02 August 2022: Articles 
Contralateral Pneumonectomy 27 Years After Right Single-Lung Transplantation for Emphysema: A Case Report
Unusual clinical course, Challenging differential diagnosis, Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents, Rare disease, Educational Purpose (only if useful for a systematic review or synthesis)
Georges Boulos123ADEF, Raoul SchorerDOI: 10.12659/AJCR.936748
Am J Case Rep 2022; 23:e936748






Abstract
BACKGROUND: Following single-lung transplantation, native lung inflation can progressively develop in patients with emphysema.
CASE REPORT: A 74-year-old female patient presented with worsening dyspnea during daily activities. She underwent a right single-lung transplantation for emphysema 27 years ago. Despite recurrent episodes of acute rejection of the grafted lung, the patient had satisfactory recovery of physical fitness during that period and did not report any serious complications or respiratory symptoms. Her recent dyspnea was due to hyperinflation of the native emphysematous lung with mediastinal shift, reduction of venous blood return, and compression of the grafted lung. Although surgical lung volume reduction had resulted in temporary functional improvement 2 years ago, a completion contralateral pneumonectomy was deemed necessary to allow re-expansion of the grafted lung. After anesthesia induction and placement of a double-lumen tube, selective ventilation of the left emphysematous native lung confirmed the absence of gas exchange based on near-zero end-expiratory carbon dioxide fraction. During selective ventilation of the grafted lung, satisfactory gas exchange was achieved and pneumonectomy proceeded uneventfully under minimally-invasive thoracotomy. Immediately after anesthesia emergence and tracheal extubation, the patient experienced respiratory improvement. Continuous thoracic epidural blockade allowed pain-free mobilization and respiratory therapy to facilitate re-expansion of the grafted lung.
CONCLUSIONS: After single-lung transplantation in COPD patients, native lung hyperinflation is a well-described rare complication. Lung volume reduction including pneumonectomy can be considered a valuable treatment option.
Keywords: emphysema, Pneumonectomy, Lung Transplantation, Aged, Dyspnea, Female, Humans, Postoperative Complications, pulmonary emphysema
Background
Lung transplantation improves survival and quality of life of patients with chronic obstructive pulmonary disease (COPD). Given the shortage of donor lungs and the risk of death due to a prolonged waiting period, offering one1 pair of donor lungs for 2 candidates is an efficient way to optimize donor organs distribution based on medical urgency and recipient demographic parameters [1]. Short- and long-term survival after single and bilateral lung transplant (SLT, BLT) are quite similar in patients older than 65 years, whereas functional parameters related to lung volume capacity and diffusion capacity, as well as exercise tolerance and health-related quality of life, are better at all follow-up times in patients undergoing BLT compared to SLT [2].
Besides allograft dysfunction and surgical complications that occur within the first weeks following lung transplantation, non-small cell lung carcinoma and progressive hyperinflation can develop later in the native emphysematous lung [3]. Thoracic surgery with one-lung ventilation (OLV) is particularly challenging in patients with severe emphysema owing to dynamic gas trapping and alterations in hemodynamics that can compromise perioperative gas exchange. Given the high procedural risk and uncertain clinical benefits, this case report illustrates the “shared decision making” that brings patient’s values and preferences together with clinician expertise to determine the best care package for the individual concerned [4].
Case Report
In 1994, a woman weighing 58 kg and 169 cm tall with tobacco-associated emphysema underwent a right SLT. After several episodes of acute graft rejection, she exhibited marked improvement in pulmonary functional tests (PFTs) with adequate recovery of her physical fitness. Over the last 4 years, the immune tolerance to the SLT was well controlled under low doses of prednisone (5 mg) and tacrolimus (1 mg), but she had increasing dyspnea on mild exercise, attributed to hyperinflation of the native lung. In May 2019, she underwent non-anatomical lung volume reduction under video-assisted thoracic surgery, which resulted in temporary functional improvement. In July 2021, although gas exchange was satisfactory at rest, this 74-year-old patient was referred to our hospital with severe dyspnea (Borg dyspnea score 8/9), and walking limitation (<10 m), unresponsive to oxygen therapy. Echocardiography revealed normal left ventricular ejection fraction with no sign of pulmonary arterial hypertension. As summarized in Table 1, the PFTs confirmed a pattern of severe lung hyperinflation and non-reversible flow obstruction along with limitation in carbon oxide diffusing capacity (27% predicted value). The plain chest radiography and thoracic computed tomography scan showed bullous emphysema of the native left lung, causing rightward mediastinal deviation and compression of the grafted lung, as well as the vena cava and the heart (Figure 1). Lung scintigraphy showed very low flow in the left lung (<6% of cardiac output) with thromboembolic occlusion of the inferior left lobar artery. Besides immunosuppressive drugs, the patient was treated with inhaled bronchodilators (glycopyrronium, formoterol, beclomethasone), losartan (100 mg), and rosuvastatin (20 mg).
A completion pneumonectomy of the hyperinflated native lung was planned to allow re-expansion of the right transplanted lung. During the 3 weeks preceding surgery, the patient’s physical condition was optimized through daily home sessions of volume incentive spirometry, deep breathing exercise, and muscle strengthening of the upper and lower limbs using elastic bands. Psychological support was also provided by her family and regular phone calls with physiotherapists and the medical team.
Before surgery, nebulized salbutamol was administered and the patient was equipped with a thoracic epidural catheter (T5–T6), 2 intravenous (i.v.) lines, and a radial artery catheter for blood pressure monitoring. Epidural analgesia was initiated with bupivacaine 0.25% and fentanyl 0.002% (bolus of 6 ml) and maintained throughout surgery (5 ml/h). General anesthesia was induced with sufentanil (10 mcg), etomidate (20 mg), and rocuronium (30 mg). A double-lumen tube was inserted and proper positioning was confirmed by fiberoptic bronchoscopy. During selective ventilation through the tracheal port, the end-tidal CO2 (ETCO2) dropped to near 0, whereas during selective ventilation through the bronchial port, ETCO2 stabilized at around 4.5% and arterial oxygen saturation (SaO2) was 98–100% with an inspiratory oxygen fraction (FiO2) of 0.8. Anesthesia was maintained with inhaled sevoflurane and 100 mg hydrocortisone was administered i.v. Pressure-controlled volume-guaranteed ventilation (Aisys CS2 workstation, GE Healthcare) was initiated after performing an alveolar recruitment maneuver and setting a tidal volume of 5.5 ml/kg of predicted body weight. A positive endexpiratory pressure of 7 cmH2O was selected, which achieved the highest lung compliance. The inspiratory: expiratory ratio (1: 2) and respiratory rate (14/min) were adjusted to allow complete alveolar emptying and normocapnia. Right pneumonectomy was carried out through an antero-lateral intercostal approach. Hemodynamics, oxygenation index (SaO2/FiO2) and ETCO2 remain within normal physiological range, even following clamping of the right pulmonary artery (Table 2). At the end of a 70-min uneventful procedure, complete recovery of the neuromuscular block was confirmed (Train-Of-Four ratio > 0.9 upon stimulation of the ulnar nerve). The estimated blood loss was less than 150 ml and 650 ml i.v. crystalloids was given. After a last alveolar recruitment maneuver, the patient was extubated and transferred to the Post-Anesthesia Care Unit.
Postoperatively, the patient reported immediate improvement in spontaneous breathing, with normocapnia and satisfactory oxygenation (Table 2), while chest X-rays showed re-expansion of the grafted lung and a shift of the trachea and heart to a more central position. The chest tube was removed 6 h postoperatively and 4 h later the chest radiogram demonstrated fluid accumulation in the left pleural cavity (Figure 2) that required a thoracocentesis to remove 500 ml of clear fluid with no evidence of infection. On the third day after surgery, the onset of atrial fibrillation required pharmacological cardioversion (amiodarone 300 mg i.v.). The patient was discharged to a rehabilitation center on the tenth postoperative day. One month later, her 6-minute walking capacity had increased above 300 m and she had full autonomy in her daily functional activities.
Discussion
According to the International Society for Heart and Lung Transplantation Registry, SLT is performed in up to 40% of patients with end-stage COPD [5]. Native lung hyperinflation compressing the grafted lung represents a unique complication that develops in 5–30% of COPD patients following SLT [6,7]. Dead space ventilation, restricted functional alveolar areas, and impaired venous blood return all contribute to produce dyspnea, respiratory muscle fatigue, and poor exercise capacity. Several case series have reported functional improvements after surgical lung volume reduction that was associated with high early morbidity (eg, infection, air leaks, and renal failure) requiring intensive care, and reduced survival at 1 year (58%) [8].
Contralateral pneumonectomy after SLT has been reported in only 3 patients (ages 46, 56, and 66 years (Table 3) [9–11]. Intractable air leak was incriminated in 1 case (17 days after SLT) [11] and progressive hyperinflation of the native lung in the other 2 patients (3 years and 12 years after SLT) [9,10]. In our patient, clinical improvement was achieved transiently after lung volume reduction and she underwent completion pneumonectomy 27 years after right SLT.
Preoperatively, the expected clinical benefits associated with removal of the native hyperinflated lung lead the multidisciplinary board involving thoracic surgeons, anesthesiologists, and chest physicians to propose a pneumonectomy via a minimally-invasive thoracotomy. Pulmonary hypertension, significant cardiovascular disease (eg, heart failure and coronary artery disease) or other organ failure (eg, liver and kidney) that could have contraindicated surgery were absent, and the fully informed patient chose to undergo surgery [12]. Besides advanced age, immunosuppression, and poor pulmonary function, muscular deconditioning was the only potentially reversible risk factor. Accordingly, a home-based physical training program with psychological support was initiated 3 weeks before surgery to empower the patient as an active partner in her health care process and to strengthen respiratory muscles to prevent postoperative pulmonary complications [13]. To reduce the administration of opiates and allow a smooth anesthesia emergence, thoracic epidural analgesia was used intraoperatively and was continued in the early postoperative period to facilitate re-expansion of the grafted lung with exercise [14]. Alternatively, a paravertebral thoracic block might have been considered [15]. Inhalational anesthesia was preferred to intravenous anesthetics given the bronchodilating and organ preconditioning effects of volatile anesthetic agents resulting in fewer postoperative pulmonary and neurocognitive disturbances [16,17]. After anesthesia induction, the lungs were isolated with a double-lumen tube and the sharp drop end-tidal CO2, while ventilating the left native lung confirmed the absence of blood flow through the left pulmonary artery and total non-functionality of the left lung. On the grafted right lung, an open protective ventilatory strategy was applied, including low VT, titrated PEEP, and alveolar recruitment maneuver to minimize ventilation-induced lung injury [18]. Interestingly, Friedrich et al recently reported their unique experience using laryngeal masks and providing assisted ventilation in 20 patients undergoing anatomical lung resection, including 1 pneumonectomy- via video-assisted thoracoscopic surgery [19]. Compared with controlled mechanical ventilation, assisted spontaneous breathing can lower the risk of ventilatory-lung injuries by reducing inspiratory support pressure, ensuring stable hemodynamics by improving venous return and facilitating postoperative recovery by reducing the need for neuromuscular-blocking drugs. These advantages have to be weighed against unexpected ventilator-patient asynchrony during surgical manipulation and the need to proceed to urgent intubation in case of severe adverse events (eg, acute bleeding and hypoxemia) [20].
Conclusions
Postoperatively, our patient exhibited impressive functional improvements allowing her to resume her daily activities and to ensure her complete autonomy at home. After SLT in COPD patients with native lung hyperinflation, lung volume reduction and pneumonectomy as a last resort are considered valuable treatment options. Given the high risk of adverse events in these unusual situations, a patient-oriented multidisciplinary approach should include preoperative patient counseling and physical fitness preparation as well as perioperative protective interventions by experienced thoracic surgeons and anesthesiologists.
Figures
References:
1.. Schaffer JM, Singh SK, Reitz BA, Single- vs double-lung transplantation in patients with chronic obstructive pulmonary disease and idiopathic pulmonary fibrosis since the implementation of lung allocation based on medical need: JAMA, 2015; 313(9); 936-48
2.. Thabut G, Christie JD, Ravaud P, Survival after bilateral versus single-lung transplantation for idiopathic pulmonary fibrosis: Ann Intern Med, 2009; 151(11); 767-74
3.. De Groote A, Van Muylem A, Scillia P, Ventilation asymmetry after transplantation for emphysema: Role of chest wall and mediastinum: Am J Respir Crit Care Med, 2004; 170(11); 1233-38
4.. Sturgess J, Clapp JT, Fleisher LA, Shared decision-making in peri-operative medicine: A narrative review: Anaesthesia, 2019; 74(Suppl. 1); 13-19
5.. Benvenuto LJ, Costa J, Piloni D, Right single lung transplantation or double lung transplantation compared with left single lung transplantation in chronic obstructive pulmonary disease: J Heart Lung Transplant, 2020; 39(9); 870-77
6.. Yonan NA, el-Gamel A, Egan J, Single lung transplantation for emphysema: Predictors for native lung hyperinflation: J Heart Lung Transplant, 1998; 17(2); 192-201
7.. Siddiqui FM, Diamond JM, Lung transplantation for chronic obstructive pulmonary disease: Past, present, and future directions: Curr Opin Pulm Med, 2018; 24(2); 199-204
8.. Kapelanski DP, Anderson MB, Kriett JM, Volume reduction of the native lung after single-lung transplantation for emphysema: J Thorac Cardiovasc Surg, 1996; 111(4); 898-99
9.. Abi Jaoude W, Tiu B, Strieter N, Maloney JD, Thoracoscopic native lung pneumonectomy after single lung transplant: initial experience with 2 cases: Eur J Cardiothorac Surg, 2016; 49(1); 352-54
10.. Liu F, Ruan Z, Wang S, Lin Q, Right native lung pneumonectomy due to over inflation three years after left single lung transplantation for pulmonary lymphangioleiomyomatosis: Ann Thorac Cardiovasc Surg, 2014; 20(1); 70-73
11.. Novick RJ, Menkis AH, Sandler D, Contralateral pneumonectomy after single-lung transplantation for emphysema: Ann Thorac Surg, 1991; 52(6); 1317-19
12.. Licker M, Triponez F, Diaper J, Preoperative evaluation of lung cancer patients: Current Anesthesiology Reports, 2014; 4(2); 124-34
13.. Assouline B, Cools E, Schorer R, Preoperative exercise training to prevent postoperative pulmonary complications in adults undergoing major surgery. A systematic review and meta-analysis with trial sequential analysis: Ann Am Thorac Soc, 2021; 18(4); 678-88
14.. Freise H, Van Aken HK, Risks and benefits of thoracic epidural anaesthesia: Br J Anaesth, 2011; 107(6); 859-68
15.. Huan S, Deng Y, Wang J, Ji Y, Yin G, Efficacy and safety of paravertebral block versus intercostal nerve block in thoracic surgery and breast surgery: A systematic review and meta-analysis: PLoS One, 2020; 15(10); e0237363
16.. Pang QY, Duan LP, Jiang Y, Liu HL, Comparison of outcomes after breast cancer surgery between inhalational and propofol-based intravenous anaesthesia: A systematic review and meta-analysis: J Pain Res, 2021; 14; 2165-77
17.. Sun H, Zhang G, Ai B, A systematic review: Comparative analysis of the effects of propofol and sevoflurane on postoperative cognitive function in elderly patients with lung cancer: BMC Cancer, 2019; 19(1); 1248
18.. Peel JK, Funk DJ, Slinger P, Tidal volume during 1-lung ventilation: A systematic review and meta-analysis: J Thorac Cardiovasc Surg, 2022; 163(4); 1573-85.e1
19.. Friederich P, Fuchsgruber F, Hiebinger A, Ventilator settings and arterial blood gases during video-assisted thoracoscopic surgery including pneumonectomy with pressure support ventilation: Br J Anaesth, 2020; 125(5); e416-17
20.. Wang C, Wu D, Pang P, Spontaneous ventilation video-assisted thoracoscopic surgery for geriatric patients with non-small-cell lung cancer: J Cardiothorac Vasc Anesth, 2022; 36(2); 510-17
19.. Brunelli A, Kim AW, Berger KI, Addrizzo-Harris DJ, Physiologic evaluation of the patient with lung cancer being considered for resectional surgery: Diagnosis and management of lung cancer, American College of Chest Physicians evidence-based clinical practice guidelines: Chest, 2013; 143; e166S-90S
20.. Colice GL, Shafazand S, Griffin JP, Physiologic evaluation of the patient with lung cancer being considered for resectional surgery: ACCP evidenced-based clinical practice guidelines (2nd edition): Chest, 2007; 132; 161S-77S
Figures
Tables
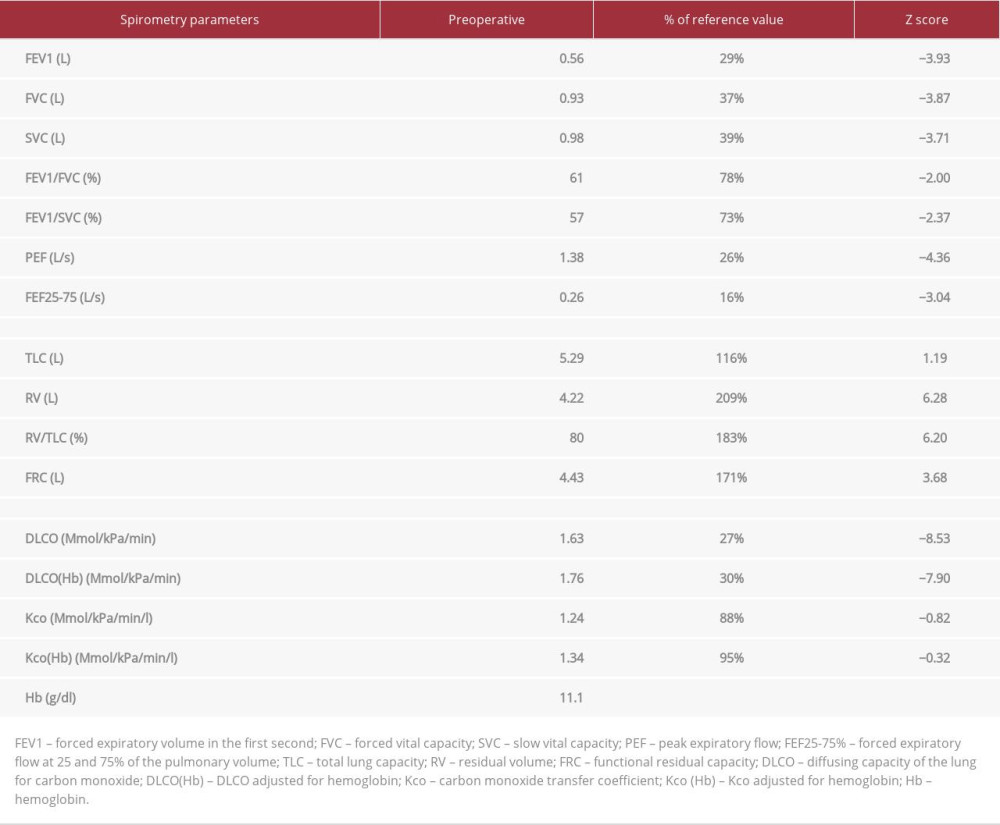 Table 1.. Patient’s pulmonary function tests preoperatively.
Table 1.. Patient’s pulmonary function tests preoperatively.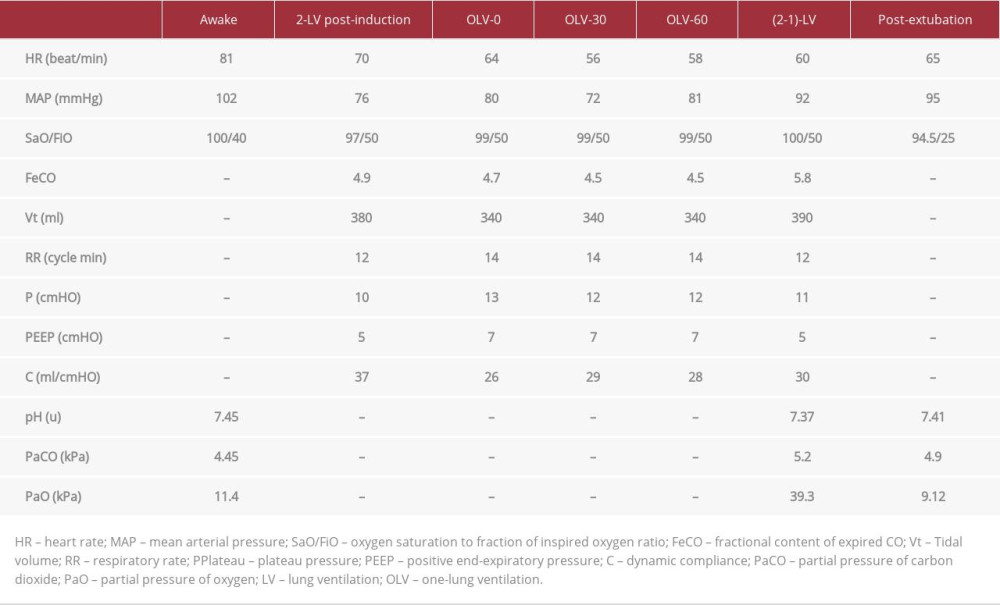 Table 2.. Perioperative hemodynamic and respiratory data.
Table 2.. Perioperative hemodynamic and respiratory data.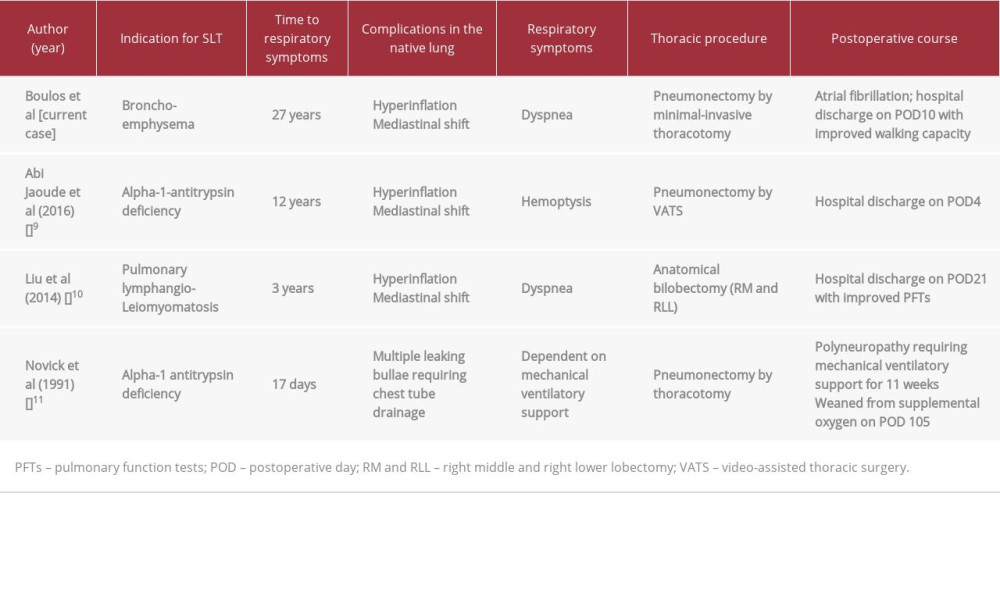 Table 3.. Reported cases of pneumonectomy after single-lung transplantation and native lung hyperinflation.Table 1.. Patient’s pulmonary function tests preoperatively.Table 2.. Perioperative hemodynamic and respiratory data.Table 3.. Reported cases of pneumonectomy after single-lung transplantation and native lung hyperinflation.
Table 3.. Reported cases of pneumonectomy after single-lung transplantation and native lung hyperinflation.Table 1.. Patient’s pulmonary function tests preoperatively.Table 2.. Perioperative hemodynamic and respiratory data.Table 3.. Reported cases of pneumonectomy after single-lung transplantation and native lung hyperinflation. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report  22,760,204
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133