18 July 2022: Articles 
Trust the Process: Prolonged Parasitemia in an Elderly Man with Asplenia from the American Midwest
Unusual clinical course, Challenging differential diagnosis, Unusual or unexpected effect of treatment, Educational Purpose (only if useful for a systematic review or synthesis)
Marko Ivancich1DEF*, Larry Lutwick2ABD, F.N.U. Shweta3ABCDEFDOI: 10.12659/AJCR.936326
Am J Case Rep 2022; 23:e936326






Abstract
BACKGROUND: Babesia species are intraerythrocytic parasitic protozoa that are endemic to the Northeast and north Midwest of the United States. Babesia microti is the most common cause of babesiosis in North America and causes a malaria-like tick-borne parasitosis. Babesia is commonly transmitted through the bite of Ixodes species ticks, often concomitantly with other tick-borne organisms such as Borrelia burgdorferi, Ehrlichia, Rickettsia rickettsii, and Anaplasma phagocytophilum. In the Midwest, Lyme disease is the most common tick-borne illness, and other organisms can sometimes be overlooked. The risk of tick-borne parasitic or bacterial infection is increased in patients after splenectomy.
CASE REPORT: An 89-year-old man with asplenia and multiple other comorbidities presented to the Emergency Department after a fall at home preceded by 2 to 3 days of fever and loss of appetite and 1 week of generalized weakness. The patient had thrombocytopenia, leukocytosis with neutrophilia, transaminitis, hyperbilirubinemia, and elevated creatine kinase level consistent with tick-borne illness. Laboratory testing revealed Borrelia and Babesia co-infection and other culprits were ruled out via high sensitivity PCR. Owing to the patient’s asplenic status, the babesiosis was slow to resolve with appropriate treatment. After an extended 8-week treatment with azithromycin and atovaquone, the patient demonstrated clinical resolution of babesiosis with a negative blood smear.
CONCLUSIONS: First-line treatment with azithromycin and atovaquone is effective in treating babesiosis even in complicated patients, such as this elderly, asplenic patient. However, in cases such as this, an extended course of a first-line treatment regimen is still appropriate.
Keywords: Babesia, Frail Elderly, Ixodes, Parasitemia, Splenectomy, Aged, Aged, 80 and over, Atovaquone, Azithromycin, Babesiosis, Humans, Male, Trust, United States
Background
Severe fulminant disease can occur and may result in death in immunodeficient patients, such as the elderly, asplenic patients, and those on immunosuppressing medications [1,3]. Most fatal babesiosis infections occur in the setting of a dys-functional reticuloendothelial system and insufficient innate immune response [2–4]. In this report, we detail the case of an 89-year-old asplenic man with babesiosis and possible
Case Report
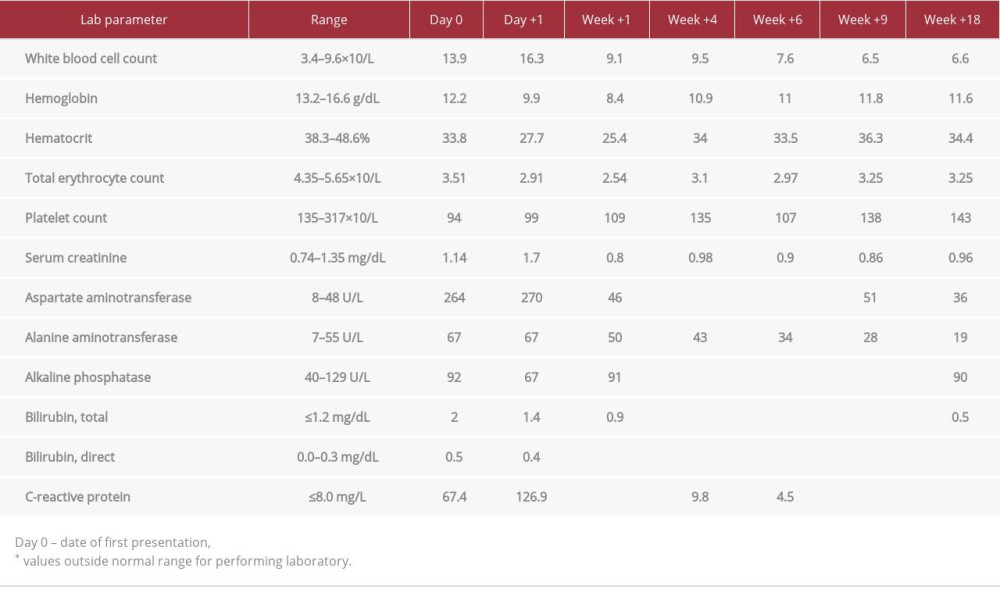
An 89-year-old asplenic man with a past medical history of coronary artery disease, chronic kidney disease, hypertension, hyperlipidemia, sinoatrial node dysfunction, obstructive sleep apnea, and basal and squamous cell skin cancers, presented to the Emergency Department after a fall at home that was preceded by 2 to 3 days of subjective fever and loss of appetite and 1 week of generalized weakness. Physical examination revealed no obvious abnormalities, other than mild tachycardia. Laboratory testing showed thrombocytopenia, leukocytosis with neutrophilia, transaminitis, hyperbilirubinemia, and an elevated creatine kinase level (Table 1). SARS-CoV-2 infection was ruled out. Further history revealed that the patient lived in rural Wisconsin near a wooded area and had 2 pet cats, one of whom lived outdoors. However, he did not recall any recent tick bite. We suspected tick-borne illness, and the patient was admitted and started empirically on doxycycline and ceftriaxone. Blood and urine cultures were negative throughout the course of treatment.
Lyme disease was diagnosed with positive IgM and IgG results on immunoblot antibody assay, based on Center for Disease Control criteria for interpretation.
On day 1 after presentation, the patient had worsening anemia and thrombocytopenia (Table 1). Due to the patient’s asplenia, a prolonged course of treatment was discussed. By day 4, the percent of parasitemia had improved to 6.13% (Figure 1), and most lab abnormalities had resolved (Table 1). However, parasitemia then increased to 7.37% two days later (Figure 1). Although discouraging, this was not completely unexpected. Treatment with atovaquone and azithromycin was continued. The course of parasitemia is demonstrated graphically in Figure 1. The parasitemia index continued to decrease thereafter, but at day 42, a blood smear still showed scant parasitemia of 0.15% (Figure 1). Peripheral blood smears were negative from day 60 onward, and antimicrobial therapy for Babesiosis was discontinued roughly 8 weeks after treatment was initiated.
Discussion
We present a case of
Recommended treatment of patients with a positive
Cases of prolonged parasitemia, such as in the case presented, have been known to relapse, sometimes even 2 years later [3]. Therefore, we suggest that providers consider follow-up examination after the apparent clearance of babesiosis. It is also important to note that co-infection with Lyme disease, transmitted by a common vector, can complicate therapy. Animal models have shown that infection with
Conclusions
In complicated cases of babesiosis with prolonged parasitosis, first-line therapy atovaquone and azithromycin should be sufficient if maintained for an adequate duration. In cases in which the parasitemia is slow to resolve, such as in our asplenic patient, a clinician may be tempted to alter treatment due to concern for treatment failure; however, first-line therapy is still recommended. Additionally, providers should have a low threshold for
References:
1.. Rosner F, Zarrabi MH, Benach JL, Habicht G, Babesiosis in splenectomized adults. Review of 22 reported cases: Am J Med, 1984; 76(4); 696-701
2.. Vannier E, Gewurz BE, Krause PJ, Human babesiosis: Infect Dis Clin North Am, 2008; 22(3); 469-88 , viii–ix
3.. Bloch EM, Kumar S, Krause PJ: Pathogens, 2019; 8(3); 102
4.. Terkawi MA, Cao S, Herbas MS: Infect Immun, 2015; 83(1); 8-16
5.. Djokic V, Akoolo L, Parveen N: Front Microbiol, 2018; 9; 85
6.. Jeong YI, Hong SH, Cho SH, Lee WJ, Lee SE: PLoS One, 2012; 7(10); e46553
7.. Wormser GP, Dattwyler RJ, Shapiro ED, The clinical assessment, treatment, and prevention of lyme disease, human granulocytic anaplasmosis, and babesiosis: Clinical practice guidelines by the Infectious Diseases Society of America: Clin Infect Dis, 2006; 43(9); 1089-134
8.. Krause PJ, Gewurz BE, Hill D, Persistent and relapsing babesiosis in immunocompromised patients: Clin Infect Dis, 2008; 46(3); 370-76
9.. Sanchez E, Vannier E, Wormser GP, Hu LT, Diagnosis, treatment, and prevention of lyme disease, human granulocytic anaplasmosis, and babesiosis: A review: JAMA, 2016; 315(16); 1767-77
10.. Djokic V, Akoolo L, Primus S: Front Microbiol, 2019; 10; 1596
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133