03 September 2022: Articles 
Milk-Alkali Syndrome: How Electronic Medical Record Open Notes Helped to Rule Out Cancer
Challenging differential diagnosis, Management of emergency care, Rare disease, Adverse events of drug therapy
Michelle-Ashley Rizk1AEF, Nicholas Abourizk1AEF, Iuliia Kovalenko1EF*, Konstantin GolubykhDOI: 10.12659/AJCR.936969
Am J Case Rep 2022; 23:e936969






Abstract
BACKGROUND: Milk-alkali syndrome is caused by excessive consumption of calcium and absorbable alkali and typically presents as a triad of hypercalcemia, acute renal failure, and metabolic alkalosis. In the era of histamine receptor blockers and proton pump inhibitors, the incidence of milk-alkali syndrome has decreased. However, the disease has not been eliminated, due to existing calcium-containing therapies. Here, we present a case of severe milk-alkali syndrome with a challenging initial diagnosis.
CASE REPORT: We present the case of a 64-year-old man who came to the hospital with encephalopathy. Serologic evaluation revealed acute renal failure, severe hypercalcemia, and metabolic alkalosis. He underwent volume resuscitation, with the initiation of calcitonin. Despite our efforts, the patient developed anuria and proceeded to intermittent hemodialysis. His workup was unrevealing, including an appropriately suppressed parathyroid hormone level, low vitamin D, and normal serum protein electrophoresis and angiotensin converting enzyme levels. Considering his persistent encephalopathy, the team was unable to obtain information from the patient regarding his calcium intake. However, at home, the patient’s significant other read his progress notes in the electronic medical record and reported that he consumed at least 1 bottle of calcium carbonate (Tums) every week. Once the encephalopathy resolved, the patient confirmed this information.
CONCLUSIONS: The search for malignancy in the setting of hypercalcemia was ceased because of the family’s at-home electronic medical record use and reporting of Tums overuse. Milk-alkali syndrome, although a rarity, should not be forgotten as a cause of hypercalcemia.
Keywords: Calcium Carbonate, electronic health records, Gastroesophageal Reflux, Hypercalcemia, Acute Kidney Injury, Alkalosis, Brain Diseases, Humans, Male, Middle Aged, Neoplasms
Background
Milk-alkali syndrome is caused by excessive consumption of calcium and absorbable alkali and typically presents as a triad of hypercalcemia, acute renal failure, and metabolic alkalosis. This disease’s name originates from the 20th century, when a new regimen began gaining popularity for the treatment and relief of peptic ulcer disease. This regimen was known as “Sippy’s method” and consisted of milk, bicarbonate, and calcium carbonate. Fortunately, many years later, with the development of histamine receptor blockers and proton-pump inhibitors, milk-alkali has become an infrequent syndrome. However, some data show that it remains third among the most common causes of hypercalcemia [1,2]. This case report emphasizes the importance of broadening the differential diagnosis of hypercalcemia with a thorough medical history. We describe the case of a middle-aged man who presented with lethargy and altered mental status after excessive ingestion of calcium for uncontrolled gastroesophageal reflux disease (GERD).
Case Report
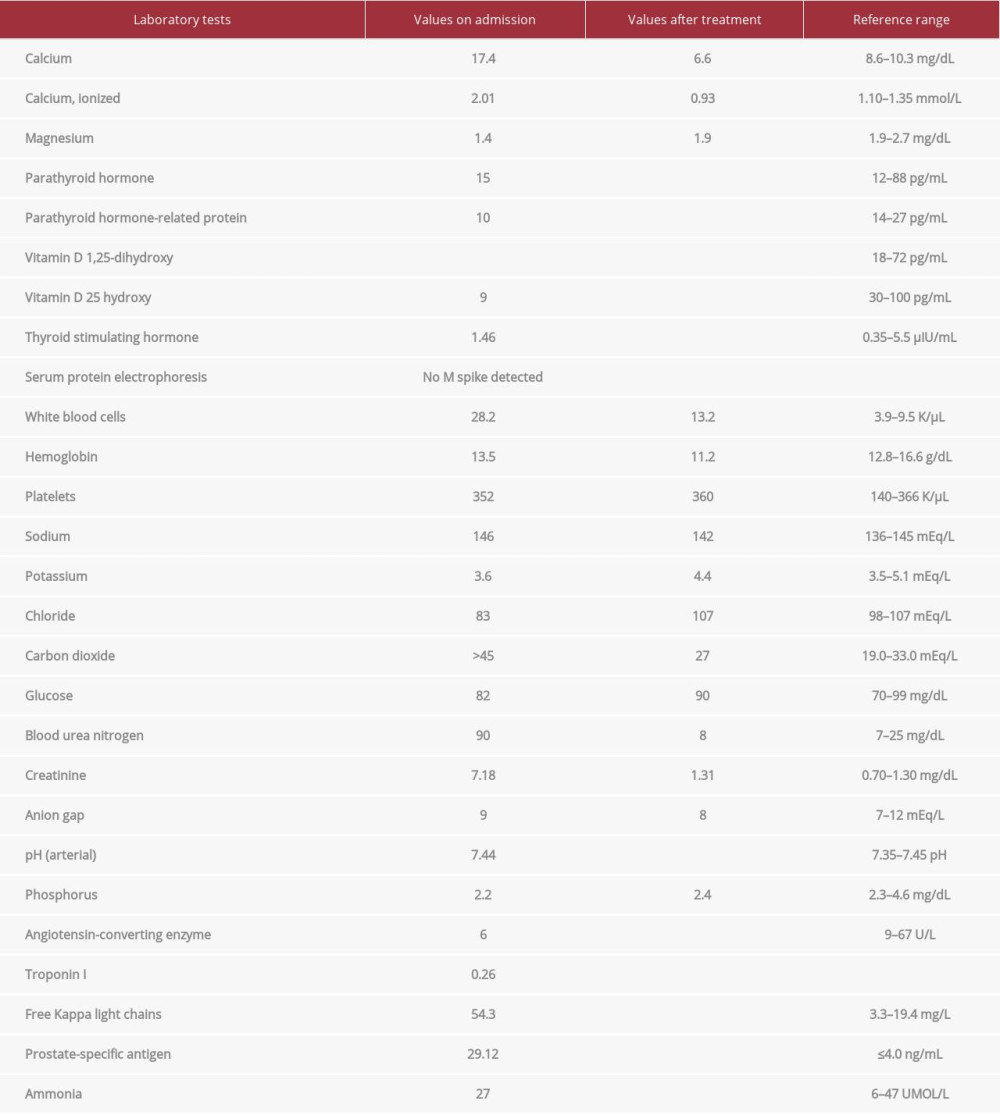
A 64-year-old man presented to the hospital with confusion, ataxia, and dysarthria. A stroke alert was called for acute encephalopathy, but stroke was ruled out. Initial serological studies in the Emergency Department revealed significant hypercalcemia with a calcium level of 17.4 mg/dL, and serum creatinine level of 7.18 mg/dL (baseline of 1.3 mg/dL). Arterial blood gas levels showed metabolic alkalosis and respiratory compensation, with pH of 7.58, pCO2 of 62 mEq/L, and HCO3 of 58 mEq/L. Significant laboratory values during hospital admission are shown in Table 1. He underwent aggressive volume resuscitation with crystalloids and calcitonin, and acetazol-amide was initiated. Hypercalcemia in the setting of malignancy was high on the differential diagnosis; therefore, paraproteinemia and multiple myeloma studies were ordered. In the milieu of recalcitrant renal failure, the patient was started on intermittent hemodialysis. He developed atrial fibrillation, with rapid ventricular response with hemodynamic instability, and was transferred to the Intensive Care Unit. His hypercalcemia improved with intermittent hemodialysis and 1 dose of zoledronic acid. Since the patient remained confused, a lumbar puncture was done to rule out inflammatory conditions. His lumbar puncture was negative for bacterial, viral, and fungal causes, but revealed elevated protein levels. A paraneoplastic assay was sent. The workup showed a suppressed parathyroid hormone (PTH) level, low vitamin D level, mildly elevated free light chains, normal angiotensin-converting enzyme levels, and no M-spike on serum protein electrophoresis. Hematologyoncology specialists believed that the suspicion for multiple myeloma was low and suggested a nuclear bone scan owing to an elevated prostate-specific antigen level and computed tomography scan findings of an enlarged prostate. Over the course of several days, the patient’s urine output improved, and intermittent hemodialysis was discontinued.
The patient’s significant other came to the hospital and indicated that she had been reading the patient’s progress notes in his electronic medical record at home. She stated that he had a long-standing history of GERD and consumed at least 1 bottle of TUMS (calcium carbonate) per week. As his encephalopathy improved gradually over subsequent days, the patient confirmed his excessive use of TUMS. The diagnosis of milk-alkali syndrome was made, which explained the hypercalcemia and associated encephalopathy. The patient’s laboratory workup after treatment is shown in Table 1. He was medically stable and eventually discharged home.
Discussion
Around 90% of causes of hypercalcemia, a common clinical problem, are related to malignancy and hyperparathyroidism [3]. However, from 8% to 38% of cases can be attributed to milk- alkali syndrome, a condition resulting from an excessive amount of calcium and alkali intake [1,2]. The incidence is thought to be related to the availability of over-the-counter calcium-containing preparations for osteoporosis and GERD. Risk factors include older age, postmenopausal state, pregnancy, hemodialysis, eating disorders, and history of transplantation [4–6].
Milk-alkali syndrome consists of a triad that involves hypercalcemia, metabolic alkalosis, and acute kidney injury. Mechanisms implicated in the clinical picture development are impaired calcium metabolism in the gut, kidneys, and bones in the setting of excessive intake of calcium and absorbable alkali [7,8]. Physiological calcium homeostasis requires more than 4 g of daily calcium intake, which suppresses calcitriol and permits achievement of normal serum levels. However, when calcium consumption exceeds 10 to 15 mg a day, suppressed calcitriol does not prevent the absorption of an excessive amount of calcium [9] but eventually leads to hypercalcemia, which causes further pathophysiologic changes underlying milk-alkali syndrome. The key event of the condition is calcium-induced diuresis, which stimulates renal bicarbonate absorption, leading to volume depletion and alkalosis in the setting of increased absorbable alkali intake [10]. Mechanisms underlying these events include calcium-induced vasoconstriction reducing the glomerular filtration rate; activation of calcium-sensing receptors located in medullary thick ascending limb, which leads to natriuresis via inhibition of the sodium-potassium-calcium transporter; and suppression of antidiuretic hormone-mediated free water absorption in the collecting duct [10]. Alkalemia further contributes to increased calcium absorption via a pH-sensitive calcium channel called the transient receptor potential vanilloid member 5 [11].
Despite having a wide range of metabolic changes, patients can remain asymptomatic, with electrolyte and acid-base derangements being found incidentally. The classic clinical picture of milk-alkali syndrome includes nausea, vomiting, weakness, and acute encephalopathy [12]. Persistent hypercalcemia in patients with prolonged calcium intake can lead to chronic milk-alkali syndrome, also known as Burnett’s syndrome. Milk-alkali syndrome can cause acute, subacute, and chronic hypercalcemia. Acute encephalopathy caused by hypercalcemia is a known phenomenon of milk-alkali syndrome. Acute manifestation of milk-alkali syndrome includes apathy, confusion, and irritability, while the chronic form can present as calcium deposition in solid organs or tissues [13]. Rare cases of milk-alkali syndrome have been reported in which patients presented with posterior reversible encephalopathy syndrome and seizures [14,15].
Diagnosis of milk-alkali syndrome requires the presence of hypercalcemia, metabolic alkalosis, and acute kidney injury due to calcium preparation and/or absorbable alkali in-take. Hypophosphatemia, hypomagnesemia, and appropriately suppressed PTH are commonly observed and support the diagnosis [12].
The mainstay of treatment is discontinuation of calcium and absorbable alkali preparations followed by appropriate volume repletion with physiologic solutions, which usually leads to complete resolution of the clinical problem. In more severe cases, treatment with furosemide to increase calcium excretion can be beneficial [16].
Conclusions
What began as a search for malignancy in the setting of hypercalcemia was quickly ceased with the help of the patient’s electronic medical record use at home and reporting of calcium intake. Milk-alkali syndrome, although not commonly encountered, should not be forgotten as a cause of hypercalcemia.
References:
1.. Picolos MK, Lavis VR, Orlander PR, Milk-alkali syndrome is a major cause of hypercalcaemia among non-end-stage renal disease (non-ESRD) inpatients: Clin Endocrinol (Oxf), 2005; 63; 566-76
2.. Zagzag J, Hu MI, Fisher SB, Perrier ND, Hypercalcemia and cancer: Differential diagnosis and treatment: Cancer J Clin, 2018; 68(5); 377-86
3.. Khairallah W, Fawaz A, Brown EM, El-Hajj Fuleihan G, Hypercalcemia and diabetes insipidus in a patient previously treated with lithium: Nat Clin Pract Nephrol, 2007; 3; 397-404
4.. Medarov BI, Milk-alkali syndrome: Mayo Clin Proc, 2009; 84; 261-67
5.. Wang M, Cho C, Gray C, Milk-alkali syndrome: A ‘quick ease’ or a ‘long-lasting problem’: Endocrinol Diabetes Metab Case Rep, 2020; 2020; EDM20-0028
6.. Waked A, Geara A, El-Imad B, Hypercalcemia, metabolic alkalosis and renal failure secondary to calcium bicarbonate intake for osteoporosis prevention – ‘modern’ milk alkali syndrome: A case report: Cases J, 2009; 2; 6188
7.. Felsenfeld AJ, Levine BS, Milk alkali syndrome and the dynamics of calcium homeostasis: Clin J Am Soc Nephrol, 2006; 1; 641-54
8.. Houillier P, Froissart M, Maruani G, Blanchard A, What serum calcium can tell us and what it can’t: Nephrol Dial Transplant, 2006; 21; 29-32
9.. Bronner F, Mechanisms of intestinal calcium absorption: J Cell Biochem, 2003; 88; 387-93
10.. Zayed RF, Millhouse PW, Kamyab F, Calcium-alkali syndrome: Historical review, pathophysiology and post-modern update: Cureus, 2021; 13(2); e13291
11.. Riccardi D, Brown EM, Physiology and pathophysiology of the calcium-sensing receptor in the kidney: Am J Physiol Renal Physiol, 2010; 298; F485-99
12.. Patel AM, Adeseun GA, Goldfarb S, Calcium-alkali syndrome in the modern era: Nutrients, 2013; 5(12); 4880-93
13.. Timilsina B, Tachamo N, Parajuli PR, Gabriely I, Acute milk-alkali syndrome: Endocrinol Diabetes Metab Case Rep, 2018; 2018(1); 18-0075
14.. Vu K, Becker G, Eagerton D, A 39 year-old woman with milk-alkali syndrome complicated by posterior reversible encephalopathy syndrome: Bone Rep, 2020; 12; 100278
15.. Nardone R, Brigo F, Trinka E, Acute symptomatic seizures caused by electrolyte disturbances: J Clin Neurol, 2016; 12(1); 21-33
16.. Malcolm OT, Identification, treatment, and prevention of calcium-alkali syndrome in elderly patients: Consult Pharm, 2015; 30; 444-54
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133