22 May 2022: Articles 
Hypokalemic Paresis in a 26-Year-Old Man After Recreational Cannabis Use
Unusual clinical course, Mistake in diagnosis
Simon Kjær Simonsen12ACDEF*, Nikolaj Fibiger RittigDOI: 10.12659/AJCR.936008
Am J Case Rep 2022; 23:e936008






Abstract
BACKGROUND: Hypokalemia (serum potassium level below 3.5 mmol/L) is present in approximately 11% of patients admitted to emergency departments. Hypokalemia can be a manifestation of many underlying causes and if untreated can be fatal. A careful approach to work-up and management is required in hypokalemic patients.
CASE REPORT: Here we report a 26-year-old previously healthy male patient who was admitted to the Emergency Department with rapidly progressing paresis of the lower and upper extremities. Initial laboratory results revealed severe hypokalemia of 2.1 mmol/l, which aggravated to 1.6 mmol/l before receiving treatment with intravenous potassium chloride supplementation. In addition, the patient developed rhabdomyolysis secondary to prolonged paralysis and immobilization induced by hypokalemia. Following this treatment, the patient’s symptoms eased rapidly, and his potassium concentration was normalized. The patient admitted to smoking cannabis the day before admission. In this case report, we systematically elaborate and exclude the causes of hypokalemia in this otherwise healthy young adult, including medication, gastrointestinal symptoms, licorice consumption, and genetical testing. Cannabis has been associated with hypokalemia, proposedly through activation of the cannabinoid receptor 1 (CB1)-mediated activation of G protein-coupled inwardly rectifying potassium (GIRK) channels.
CONCLUSIONS: This case report emphasizes that hypokalemia can cause paralysis and cannabis should be included in the diagnostic mindset.
Keywords: Cannabis, G Protein-Coupled Inwardly-Rectifying Potassium Channels, Hypokalemia, Receptors, Cannabinoid, Adult, Analgesics, Humans, Male, Paralysis, Paresis, Potassium, young adult
Background
Hypokalemia is a well-known phenomenon in emergency departments, and approximately 11% of patients present with a serum potassium level below 3.5 mmol/L [1]. Symptoms vary from no symptoms to muscle weakness, paralysis, and cramps in addition to the presence of U-waves, ventricular extrasystoles, ST-segment depression, and flattening of the T-wave in the ECG, and eventual cardiac arrest [1]. In severe cases, when the potassium level is lower than 2 mmol/L, frank rhabdomyolysis can occur with markedly elevated serum creatinine kinase and myoglobinuria [2,3].
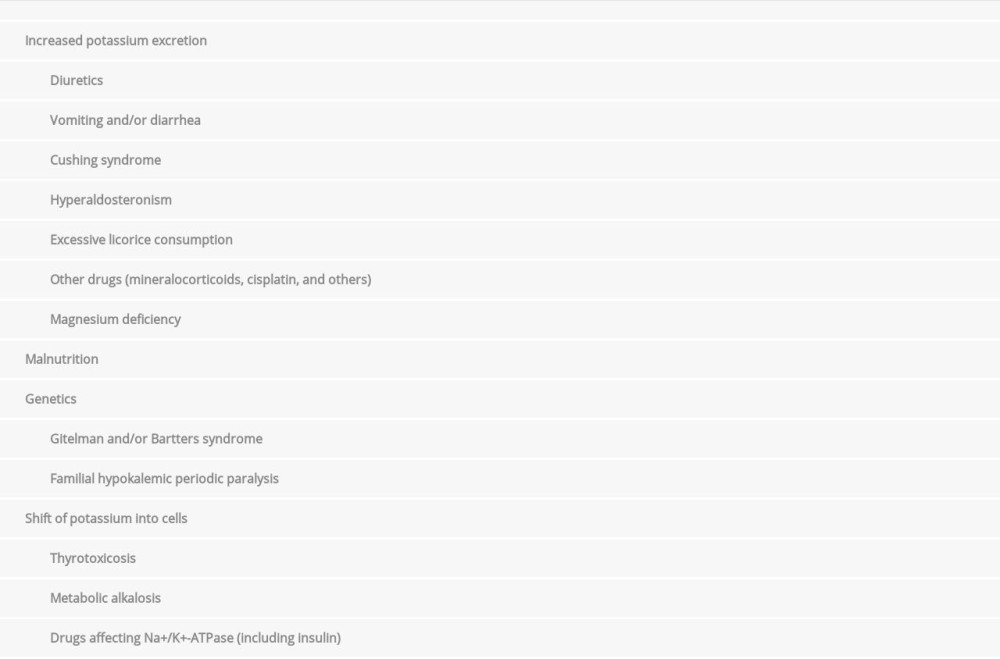
Hypokalemia can be divided into 4 principal causes: increased potassium excretion, displacement of extracellular potassium into the cells, genetic causes, and malnutrition (Table 1) [4] and/or the algorithm suggested by Gram et al [5]. Excretion is known to be the most common cause of severe hypokalemia (s-potassium <2.5 mmol/l) in Western countries, primarily due to treatment with diuretic medication and prolonged vomiting and/or diarrhea [1,4]. We present a case in which a young man presented with ascending paralysis, hardly distinguishable from Guillain-Barré syndrome, following a cannabis smoking episode the day before. The patient was diagnosed with severe hypokalemia. Case reports on the association between hypokalemia and cannabinoids are rare, and the mechanism of action is controversial.
Case Report
A 26-year-old man with no previous medical history, presented to the Emergency Department with a chief concern of rapidly progressing paralysis of the limbs. The night before admission, he felt progressing muscular tension and pain in the lower extremities. In the morning, as he woke up, the symptoms had aggravated to paralysis of the lower extremities and paresis of the upper extremities, hindering him from getting out of the bed. Therefore, the patient contacted his general practitioner, describing the symptoms and added that he did not perform any unusual activities on the days before, besides the fact that he was an occasional cannabis smoker, having smoked cannabis the night before.
However, he denied a daily use of cannabis and alcohol and had only used cannabis a few times before, without experiencing any of the above symptoms. Furthermore, he denied use of other psychoactive drugs, and he reported normal consumption of food and drinks on the days before admission. The general practitioner then admitted the patient to the Emergency Department, suspecting Guillain-Barré syndrome (GBS).
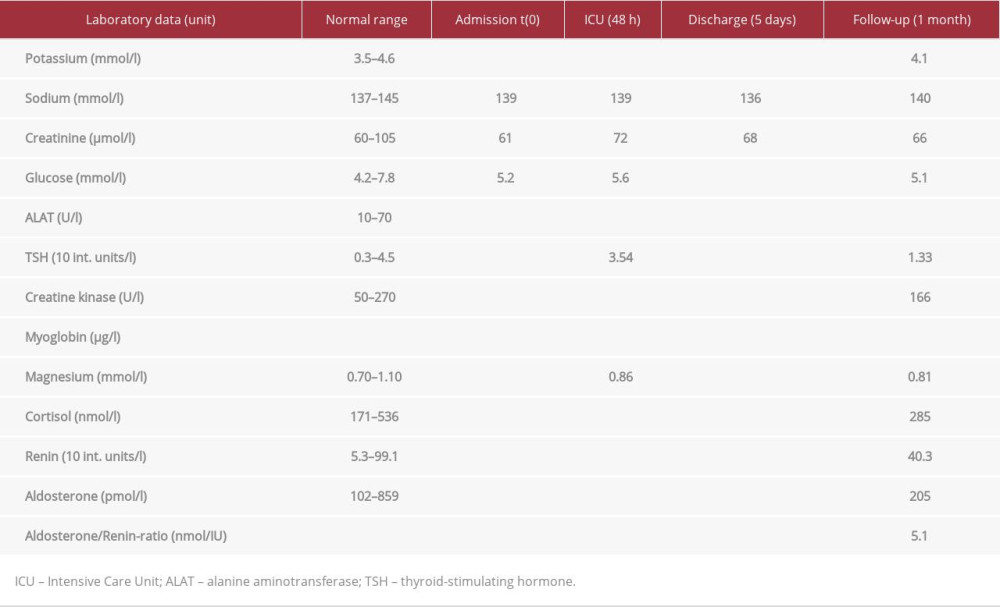
On examination in the Emergency Department, the patient was alert with a Glasgow Coma Score of 15. His vital parameters were normal, including a non-invasive blood pressure of 127/66 mmHg, heart rate of 66 bpm, pulse oximetry with 100% oxygen saturation, and a temperature of 36.8°C. The standard physical examination revealed no positive findings besides ceased motor function and tone in the lower extremities and to a lesser extent in the upper extremities. The reflex of the patella, hamstring, and Achilles’ tendon was diminished, while upper extremity reflexes, Babinski reflex, and all sensorics were intact. Results of examination of the cranial nerves were normal, and the lumbar puncture showed a normal cell count. Initial laboratory results revealed severe hypokalemia of 2.1 mmol/l and ALAT 133 U/l, while all other parameters tested were within the normal range (Table 2). Subsequent laboratory results revealed elevated serum creatine kinase and myoglobin, consistent with rhabdomyolysis.
Based on the anamnesis and examination, GBS was still heavily suspected and treatment with intravenous human immunoglobulin was initiated. Over the next 36 h, the patient’s symptoms (peripheral paralysis, abolished reflexes, and shortness of breath) gradually intensified despite treatment with immunoglobulins, and a repeat arterial blood gas analysis revealed aggravation of the existing hypokalemia (1.6 mmol/l). Immediately thereafter, the patient was transferred to the Intensive Care Unit, where 100 mmol potassium chloride was administered over the next few hours. Following this treatment, the patient’s weakness began to ease as the potassium concentration was normalized (Table 2). His rhabdomyolysis was treated with per oral rehydration and small amounts of intravenous fluids. He was discharged 2 days later after being advised to avoid recreational use of cannabis. During follow-up, the potassium supplement was gradually tapered without reoccurrence of hypokalemia.
Discussion
In our search for a plausible cause of severe hypokalemia in the 26-year-old otherwise healthy man, we provide a systematic discussion of the 4 main causes of hypokalemia in relation to the case report.
Increased potassium excretion seems unlikely in the case presented, as the patient did not take any daily medication, had no gastrointestinal problems (eg, vomiting or diarrhea), and did not consume licorice in the period leading up to admission. He had no clinical signs of Cushing syndrome, and follow-up laboratory results confirm normal serum cortisol and no sign of hyperaldosteronism. Malnutrition also seems unlikely as the patient was a 107-kg well-nourished man. Inherited disorders, such as Gitelman syndrome (GS) and Bartters syndrome (BS), are known to cause hypokalemia through the inactivation of genes coding for 2 different ion transporters in the kidney, leading to increased potassium excretion. GS is known to cause hypokalemia and hypomagnesemia that often goes unrecognized until young adulthood, while BS is frequently diagnosed in neonates due to growth retardation and nephrocalcinosis [6]. Our patient presented with continuously normal levels of serum magnesium on follow-up, and no other family members were known to have hypokalemia and/or hypomagnesemia, leaving the above genetic disorders unlikely to be present in our patient. Furthermore, genetic testing for familial hypokalemic periodic paralysis (FHPP) revealed normal variants of the CACNA1S and SCN4A genes. The patient presented with normal pH and thyroid-stimulating hormone (TSH) upon admission and on follow-up, indicating there was no metabolic alkalosis or thyrotoxicosis causing a shift of potassium into the cells (the cause of hypokalemia).
In the existing literature, there are other case series and small-scale studies showing hypokalemia associated with cannabis and synthetic cannabinoid use [7–10]. However, the mechanism of action is controversial. Hermanns-Clausen et al [7] proposed 3 mechanisms that may be involved: potassium loss via the kidneys, potassium loss by excessive sweating or diarrhea, and potassium shift into cells. Case reports suggest a fourth and different mechanism of action, as cannabis use is often followed by a craving for food, resulting in binge-eating [8,9]. Consumption of large amounts of carbohydrates stimulates insulin release, which drives potassium into the muscle cells, leading to extracellular hypokalemia. Our patient had no excessive sweating or diarrhea, and there was no indication of increased renal potassium loss in the anamnesis. Additionally, the patient did not report any binge-eating episode in relation to the cannabis smoking episode.
Cannabinoid receptors can affect the shift of potassium from the extracellular to the intracellular space. The proposed mechanism of action includes 2 major cannabinoid receptors – CB1 and CB2 [11]. The CB1 receptor is of particular interest, as stimulation is known to cause an activation of G protein-coupled inwardly rectifying potassium (GIRK) channels through intra-cellular signal cascades [12,13]. The CB1 receptor is widely expressed in the brain, but recent evidence suggests that CB1 receptors are also expressed in several peripheral tissues, including the lungs, heart, and vasculature [11] as well as skeletal muscle and adipocytes [13]. Further studies support that CB1 receptors play an important role in hypokalemia following cannabis use [7,10].
With regards to the rhabdomyolysis, this condition is known to cause hyperkalemia from the damaged muscle cells releasing potassium [14], although in that case presenting paradoxically together with hypokalemia. However, for that patient, the cause of rhabdomyolysis was most likely a result of prolonged immobilization [14] secondary to the peripheral paralysis from hypokalemia. The above effect of rhabdomyolysis on the serum potassium level emphasizes the severity of the patient’s hypokalemia from cannabis use.
Conclusions
Hypokalemia is frequently detected in patients admitted to emergency departments; it has numerous causes and symptoms vary. Cannabis is known to cause hypokalemia, proposedly through activation of cannabinoid receptor 1 (CB1)-mediated activation of G protein-coupled inwardly rectifying potassium (GIRK) channels. Here, we present a case of cannabis-induced severe hypokalemia causing paralysis of upper and lower extremities, as well as rhabdomyolysis. This case emphasizes that hypokalemia can cause peripheral paralysis and cannabis should be included in the diagnostic mindset.
References:
1.. Marti G, Schwarz C, Leichtle AB, Etiology and symptoms of severe hypokalemia in emergency department patients: Eur J Emerg Med, 2014; 21(1); 46-51
2.. Knochel JP, Neuromuscular manifestations of electrolyte disorders: Am J Med, 1982; 72(3); 521-35
3.. Knochel JP, Schlein EM, On the mechanism of rhabdomyolysis in potassium depletion: J Clin Invest, 1972; 51(7); 1750-58
4.. , [Doctor’s Handbook]Lægehåndbogen: [Hypokalaemia] Hypokaliæmi, Copenhagen, Denmark, Sundhed.dk Updated 04.02.2022. Available at: [in Danish]https://www.sundhed.dk/sundhedsfaglig/laegehaandbogen/generelt/tilstande-og-sygdomme/elektrolytforstyrrelser/hypokaliaemi/
5.. Grams ME, Hoenig MP, Hoorn EJ, Evaluation of hypokalemia: JAMA, 2021; 325(12); 1216-17
6.. Hansen KW, Mosekilde L, [Gitelman syndrome. An overlooked disease with chronic hypomagnesemia and hypokalemia in adults]: Ugeskr Laeger, 2003; 165(11); 1123-27 [in Danish]
7.. Hermanns-Clausen M, Kneisel S, Szabo B, Auwärter V, Acute toxicity due to the confirmed consumption of synthetic cannabinoids: Clinical and laboratory findings: Addiction, 2013; 108(3); 534-44
8.. Feldman ML, Hadfield S, Pot paresis: Marijuana and a case of hypokalemic periodic paralysis: J Emerg Med, 2009; 36(3); 236-38
9.. Tantravahi P, Sengchannavong A, Halloran A, Johnston E, Rare case of hypokalemic periodic paralysis associated with marijuana binge episode: Abstract published at Hospital Medicine 2018 April 8–11, Orlando, Fla Abstract 883. May 21st 2021https://shmabstracts.org/abstract/rare-case-of-hypokalemic-periodic-paralysis-associated-with-marijuana-binge-episode/
10.. Osadolor HB, Emokpae AM, Effects of marijuana on sodium and potassium (na + & p +) ions homeostasis among smokers in Benin City – a metropolitan city in Nigeria: Int J Pharma Bio Science, 2010; 1(3); 1-3
11.. Ye L, Cao Z, Wang W, Zhou N, New Insights in cannabinoid receptor structure and signaling: Curr Mol Pharmacol, 2019; 12(3); 239-48
12.. Ibsen MS, Connor M, Glass M, Cannabinoid CB(1) and CB(2) receptor signaling and bias: Cannabis Cannabinoid Res, 2017; 2(1); 48-60
13.. Mackie K, Cannabinoid receptors: Where they are and what they do: J Neuroendocrinol, 2008; 20(Suppl. 1); 10-14
14.. Cabral BMI, Edding SN, Portocarrero JP, Lerma EV, Rhabdomyolysis: Dis Mon, 2020; 66(8); 101015
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133