06 April 2022: Articles 
Two Case Presentations of Scapulothoracic Dissociation with a Range of Features and Approaches to Management: A 26-Year-Old Woman Injured in a Car Accident and a 52-Year-Old Woman Injured While Cycling
Challenging differential diagnosis, Unusual setting of medical care, Rare disease, Educational Purpose (only if useful for a systematic review or synthesis), Rare coexistence of disease or pathology
Christos Vlachos1ABCEF*, Eftychios PapagrigorakisDOI: 10.12659/AJCR.935781
Am J Case Rep 2022; 23:e935781






Abstract
BACKGROUND: Scapulothoracic dissociation (SD) is caused by a high-energy trauma that results in disruption of the scapulothoracic articulation, scapula and clavicular fracture, and severe neurovascular injury. This report describes 2 cases of traumatic SD with a range of features and approaches to management, a 26-year-old woman injured in a car accident and a 52-year-old woman injured while cycling.
CASE REPORT: Case 1. A 26-year-old woman sustained an SD due to a car accident. A high index of suspicion led to the diagnosis, since there was a subtle clinical presentation. Open reduction and internal fixation (ORIF) of the clavicle was performed and the postoperative course was uncomplicated. Case 2. A 52-year-old woman was hit by a car while cycling and sustained multiple trauma injuries including a simultaneous brachial plexus injury and central cord syndrome, making the diagnosis of both entities a challenge. ORIF of the clavicle was performed and the brachial plexus was treated in a second stage. At the time of this report, the prognosis was poor.
CONCLUSIONS: These cases have shown that the accurate diagnosis of SD requires a high index of suspicion and a detailed clinical examination and imaging, since there is a range of presentations and anatomic findings. Rapid treatment is crucial in preventing limb deformity and neurological damage and saving the patient’s life.
Keywords: Central cord syndrome, Scapula, Shoulder, Accidents, Adult, Automobiles, Clavicle, Female, Humans, Multiple Trauma
Background
The scapulothoracic articulation (SD) is characterized as an atypical joint, since there is no cartilage, synovium, or capsule [1]. Instead, the interval between the scapula and thorax consists of muscles and bursae, with the scapula conjoined only indirectly with the axial skeleton through the acromioclavicular and sternoclavicular joints [2]. Knowledge of this unusual anatomy is crucial in understanding the mechanism of SD, a devastating and potential limb- and life-threatening injury of the shoulder girdle with a mortality rate of approximately 10% [3]. Oreck et al [4] described SD as a laterally displaced scapula with separation of the ipsilateral acromioclavicular joint and rupture of the ipsilateral brachial plexus and subclavian vessels, without lesion of the overlying skin. Since a high-velocity mechanism is needed to provoke an SD [1,5], clinicians’ attention tends to be distracted from the presence of associated injuries; thus, SD can be overlooked. Today, SD is no longer an infrequent entity. This is attributed to the expansion of its definition [1,6] and to its early diagnosis [1].
Several authors have published cases of SD, which despite their similarities, were not as challenging as those in our present report. For instance, Stepanovic et al [7] and Anbarasan et al [8] reported cases of open SD and their treatment plans, while Vergano et al [9] presented a case of incomplete tetraplegia and SD. In addition, Masmejean et al [3] reported cases of SD with associated upper limb fractures.
Evaluation of the patient begins with the Advanced Trauma and Life Support (ATLS) protocol [1] and continues with clinical examination and imaging studies [10]. A definitive treatment of SD is still lacking, as there is not yet a widely accepted algorithm for the order and surgical options of the individual injuries. This paper analyzes 2 challenging cases of traumatic SD with a range of injuries and approaches to management in an attempt to shed light on the wide clinical spectrum of this rare lesion. The first case regards a 26-year-old woman who was injured in a car accident and had a subtle clinical presentation and a favorable outcome, while the second case describes a 52-year-old woman injured while cycling and sustained an open clavicle fracture, leading to a simultaneous brachial plexus palsy and central cord syndrome.
Case Reports
CASE 1:
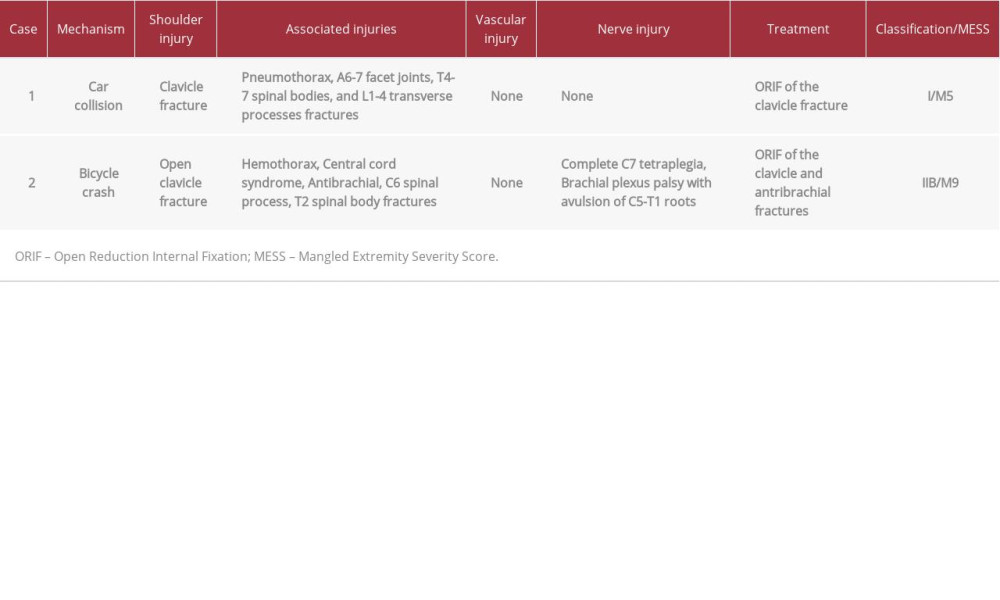
A 26-year-old woman with a non-contributory past medical history presented as an emergency following a head-on road traffic accident while driving her car. On arrival, she was anxious and presented with hypotension, tachycardia, and tachypnea (hypovolemic shock grade 3). Breath sounds were absent in the left lung, while she had a Glasgow Coma Scale score of 13 and a reported history of unconsciousness. Following the ATLS protocol, she was resuscitated with crystalloids and blood products. The chest radiograph revealed a left pneumothorax, which was treated with a chest tube insertion. On inspection, there was profound swelling on the anterosuperior aspect of the left shoulder and at the posterior aspect of the scapula, with intact overlying skin. A careful review of a well-centered chest radiograph revealed a displaced clavicle fracture (3.5 cm), with lateral translation of the scapula (Figure 1). The scapula index, which was first suggested by Kelbel et al, was 1.45 [11]. The acromioclavicular and sternoclavicular joints were intact. There were no neurologic deficits, while the brachial and radial pulses were palpable and there was a good capillary refill time in the left hand. In addition, she had fractures of the A6-7 facet joints, T4-7 spinal bodies, and L1-4 transverse processes. A computed tomography (CT) angiography was performed, with no significant findings. The Mangled Extremity Severity Score (MESS) was 5. By the time she was hemodynamically stable, the patient was taken to the operating room. Open reduction and internal fixation (ORIF), using an anatomic clavicle plate and locking screws, was performed (Figures 2, 3). After surgery, the clavicle fracture was reduced and the scapula was relocated to its normal position. The spinal fractures were treated conservatively with a Taylor’s spine brace and Philadelphia neck collar. Recovery was uncomplicated. The patient was mobilized the day after surgery and she was discharged 21 days after her hospital admission. At the 5-month follow up, the patient was doing very well. The range of motion of her shoulder was full and painless and she had returned to her occupation as a waitress (Figure 4, Table 1).
CASE 2:
A 52-year-old woman, with a non-contributory past medical history, was admitted as an emergency after being hit by a car and sustaining a lateral impact that threw her off her bicycle. By the time she presented, she was hemodynamically unstable, with severe tachycardia and hypotension, and was in respiratory distress (hypovolemic shock grade 4). She had a Glasgow Coma Scale score of 11, while the ambulance rescue team reported several episodes of unconsciousness. According to the ATLS protocol, a chest tube was inserted for hemothorax of the left lung, while crystalloid fluids and 2 blood units were administered to the patient. In neurological examination, it was noted that the patient had sustained an incomplete tetraplegia and complete brachial plexus palsy of the left upper extremity, while initial inspection revealed an open fracture of the left clavicle midshaft (Gustilo IIIa) [12] and an ipsilateral fracture of the antebrachial midshaft. The upper limb was pale and no brachial or radial pulses were palpable, although the perfusion was normal. Additional imaging studies showed a C6 spinal process, a T2 spinal body, and multiple left thoracic rib fractures, leading to a MESS score of 9, while CT angiography did not reveal any vessel injury. The wound on the clavicle was washed out carefully in the operating room and was primarily closed by the plastic surgeons. Magnetic resonance imaging (MRI) performed in a second stage revealed primarily a spinal cord edema at the cervical spine, which was clinically diagnosed as central cord syndrome, leading to the incomplete tetraplegia, extrusion of the C5-T1 brachial plexus roots (preganglionic damage), and rupture of the brachial plexus trunks at the site of the clavicle fracture (postganglionic damage), findings compactible with brachial plexus palsy. Furthermore, in radiological work-up the clavicle fracture was noted to be displaced enough (4 cm) and there was a measured scapula index of 1.55, implying the presence of an SD [11] (Figures 5, 6). After 4 days in the Intensive Care Unit, the patient was taken to the operating room, where an exploration of the brachial plexus and ORIF of the clavicle and the forearm were performed using plates and screws (Figure 7). It was decided that the brachial plexus would be treated with neuron grafts at a second stage due to extensive damage. The postoperative X-ray showed a reduced scapula with no signs of shoulder girdle instability. At the 3-month follow-up, the patient seemed to have no improvement of her neurologic condition (Table 1).
Discussion
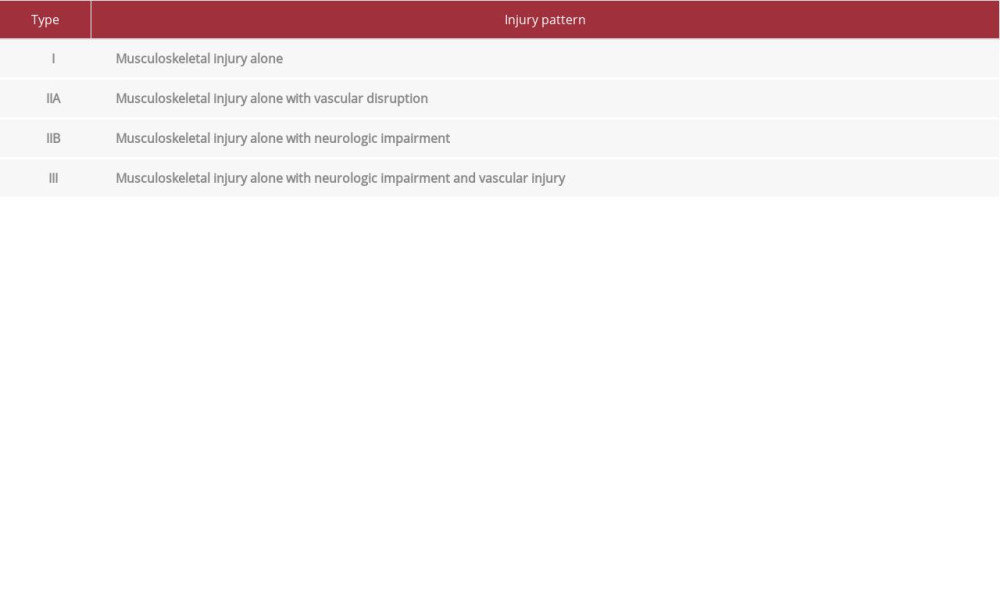
The main lesson to be learned from the abovementioned case reports is that an SD can present with a variety of clinical manifestations, since the symptoms of the first patient were insignificant, while the symptoms of the second patient were marked and overlapping. Subsequently, a high index of suspicion was predisposed from the clinician in order to diagnose both patients. In this direction, Zelle et al [13] modified the first practical classification described by Damschen et al [5] in an attempt to encompass the majority of SD’s clinical presentations (Table 2). Thus, Zelle et al created an effective tool not only in determining the need for additional testing, but also the appropriate timing for surgical intervention [13]. Our first case was categorized as I and the second case as IIIB, according to this classification.
The first patient had a quiet clinical manifestation of SD. Despite the clavicle fracture, the overlying skin was intact, the whole upper limb was rosy with palpable pulses, while the neurological examination revealed nothing. The only clinical finding was an intense edema of the shoulder area, a presentation that may not raise a suspicion of SD. On the contrary, the second patient had a noisy clinical presentation, since she had sustained an open clavicle fracture (Gustilo IIIa) [12], with concomitant fracture of the ipsilateral antebrachial midshaft. Furthermore, her upper limb was pale and no pulses could initially be palpated. A significant difficulty came up during neurological examination since an incomplete tetraplegia and complete brachial plexus palsy were revealed. More specifically, this complicated clinical manifestation was attributed to the overlapped presence of a central cord syndrome and brachial plexus injury at the fracture site. To the best of our knowledge, there is only 1 case report, published by Vergano et al [9], in which the patient had an incomplete tetraplegia and complete disruption of the brachial plexus and the axillary artery, and was finally treated with an above elbow amputation.
In the literature, 3 major injury types of SD have been described, with the most common being a distracted clavicle fracture, as in both of our cases, followed by dissociation of the acromioclavicular and sternoclavicular joints [3,7,14,]. Moreover, a simultaneous extremity fracture is not rare, with a coincidence of humerus, radius, ulna, and hand fractures of 41% in patients with SD [8,15]. Similar published studies have reported cases of concomitant humeral and forearm fractures [3,9,16] that were surgically treated in the same stage with the SD, and once the critical phase was under control.
Brachial plexus injuries are documented in almost 100% of patient with SD [5], in contrast to our first patient in whom neurological symptoms were absent. It is crucial to distinguish whether the damage is preganglionic or postganglionic and if the paralysis is complete or partial, since these factors affect the functional prognosis of the patient. A 2-level neurological lesion with proximal damage in the region where the root emerges from the foramen and a second injury more distally is also a possibility [4], as happened in our second patient. This double and nonrepairable injury led to the decision of reconstructing the brachial plexus in a second stage, despite the risk of scar formation [1].
Regarding the rare occasion of open SD, the literature is not wide because of the limb- and life-threatening nature of this injury [7]. Stepanovic et al [7] performed a percutaneous placement of an intramedullary Schanz pin in their patient for damage control reasons, while Anbarasan et al [8] had no other choice but to proceed to forequarter amputation. In our case, a meticulous surgical cleaning of the wound was primarily performed and an ORIF of the clavicle was achieved in a second stage. A remarkable comment is that these severe and concomitant injuries, as in our second case, tend to divert physicians’ attention and may lead to a delayed diagnosis.
Essential to the diagnostic process are the imaging studies. Primarily, a well-centered and non-rotated chest radiograph can show an increased soft-tissue density in the shoulder area and a bony or ligamentous injury. Oreck et al [4] suggested measuring the distance between a midline thoracic spinous process and the medial border of the scapula in both sides, with a difference >1 cm to indicate an SD, a proven efficient tool in the literature [3,17]. Additionally, given that scapula position changes depending on patient position, Kelbel et al [11] introduced the idea of scapula index by calculating the ratio of the distances on the injured and uninjured side, with a mean scapula index of 1.29 being indicative of SD. CT and MRI myelography are also useful, since they can detect a nerve root avulsion, a preganglionic or postganglionic injury, or a spinal cord edema [1,3,10,18]. Our first patient had no neurological symptoms to justify a myelography, while in the second patient, a cervical spine and brachial plexus MRI were performed. In addition, electromyography and nerve conduction velocity studies are efficient in identifying the location of the damage and monitoring the status of the nerve injury. However, they should be performed no sooner than 3 to 4 weeks after injury [19,20].
Concerning the treatment of bony injuries, there are no widely accepted treatment guidelines in the literature. Many authors prefer to proceed firstly to ORIF of the clavicle fracture, this way, protecting the underlying vascular and neurological repair [3,9,16]. The same was performed in both of our cases. As for brachial plexus injuries, treatment options depend on the location and the severity of the lesion, and the goals are chiefly the restoration of elbow flexion and subsequently the dynamic stabilization of the shoulder girdle, the restoration of arm adduction and of C6–C7 regional sensation, and finally of wrist extension and finger flexion [18,21].
In conclusion, the 2 cases presented here differ significantly in their clinical presentation, severity, and prognosis. The first patient had a subsequent injury and, after the operative treatment, she had a relatively short hospitalization and an almost full recovery in the following months, achieving an excellent outcome. In contrast, representing the majority of published cases [3,8,9], the second patient sustained a serious brachial plexus injury and central cord syndrome that demanded a prolonged rehabilitation course, with an overall poor prognosis.
Conclusions
The early recognition and diagnosis of SD presuppose a high suspicion, meticulous clinical examination, and careful radio-graphic evaluation. The surgeon should coordinate all of these and facilitate any urgent or late intervention in order to prevent a life-threatening condition, limb deformity, or neurological damage. Despite its increasing frequency of occurrence, the complexity and wide clinical spectrum of SD makes the establishment of evidence-based treatment guidelines very difficult. Finally, the prognosis in the majority of patients is not good, and therefore, additional literature in this direction should be developed.
Figures
References:
1.. Choo AM, Schottel PC, Burgess AR, Scapulothoracic dissociation: Evaluation and management: J Am Acad Orthop Surg, 2017; 25(5); 339-47
2.. Warth RJ, Spiegl UJ, Millett PJ, Scapulothoracic bursitis and snapping scapula syndrome: A critical review of current evidence: Am J Sports Med, 2015; 43(1); 236-45
3.. Masmejeam EH, Asfazadourian H, Alnot JY, Brachial plexus injuries in scapulothoracic dissociation: J Hand Surg Br, 2000; 25(4); 336-40
4.. Oreck SL, Burgess A, Levine AM, Traumatic lateral displacement of the scapula: A radiographic sign of neurovascular disruption: J Bone Joint Surg Am, 1984; 66(5); 758-63
5.. Damschen DD, Cogbill TH, Siegel MJ, Scapulothoracic dissociation caused by blunt trauma: J Trauma, 1997; 42(3); 537-40
6.. Flanagin BA, Leslie MP, Scapulothoracic dissociation: Orthop Clin North Am, 2013; 44(1); 1-7
7.. Stepanovic ZL, Milisavljevic SS, Prodanovic NS, Open scapulothoracic dissociation: J Trauma Acute Care Surg, 2015; 79(4); 698-700
8.. Anbarasan A, Mohamad NH, Mariapan S, Open traumatic scapulothoracic dissociation: Case report of a rare injury: Trauma Case Rep, 2018; 18; 42-45
9.. Vergano LB, Monesi M, Scapulothoracic dissociation: A devastating “floating shoulder” injury: Acta Biomed, 2018; 90(1-S); 150-53
10.. Brucker PU, Gruen GS, Kaufmann RA, Scapulothoracic dissociation: Evaluation and management: Injury, 2005; 36(10); 1147-55
11.. Kelbel MJ, Jardon OM, Hurman WW, Scapulothoracic dissociation: A case report: Clin Orthop, 1986; 209; 210-14
12.. Kim PH, Leopold SS, In brief: Gustilo-Anderson classification. [corrected]: Clin Orthop Relat Res, 2012; 470(11); 3270-74
13.. Zelle BA, Pape HC, Gerich TG, Functional outcome following scapulothoracic dissociation: J Bone Joint Surg Am, 2004; 86(1); 2-8
14.. Merk BR, Minihane KP, Shah NA, Scapulothoracic dissociation with acromioclavicular separation: A case report of a novel fixation method: J Orthop Trauma, 2008; 22(8); 572-75
15.. Lee L, Miller TT, Schultz E, Toledano B, Scapulothoracic dissociation: Am J Orthop (Belle Mead NJ), 1998; 27(10); 699-702
16.. Albert S, Jayashankar V, Gouse M, A paradoxical triad: scapulothoracic dissociation with clavicle and humeral shaft fractures: Case Rep Emerg Med, 2014; 2014; 689157
17.. Nagi ON, Dhillon MS, Traumatic scapulothoracic dissociation. A case report: Arch Orthop Trauma Surg, 1992; 111(6); 348-49
18.. Doi K, Otsuka K, Okamoto Y, Cervical nerve root avulsion in brachial plexus injuries: Magnetic resonance imaging classification and comparison with myelography and computerized tomography: J Neurosurg, 2002; 96(3 Suppl.); 277-84
19.. O’Shea K, Feinberg JH, Wolfe SW, Imaging and electrodiagnostic work-up of acute adult brachial plexus injuries: J Hand Surg Eur Vol, 2011; 36(9); 747-59
20.. Ainscow DA, Dislocation of the scapula: J R Coll Surg Edinb, 1982; 27(1); 56-57
21.. Rorabeck CH, Harris WR, Factors affecting the prognosis of brachial plexus injuries: J Bone Joint Surg Br, 1981; 6-B(3); 404-7
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133