal of Medicine, 1977; 296(23); 1305-9
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,422
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133