23 May 2022: Articles 
Liver Transplantation for Giant Hemangioma Complicated by Kasabach-Merritt Syndrome: A Case Report and Literature Review
Unusual or unexpected effect of treatment, Rare disease
Yi Zhao1ADEF*, Carley E. Legan1AEDOI: 10.12659/AJCR.936042
Am J Case Rep 2022; 23:e936042






Abstract
BACKGROUND: Liver hemangiomas are the most common benign liver tumor. Giant hepatic hemangiomas are hemangiomas that are greater than 4 cm in diameter. While asymptomatic giant hepatic hemangioma patients can be monitored without intervention, patients that experience complications can be managed by trans-arterial embolization, radiofrequency ablation, surgical resection, or enucleation. Although there is no consensus on definite medical treatment or optimal timing of surgery, liver transplantation is rarely indicated. Among giant hepatic hemangioma patients who received liver transplantation, Kasabach-Merritt syndrome (KMS), a consumptive coagulopathy associated with hemangiomas, is one of the most common indications. We present a case of giant hepatic hemangioma complicated by Kasabach-Merritt syndrome, which was successfully treated by orthotopic liver transplantation.
CASE REPORT: The patient was a 39-year-old woman with a known history of multiple giant hepatic hemangiomas who presented with abdominal pain and distension. She had life-threatening intra-abdominal hemorrhages caused by benign endometriomas due to hepatic hemangiomas complicated by Kasabach-Merritt syndrome. Despite interventional radiology embolization of a bleeding uterine artery and aggressive resuscitation with fluid and blood products, the patient’s status continued to decline. Emergent orthotopic liver transplantation was applied with subsequent resolution of the consumptive coagulopathy. She remained well at 2-month follow-up, with normal liver enzyme levels and intact liver allograft function.
CONCLUSIONS: Liver transplantation is indicated for selected patients with giant hepatic hemangioma complicated by KMS; despite the high surgical risk, outcomes seem favorable.
Keywords: Hemangioma, Kasabach-Merritt syndrome, Liver Transplantation, Adult, Disseminated Intravascular Coagulation, Female, Hemangioma, Cavernous, Hemoperitoneum, Humans, Liver Neoplasms
Background
Liver hemangiomas are the most common benign liver tumor, with highest incidence among women in the fourth decade of life [1]. Giant liver hemangiomas have a diameter greater than 4 cm. There is no consensus on definite medical treatment or optimal timing of surgery for liver hemangiomas. The majority of patients are managed expectantly; in rare occasions, liver transplantation is indicated. This case highlights a patient with unresectable giant hepatic hemangioma complicated by Kasabach-Merritt syndrome (KMS) who was treated with orthotopic liver transplantation.
Case Report
The patient was a 39-year-old woman with a known history of multiple giant hepatic hemangiomas, KMS, and endometriomas. In 2019, the patient was found to have multiple hepatic hemangiomas (largest diameter: 10.8 cm) during a workup for female infertility after taking oral contraceptive pills for years. She underwent elective laparoscopy for resection of an ovarian endometrioma and uterine fibroids and developed hemorrhagic shock postoperatively. The patient required a massive blood transfusion and a repeated laparotomy to achieve hemostasis. Laboratory data revealed disseminated intravascular coagulopathy, consistent with KMS. She made a full recovery and had regular follow-ups with Hepatology and Hematology, which decided not to recommend a liver transplant, as her condition was stable.
The patient presented to the Emergency Department in August 2021 for acute onset abdominal pain and distention. Laboratory data on admission revealed a platelet count of 135×103/µL of blood, a prothrombin time of 22.6 s, an INR of 2.1, and a fibrinogen level of 71 mg/dL, consistent with consumptive coagulopathy. An abdominal computed tomography scan showed innumerable solid and cystic masses throughout the liver, with the largest one measuring 14.3×14.6×14.9 cm (Figure 1). In addition, there was active arterial extravasation into enlarged right adnexa and hemoperitoneum. The patient underwent an emergent coil embolization of a right uterine artery branch by an interventional radiologist. Despite aggressive resuscitation with fluid and blood products, her condition continued to deteriorate, and she developed abdominal compartment syndrome with a peak bladder pressure greater than 30 mmHg. Emergent paracentesis yielded grossly bloody fluid with no evidence of malignancy. The patient was started on high-dose steroids for persistent coagulopathy.
The patient was listed for a liver transplant earlier in the hospital course. However, her acute life-threatening hemorrhage from KMS-associated benign endometriomas was not reflected by the model for end-stage liver disease (MELD) score of 24. A MELD exception status was applied, and the patient underwent a total hepatectomy and orthotopic liver transplant on hospital day 13. A total of 9300 g of liver with multiple cavernous hemangiomas were removed. During surgery, the patient received 8 units of packed red blood cells, 11 fresh frozen plasma units, 4 cryoprecipitate units, and 4 units of platelets. Her coagulopathy improved immediately following surgery, and the patient was discharged 8 days after liver transplant. She underwent a liver biopsy about 1 month after surgery for up-trending liver enzymes, which was negative for acute cellular rejection. The patient was doing well at her 2-month follow-up appointment, with recovering liver enzyme levels.
Discussion
Liver hemangiomas can be asymptomatic; however, with an increase in size, the mass effect can cause various complications, including liver failure, respiratory distress, organ displacement, venous compression and stasis, early satiety, and peripheral edema. While asymptomatic patients can be monitored without intervention, symptomatic patients can be managed by trans-arterial embolization, radiofrequency ablation, surgical resection, enucleation, or liver transplantation [2].
Based on the United Network for Organ Sharing database, 394 liver transplantation were performed for benign liver tumors between 1989 and 2008, accounting for only 0.9% of all liver transplantations [3].
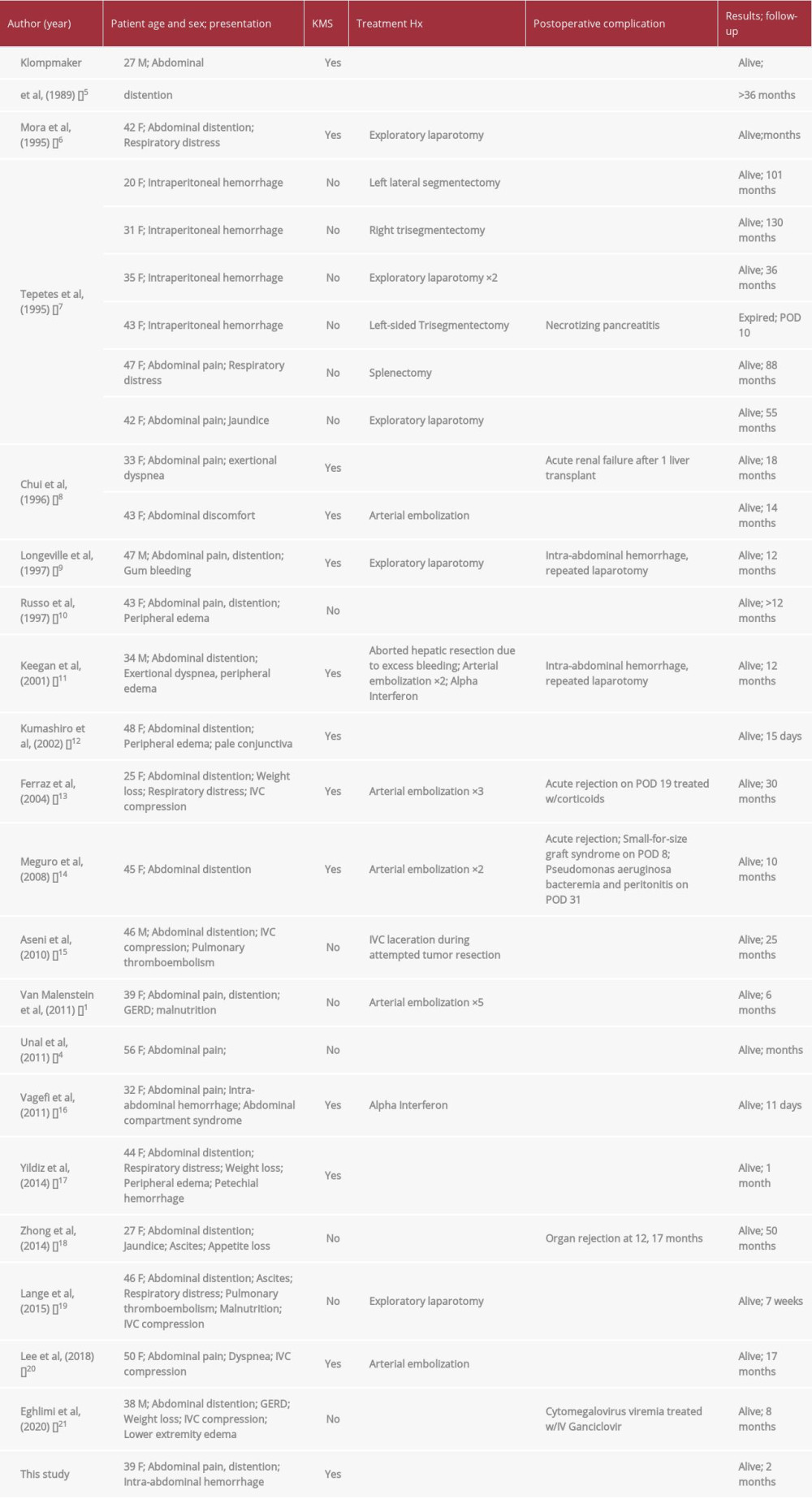
To date and to the best of the authors’ knowledge, 25 liver transplants for benign liver tumors in 19 studies have been reported in adults. Table 1 summarizes the patients’ characteristics, presentation, treatment history, outcome, and complications following liver transplant for 26 cases, including ours [1,4–21]. There were 21 female patients in the benign liver tumor transplant group. Although by no means a randomized sample, female sex hormone has been suggested to cause sexual imbalance. Multiple case reports and case series correlated pregnancy and estrogen replacement therapy with an increase in tumor size [1]. Our patient had a history of oral contraceptive use and was received 2 rounds of infertility treatments that consisted of recombinant human chorionic gonadotropin, selective estrogen receptor modulators, and progesterone, which may have contributed to rapid growth of the hepatic hemangioma. Abdominal pain and distention are the most common presentations (84.6%), followed by respiratory distress (30.8%), intra-abdominal hemorrhage (23%), weight loss, and malnutrition (23%). Two patients who presented with intra-abdominal hemorrhages developed abdominal compartment syndrome during their hospitalizations. About 20% of patients also presented with inferior vena cava compression and peripheral edema. The majority of the patients had undergone various treatments for their giant benign hepatic tumor prior to transplant. Eleven patients (42.3%) underwent abdominal surgery, including exploratory laparotomy and various degrees of hepatic resection. Six patients underwent arterial embolization, but the tumor failed to regress enough for hepatic resection. Two patients were prescribed alpha interferon treatment. Four patients (15.4%) received liver transplants from living donors, the rest from cadaveric donors. Out of the 26 cases with patient age ranging from 20 to 56 years old, only 1 patient died during the perioperative period, from necrotizing pancreatitis. Eight patients experienced liver transplant complications during the follow-up period, including acute and chronic organ rejection, repeated laparotomy to achieve hemostasis, and infections.
Most patients who underwent liver transplantations had a dominant tumor measuring greater than 4 cm in diameter. A patient reported by Unal et a. stands out among these cases as her largest tumor only measured 1.8×1.6×0.8 cm [4]. She underwent liver transplantation for what was initially thought to be hepatic cellular carcinoma based on characteristic magnetic resonance imaging and chronic hepatitis C status. After liver resection, histologic examination revealed mixed capillary-cavernous hemangioma.
KMS is one of the main indications for liver transplantation. It was present in 13 out of 26 patients. KMS was first described in 1940 as a consumptive coagulopathy associated with cutaneous hemangiomas in children [22]. The pathophysiologic event that leads to KMS is platelet trapping within a hemangioma and subsequent platelet activation and consumption of clotting factors. KMS management centers on resolving the lesion, which will lead to correction of the coagulopathy, as presented in this case. In lesions not amenable to surgery, steroids and alpha interferon are first-line therapies, followed by Vincristine and combination chemotherapy [23].
Conclusions
Liver transplantation is indicated for a small subset of patients with giant hepatic hemangioma complicated by KMS. Despite the high surgical risk, liver transplantation is a feasible option, and outcomes are favorable.
References:
1.. van Malenstein H, Maleux G, Monbaliu D, Giant liver hemangioma: The role of female sex hormones and treatment: Eur J Gastroenterol Hepatol, 2011; 23; 438-43
2.. , EASL Clinical Practice Guidelines on the management of benign liver tumours: J Hepatol, 2016; 65; 386-98
3.. Ercolani G, Grazi GL, Pinna AD, Liver transplantation for benign hepatic tumors: A systematic review: Dig Surg, 2010; 27; 68-75
4.. Unal E, Francis F, Aquino A, Liver transplant for mixed capillary-cavernous hemangioma masquerading as hepatocellular carcinoma in a patient with hepatocellular carcinoma: Exp Clin Transplant, 2011; 9; 344-48
5.. Klompmaker IJ, Sloof MJ, van der Meer J, Orthotopic liver transplantation in a patient with a giant cavernous hemangioma of the liver and Kasabach-Merritt syndrome: Transplantation, 1989; 48; 149-51
6.. Mora A, Cortés C, Roigé J, Noguer M, [Orthotopic liver transplant for giant cavernous hemangioma and Kasabach-Merritt syndrome]: Rev Esp Anestesiol Reanim, 1995; 42; 71-74 [in Spanish]
7.. Tepetes K, Selby R, Webb M, Orthotopic liver transplantation for benign hepatic neoplasms: Arch Surg, 1995; 130; 153-56
8.. Chui AK, Vass J, McCaughan GW, Sheil AG, Giant cavernous haemangioma: A rare indication for liver transplantation: Aust N Z J Surg, 1996; 66; 122-24
9.. Longeville JH, de la Hall P, Dolan P, Treatment of a giant haemangioma of the liver with Kasabach-Merritt syndrome by orthotopic liver transplant a case report: HPB Surg, 1997; 10; 159-62
10.. Russo MW, Johnson MW, Fair JH, Brown RS, Orthotopic liver transplantation for giant hepatic hemangioma: Am J Gastroenterol, 1997; 92; 1940-41
11.. Keegan MT, Kamath GS, Vasdev GM, Liver transplantation for massive hepatic haemangiomatosis causing restrictive lung disease: Br J Anaesth, 2001; 86; 431-34
12.. Kumashiro Y, Kasahara M, Nomoto K, Living donor liver transplantation for giant hepatic hemangioma with Kasabach-Merritt syndrome with a posterior segment graft: Liver Transpl, 2002; 8; 721-24
13.. Ferraz AA, Sette MJ, Maia M, Liver transplant for the treatment of giant hepatic hemangioma: Liver Transpl, 2004; 10; 1436-37
14.. Meguro M, Soejima Y, Taketomi A, Living donor liver transplantation in a patient with giant hepatic hemangioma complicated by Kasabach-Merritt syndrome: Report of a case: Surg Today, 2008; 38; 463-68
15.. Aseni P, Lauterio A, Slim AO, Life-saving super-urgent liver transplantation with replacement of retrohepatic vena cava by dacron graft: HPB Surg, 2010; 2010; 828326
16.. Vagefi PA, Klein I, Gelb B, Emergent orthotopic liver transplantation for hemorrhage from a giant cavernous hepatic hemangioma: Case report and review: J Gastrointest Surg, 2011; 15; 209-14
17.. Yildiz S, Kantarci M, Kizrak Y, Cadaveric liver transplantation for a giant mass: Gastroenterology, 2014; 146; e10-11
18.. Zhong L, Men TY, Yang GD, Case report: Living donor liver transplantation for giant hepatic hemangioma using a right lobe graft without the middle hepatic vein: World J Surg Oncol, 2014; 12; 83
19.. Lange UG, Bucher JN, Schoenberg MB, Orthotopic liver transplantation for giant liver haemangioma: A case report: World J Transplant, 2015; 5; 354-59
20.. Lee JH, Yoon CJ, Kim YH, Living-donor liver transplantation for giant hepatic hemangioma with diffuse hemangiomatosis in an adult: A case report: Clin Mol Hepatol, 2018; 24; 163-68
21.. Eghlimi H, Arasteh P, Azade N, Orthotopic liver transplantation for management of a giant liver hemangioma: A case report and review of literature: BMC Surg, 2020; 20; 142
22.. Inglefield JT, Tisdale PD, Fairchild JP, A case of hemangioma with thrombocytopenia in the newborn infant treated by total excision. Review of the literature: J Pediatr, 1961; 59; 238-42
23.. Hall GW, Kasabach-Merritt syndrome: Pathogenesis and management: Br J Haematol, 2001; 112; 851-62
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133