12 April 2022: Articles 
A Case of Rebound Inflammation in a 38-Year-Old Man with Severe COVID-19 Pneumonia Following Cessation of Dexamethasone Therapy
Unusual clinical course, Challenging differential diagnosis, Unusual or unexpected effect of treatment, Clinical situation which can not be reproduced for ethical reasons
Hoa TranDOI: 10.12659/AJCR.935946
Am J Case Rep 2022; 23:e935946






Abstract
BACKGROUND: Since the initial COVID-19 cases in 2019, the pandemic has expanded globally. Clinical data showed that dexamethasone treatment at a dose of 6 mg daily for up to 10 days in hospitalized patients with COVID-19 who were receiving respiratory support decreased 28-day mortality in COVID-19 patients. Recent reports, on the other hand, have indicated that both steroid resistance and rebound events occur. We report a case of rebound inflammation after the termination of dexamethasone medication in a 38-year-old man with severe COVID-19 pneumonia, which improved after the reintroduction of dexamethasone.
CASE REPORT: A 38-year-old male patient with no past medical history of note presented with new onset of dyspnea. He was subsequently diagnosed with severe coronavirus disease 2019 (COVID-19). Initially, the patient was clinically improved following a 3-day course of 16 mg of dexamethasone daily. Shortly after discontinuing corticosteroids, the patient’s clinical condition deteriorated, necessitating increased oxygen support. Following the reintroduction of corticosteroids, the patient gradually improved and responded favorably in terms of respiratory function, symptoms, and imaging, after which he was successfully discharged.
CONCLUSIONS: This case exemplifies the previously observed rebound effects of discontinuing dexamethasone medication in individuals with severe COVID-19 pneumonia. The timing and length of dexamethasone medication should be tailored to the individual patient. In addition, monitoring lung function should be part of the gradual withdrawal of dexamethasone to avoid rebound lung inflammation and the long-term effects of increasing lung fibrosis.
Keywords: COVID-19, Cytokines, Glucocorticoids, Adrenal Cortex Hormones, Adult, Dexamethasone, Humans, Inflammation, Male, SARS-CoV-2, COVID-19 Drug Treatment
Background
The first case of COVID-19 was identified in Wuhan city, China in 2019 and this infection has since spread rapidly around the world. According to WHO’s World Health statistics in January 2021, over 80 million confirmed cases have been registered in the world [1]. Among patients infected with COVID-19, asymptomatic and mild symptoms were reported in 81%, severe symptoms (ie, dyspnea and hypoxemia) were reported in 14%, critical symptoms (ie, respiratory failure, shock, and multi-organ damage) were reported in 5%, and the overall mortality rate was 2.3% [2]. It is assumed that host immune response plays an important role in the immunopathological mechanism of cytokine storm syndrome in critically ill patients with COVID-19. Accordingly, immunomodulatory agents that suppress an excessive inflammatory response (eg, corticosteroids) are promising potential therapies for COVID-19. Among available therapies, corticosteroids are widely used in clinical practice and multiple clinical trials showed they lower the mortality rate [3]. In patients hospitalized with COVID-19, the use of dexamethasone 6 mg daily resulted in lower 28-day mortality rate among those who were receiving respiratory support [4]. However, cases of corticosteroid resistance or rebound inflammatory response during corticosteroid tapering or after discontinuation have been reported [3,5–7]. This report describes a case of rebound inflammation in a 38-year-old man with severe COVID-19 pneumonia following cessation of dexamethasone therapy, with improvement following reintroduction of dexamethasone.
Case Report
A 38-year-old male patient with no prior medical history was admitted to the hospital with shortness of breath. The patient had a mild temperature, a dry cough, and no difficulties breathing 15 days before admission. Rapid COVID-19 antigen testing revealed a positive result. The patient was subsequently instructed to remain at home and self-isolate. Two days later, the patient experienced mild exertional dyspnea and required 10 days of home nasal cannula oxygen therapy. As the dyspnea became more severe, he was transferred to a tertiary hospital and treated there for 2 days with methylprednisolone (32 mg once daily), high-flow nasal cannula (HFNC) oxygenation, and empiric antibiotic (levofloxacin) without improvement. He was then transferred to University Medical Center Ho Chi Minh City. Clinical status on admission of the patient was assessed as follows: conscious, coherent, breathing with difficulty, SpO2 of 96% on HFNC (Flow=60 L/min, FiO2=55%). A chest X-ray showed bilateral pulmonary patchy infiltrates (Figure 1). The real-time polymerase chain reaction method used to diagnose SARS-CoV-2 infection was Alinity m SARS-CoV-2, which gave a positive result.
The patient was then treated with methyl-prednisolone (125 mg twice daily for 3 days), enoxaparin (6000 UI twice daily) and empiric antibiotic (levofloxacin). Three days later, dyspnea and oxygen demand was reduced, the patient was given oxygen via nasal cannula with 3-4 L/min flow, antibiotic (levofloxacin), enoxaparin, and methylprednisolone (80 mg twice daily for 3 days, tapered to 32 mg twice daily from days 7 to 9).
Between days 10 and 13, the patient had more acute dyspnea and required a higher degree of oxygen assistance, with more bilateral pulmonary infiltrates on chest X-rays (Figure 2A). He was suspected of having secondary pneumonia at the time and was treated with broad-spectrum empiric antibiotics (levofloxacin, meropenem, and vancomycin). His shortness of breath, however, became worse, he developed a low-grade fever, and his chest computed tomography (CT) scan revealed diffuse interstitial lesions in both lungs (Figure 2B). His persistent fever, shortness of breath, and increased CRP and IL-6 indicated unresponsiveness to broad-spectrum antibiotics (Table 1). By then, a high clinical suspicion existed for an inflammatory rebound. We decided to be re-administer dexamethasone phosphate 16 mg daily and continued empiric antibiotics. He no longer had fever after 2 days corticosteroids re-administration, his dyspnea improved, and the oxygen requirement gradually decreased after 4 days (Figure 3). The duration of the second course of corticosteroid was 9 days and he was discharged from the hospital. Microbiological testing during hospitalization was all negative (day 1: negative blood and sputum culture, day 12: negative blood and sputum culture; negative fungal blood culture and acid-fast bacillus).
Discussion
We reported that a 38-year-old man with severe COVID-19 pneumonia experienced rebound pneumonia after being treated with a standard course of corticosteroid. When rebound pneumonia occur, higher corticosteroid dose and longer duration of treatment beyond the recommended 10-day course are suggested to achieve remission and prevent relapse.
COVID-19 damages type II pneumocytes, which are important for lung tissue healing and surfactant synthesis. This results in an increase in surface tension, which causes difficulties breathing. Additionally, these wounded type II pneumocytes contribute to the loss of alveolar immunologic balance, triggering a cascade of overt local and systemic inflammatory responses. Cytokine agents excreted at an excessive level by activated inflammatory cells induce broad systemic harm as a result of the systemic inflammatory response syndrome. Additionally, this excessive response activates procoagulant factors, resulting in microthrombi in numerous tissues or other severe clinical conditions such as acute respiratory distress syndrome, multi-organ failure syndrome, and ischemia [8]. As a result, corticosteroids (especially dexamethasone and its substitutes) have been suggested in current guidelines for the treatment of COVID-19 in hospitalized patients requiring oxygen.
Nonetheless, several critical questions remain [9]: How to optimize the use of corticosteroids in the treatment of COVID-19? Should we tailor corticosteroid therapy to the individual patient, including the appropriate first dose, timing, and duration, based on clinical response or biomarkers? How can we determine whether the rebound phenomenon occurs following dose reduction or withdrawal of corticosteroids?
The following definition was given for the rebound phenomenon: (1) patients who responded to initial corticosteroid therapy; (2) patients who demonstrated a clinical deterioration of at least 1 point on the 7-point ordinal scale, worsened oxygenation, or required additional COVID-19 treatment within 1 week of corticosteroid reduction or cessation; and (3) patients in whom infection was ruled out retrospectively. When the dose of corticosteroids was reduced in this patient who originally responded to methyl-prednisone (125 mg twice daily) after 3 days of therapy, his clinical and laboratory symptoms deteriorated and improved upon re-initiation of corticosteroids. Similarly, Imai et al [6] described an inflammatory rebound reaction following corticosteroid reduction or discontinuation. Ryosuke Imai’s study described 113 COVID-19 patients treated with corticosteroids, with 9 patients (8.0%) relapsing into an inflammatory state. Three criteria were used to define the rebound group: (1) patients responded to initial corticosteroid therapy; (2) patients experienced a significant worsening of their clinical course (particularly worsening hypoxemia) following corticosteroid tapering or discontinuation; and (3) an infectious state must be ruled out. Imai et al’s study established that the rebound group began corticosteroids earlier in the illness phase and for a shorter duration. The median number of days between the onset of symptoms and the onset of an inflammatory rebound reaction was 12 days. Twenty days after symptom start, no rebound cases were observed. Corticosteroid therapy with a short duration was considered to be the cause of inflammatory rebound. Imai et al proposed extending the duration of corticosteroids to 14 days. As a result, the most likely therapeutic option for rebound is to increase the corticosteroid dose or to extend the period of treatment.
Our patient had 15 days from the onset of symptoms to admission. After 3 days of corticosteroid treatment, his clinical status improved, and then deteriorated on days 10–13 after hospitalization, roughly 25–28 days after symptom onset, which differed from Imai et al’s previously described restricted time frame of 14 days after symptom onset [6]. As a result, another possibility for our patient’s differential diagnosis is COVID-19 post-infection or interstitial lung disease. Similarly, Myall et al [10] reported that 39% of COVID-19 patients had persistent signs and symptoms 4 weeks following discharge. Interstitial lung illness, most often organizing pneumonia [3], was detected in 35 survivors (4.8%). On imaging, the majority of X-ray or computed tomography images revealed bilateral subpleural ground-class consolidation in the lower or middle section of the lung, or occasionally subpleural and peri-bronchial linear dense consolidation, as well as traction bronchiectasis. In terms of treatment, 30 of 35 patients received corticosteroids again and showed further improvement in respiratory function, symptoms, and imaging. Chen et al reported a 78-year-old patient with severe COVID-19 pneumonia. Initially, the patient was treated with dexamethasone 6 mg for 10 days. There was clinical improvement following the treatments. However, after the steroid was discontinued, on day 15, the patient experienced rebound pneumonia and clinical deterioration. His clinical condition improved until dexamethasone was re-administered [7]. In our patient, rebound occurred after tapering the corticoid. It could happen during corticosteroid tapering or after discontinuation. The dose and duration of the corticoid treatment should be individualized for each patient.
Chong et al [3] discussed the clinical, biochemical, and imaging similarities between the 2 entities of COVID-19 pneumonia and secondary organizing pneumonia (OP). Both present clinically as mild-to-subacute respiratory symptoms that are typically discovered years later as a result of atypical acute respiratory distress syndrome (ARDS) and silent hypoxemia. Histopathological findings such as ante-mortem biopsies or post-mortem autopsy can be used to differentiate these. Both of these entities are thought to be the result of a prolonged dysregulated immunological response following initial viral infection, which accounts for the good response to a second course of corticosteroid medication. Increased corticosteroid doses and treatment duration beyond the usual 10-day course are both recommended to establish remission and avoid relapse. Consistent evidence supports examining secondary OP in persons with past COVID-19 infection who have clinical and radiographic deterioration following recent cessation of corticosteroids, in the absence of evidence of new infection or other causation [3,11]. Secondary OP was a strong possibility in our patient. Despite the availability of chest CT, no lung biopsy was performed to confirm or establish secondary OP.
Conclusions
This case emphasizes the recently observed rebound consequences of discontinuing dexamethasone medication in individuals with severe COVID-19 pneumonia. The time and duration of dexamethasone medication should be tailored to each patient. Dexamethasone discontinuation should also include monitoring lung function to avoid rebound lung inflammation and the long-term effects of increasing lung fibrosis.
Figures
References:
1.. Gabutti G, d’Anchera E, De Motoli F, The epidemiological characteristics of the COVID-19 pandemic in Europe: Focus on Italy: Int J Environ Res Public Health, 2021; 18(6); 2942
2.. McIntosh K, COVID-19: Clinical features UpToDate. (last updated: 10, 2022). Available from: https://www.uptodate.com/contents/covid-19-clinical-features
3.. Chong WH, Saha BK, Chopra A, Does COVID-19 pneumonia signify secondary organizing pneumonia? A narrative review comparing the similarities between these two distinct entities: Heart Lung, 2021; 50; 667-74
4.. Horby P, Lim WS, Emberson JR, Dexamethasone in hospitalized patients with COVID-19: N Engl J Med, 2021; 384(8); 693-704
5.. Farrokhnia M, Dalfardi B, Letter to Editor: Inflammatory rebound in severe acute respiratory syndrome coronavirus 2 infection: Shiraz E-Medical Journal, 2021 [in press]
6.. Imai R, Ro S, Tomishima Y, Nishimura N, Steroid resistance and rebound phenomena in patients with COVID-19: Respir Invetsig, 2021; 59; 608-13
7.. Chen PH, Cheng CY, Li LF, Yu CC, Pneumonia rebound after stopping steroid in a patient with COVID-19: A case report: Respirol Case Rep, 2021; 9(11); e0869
8.. Shanmugam C, Mohammed AR, COVID-2019 – A comprehensive pathology insight: Pathol Res Pract, 2020; 216(2020); 153222
9.. Prescott HC, Rice T, Corticosteroids in COVID-19 ARDS evidence and hope during the pandemic: JAMA, 2020; 324(13); 1292-95
10.. Myall KJ, Mukherjee B, Persistent post-COVID-19 interstitial lung disease an observational study of corticosteroid treatment: Am Thorac Soc, 2021; 18(5); 799-806
11.. de Oliveira Filho CM, Vieceli T, de Fraga Bassotto C, Organizing pneumonia: A late phase complication of COVID-19 responding dramatically to corticosteroids: Braz J Infect Dis, 2021; 25(1); 101541
Figures
Tables
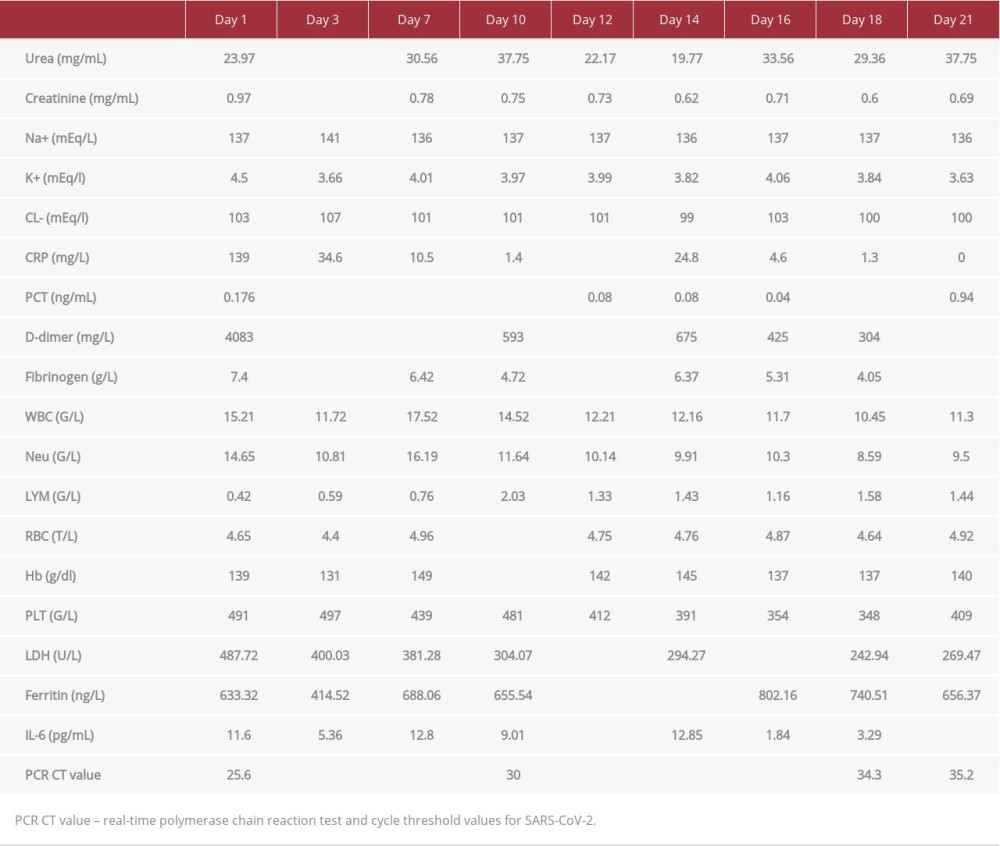 Table 1.. Laboratory findings during hospitalization, which first demonstrated lower inflammatory marker concentrations (days 1–3), but subsequently increased at day 7, and eventually declined following corticosteroid re-initiation.Table 1.. Laboratory findings during hospitalization, which first demonstrated lower inflammatory marker concentrations (days 1–3), but subsequently increased at day 7, and eventually declined following corticosteroid re-initiation.
Table 1.. Laboratory findings during hospitalization, which first demonstrated lower inflammatory marker concentrations (days 1–3), but subsequently increased at day 7, and eventually declined following corticosteroid re-initiation.Table 1.. Laboratory findings during hospitalization, which first demonstrated lower inflammatory marker concentrations (days 1–3), but subsequently increased at day 7, and eventually declined following corticosteroid re-initiation. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133