24 November 2022: Articles 
A Rare Presentation of Recalcitrant Oropharyngeal Stenosis in a 54-Year-Old Male Patient Following Transoral Robotic Surgery for Obstructive Sleep Apnea
Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents, Educational Purpose (only if useful for a systematic review or synthesis)
Pietro CanziDOI: 10.12659/AJCR.937123
Am J Case Rep 2022; 23:e937123






Abstract
BACKGROUND: Transoral robotic surgery (TORS) is an effective and safe option for obstructive sleep apnea syndrome (OSAS) patients with isolated retrolingual obstruction, as well as part of multilevel surgical approach in case of multilevel obstruction. Stenosis after TORS in OSAS patients is rarely described and no literature review has investigated this dramatic untoward event.
CASE REPORT: We report on a case of severe recalcitrant oropharyngeal stenosis after multilevel surgery with transoral robotic tongue base resection in an OSAS patient, leading to tracheotomy and gastrostomy dependence. Following the failure of numerous conservative therapeutic attempts, oropharyngeal patency was restored after extensive scar tissue removal through an open-neck approach, followed by a pharyngeal reconstruction with radial forearm free flap (RFFF).
CONCLUSIONS: Recalcitrant oropharyngeal stenosis is a dramatic complication that must be considered in OSAS patients submitted to TORS in a multilevel strategy and that is rarely described in the literature. A thorough review of the existing literature is presented to assess which factors are involved and the therapeutic strategies invoked in this scenario. The adoption of resection tools suited for robot-assisted surgery and the staging of TORS in case of multilevel surgery could decrease the risk of extensive scar formation. To date there is still no broad consensus on which therapeutic choice is the best for recalcitrant oropharyngeal stenosis. When minimally invasive treatments fail, a wide scar resection with a RFFF oropharyngeal reconstruction could be considered as a valuable option to restore the upper aerodigestive tract patency.
Keywords: Oropharynx, Robotic Surgical Procedures, Sleep apnea, obstructive, Surgical Flaps, Male, Humans, Middle Aged, Constriction, Pathologic, Cicatrix, Treatment Outcome
Background
Currently, transoral robotic surgery (TORS) is an effective and safe option for adults and pediatrics patients suffering from obstructive sleep apnea syndrome (OSAS) (Figure 1) [1,2]. A recent review and meta-analysis have shown TORS to have a low rate of complications, which mainly include transient dysphagia (7.2%), bleeding (4.2%), and postoperative pharyngeal oedema (1%) [3]. Stenosis after OSAS surgery is rarely described and no review of the literature has investigated this dramatic untoward event. The following is a report of a case of severe recalcitrant oropharyngeal stenosis requiring tracheotomy and gastrostomy dependence after TORS was used as part of a multilevel surgical approach for OSAS. A thorough review of the existing literature is presented to assess which factors are involved in the development of oropharyngeal stenosis in OSAS patients after TORS and which therapeutic strategies are invoked.
Case Report
A 54-year-old micrognathic White male with OSAS underwent uvulopalatoplasty and transoral robotic tongue base resection. Unfortunately, since the surgery was performed in another hospital, we did not have a record of that surgery. The emergence of postoperative dyspnea and dysphagia due to the development of a concentric oropharyngeal stenosis led the patient to undergo tracheostomy, TORS plasty of the concentric scar tissue, and reconstruction with a buccal myomucosal graft. After the failure of these previous treatments, the patient required a laparoscopic gastrostomy and was admitted to our hospital. An upper airways endoscopy (Figure 2) and a neck CT scan (Figure 3) showed a subtotal concentric oropharyngeal stenosis, with a 10-mm craniocaudal extent. The patient underwent a transoral scar resection and a pharyngeal plasty with salivary stent positioning (Figures 4–6). On the 25th postoperative day, we removed the salivary stent. Ten days later, the endoscopic control showed the recurrence of scarring tissue, which led to a complete stenosis of the pharyngeal lumen. This happened despite the use of post-surgical medication with mitomycin-c. Considering the failure of all the previous conservative therapeutic attempts, we opted for an extensive scar tissue removal through an open-neck approach, followed by pharyngeal reconstruction with radial forearm free flap (RFFF) (Figure 7). The scar resection was done by removing the lateral and posterior walls of the oropharynx and exposing the prevertebral fascia. The RFFF was harvested according to Soutar and positioned to reconstruct the pharyngeal defect [4]. Termino-terminal microvascular surgical anastomosis was conducted between the radial artery and the superior thyroid artery and between the comitant vein and the superior thyroid vein (Figure 8). The salivary stent was then repositioned. On the 21st postoperative day, after removing the salivary stent, the patient underwent a steroid injection in the granulation tissue between the mucosa and the radial free flap. This procedure was repeated 3 times. Because of the persistence of granulation tissue, in the following months we performed 4 CO2 laser vaporization procedures, 6 stricture dilations using a Sengstaken-Blakemore tube, and 11 topical mitomycin-C applications to the neopharyngeal wall.
Finally, the patient recovered an adequate oropharyngeal patency and underwent tracheostomy and gastrostomy closure.
Discussion
Oropharyngeal stenosis is life-threatening, but fortunately is rare. We have reported a case of severe and relapsing stenosis of the oropharynx as a consequence of TORS as part of a multilevel surgical approach for OSAS. We searched for similar reports in the literature and found only a few records of postoperative stenosis following robotic surgery, performed either alone and as part of a multilevel surgery. Our review of the existing literature (Table 1) revealed a total of 6 cases of partial or complete stenosis after TORS in OSAS patients and only 1 case in TORS for oropharyngeal cancer [1,5–7]. Of the 6 cases of oropharyngeal stenosis after OSAS surgery, 5 patients underwent multilevel surgery [1,5,6]. By extending the search to cases of pharyngeal stenosis after multilevel surgery without
TORS in OSAS patients, only 2 more cases were found [8,9]. Overall, 9 cases of postoperative oropharyngeal stenosis have been reported in the literature. Out of these 9 cases, OSAS was the surgical enrolment criterion in 8 cases (88.9%), TORS was part of the surgical strategy in 7 cases (77.8%), and stenosis was associated to multilevel surgery in 7 cases (77.8%). Due to the rarity of this complication, it is not easy to draw conclusions from such a small number of cases; however, we may suppose that the cause of postoperative oropharyngeal stenosis lies in the 2 following conditions: extensive scarring and the type of patient. Extensive scarring is a consequence of both the TORS procedure and the multilevel surgery. TORS is usually performed with a monopolar cautery, and the amount of heat dissipated by the alternate electric current causes significant collateral damage to adjacent tissues and undesired effects on wound healing. Several studies have shown that monopolary cautery is associated with postoperative scar contracture and wound healing delay [10–12non-compliant with Continuous Positive Airway Pressure (CPAP]. Multilevel surgery also contributes to extensive scar formation, involving multiple and adjacent anatomical sites. OSAS patients typically have a reduced pharyngeal airway space and possible associated micrognathia. These factors contribute to the narrowing of the posterior airway space, which may lead to narrowing of the scarring tissue consequent to surgery [13].
The association between OSAS and patient’ morphology has caused a growing interest in the analysis of airway shape and dimension. In particular, there is recent evidence about the potential role of 3D imaging digital technology to identify alteration of the upper airway anatomy for better therapeutic planning [14,15]. Some authors reported that surgical techniques applied to narrow spaces can incite inflammation and injure the mucosa beyond the treated area [5,16a potential complication of multilevel, single-stage upper airway surgery involving lingual tonsillectomy in children, and to discuss the manner in which OPS may be managed successfully. DESIGN Case series with an average follow-up of 12 months. SETTING Tertiary care children’s hospital. PATIENTS Medical charts were reviewed for 104 patients who underwent lingual tonsillectomy over a 30-month period from January 1, 2007, to June 30, 2009. INTERVENTION Multilevel, single-stage upper airway surgery, including lingual tonsillectomy. MAIN OUTCOME MEASURE Development of OPS noted during office or intraoperative examination. RESULTS Forty-nine of 104 patients underwent multilevel, single-stage upper airway procedures that included lingual tonsillectomy. Four of these 49 patients developed OPS, for a complication rate of 8.2%. Three patients required pharyngoplasty (scar release, debulking of fibrotic tissue, and re-orientation of the scar]. In the case report described here, all of these potential risk factors for postoperative oropharyngeal stenosis were present.
Regarding the management of the postoperative oropharyngeal stenosis, many different procedures have been described (Table 2) [5–8,16–20]. However, the majority can be applied only in case of mild stenosis (stenosis dilation, intralesional steroids, minor scar tissue lysis). Flap reconstruction is a feasible alternative when a wide resection is needed to treat an oropharyngeal stenosis. Local flaps, such as buccal mucosal or facial artery musculomucosal flap, are the first available options in case of small-to-moderate-sized defects [21–24]. Larger defects require regional myocutaneous pedicled flaps or microvascular tissue transfer, which are all excellent options for wide oropharyngeal and hypopharyngeal reconstruction. Among these, fasciocutaneous free flaps, because of their flexibility and reliability, are a valid option in reconstructing tubular structures [25]. In our report, due to the failure of all the previous attempts to restore the pharyngeal patency, we planned an extensive scar tissue removal and a reconstruction with the RFFF. RFFF is the criterion standard method in oropharyngeal reconstructive head and neck cancer surgery [26] and is described also in oral cavity and oesophagus reconstruction after caustic injuries and burns contractures [27,28]. The thin, pliable, predominantly hairless skin of the RFFF made it suitable to our purpose and led to a good aesthetic outcome. The main limits of this type of flap are: the possibility of donor-site complications, the risk of fistula at the mucosa-skin junction, and vascular complications of the pedicle (thrombosis and/or ischemia). None of these complications occurred in our case. However, the development of granulation tissue after RFFF pharyngeal reconstruction required postoperative laser vaporizations, dilations, topical mitomycin-C, and steroid injections. Pharyngeal stricture after microvascular free flap reconstruction usually occurs at the free flap mucosal anastomosis, and the incidence has been reported to range from 5% to 22% [29].
Among the various therapeutic options available, mitomycinc alone or in combination with other treatments (eg, stricture dilation, steroids injection) is suitable as a strong inhibitor of fibroblast proliferation in wound healing processes [30–33]. In our report, the combination of these strategies allowed restoration of the neopharyngeal patency.
Conclusions
Oropharyngeal stenosis is a rare and dramatic complication that must be considered in OSAS patients submitted to TORS in a multilevel strategy. The adoption of resection tools suited for robot-assisted surgery with a decreased thermal tissue damage may be recommended to prevent untoward events related to the widest coagulation zones. In patients enrolled for OSAS multilevel surgery with a severe posterior airway space reduction, TORS may be staged to decrease the risk of extensive scar formation. Moreover, there is still no broad consensus on which therapeutic choice is the best for recalcitrant oropharyngeal stenosis. When minimally invasive treatments fail, a wide scar resection with a RFFF oropharyngeal reconstruction could be considered as a valuable option to restore the upper aerodigestive tract patency.
Figures
References:
1.. Vicini C, Montevecchi F, Campanini A, Clinical outcomes and complications associated with TORS for OSAHS: A benchmark for evaluating an emerging surgical technology in a targeted application for benign disease: ORL J Otorhinolaryngol Relat Spec, 2014; 76(2); 63-69
2.. Montevecchi F, Bellini C, Meccariello G, Transoral robotic-assisted tongue base resection in pediatric obstructive sleep apnea syndrome: Case presentation, clinical and technical consideration: Eur Arch Otorhinolaryngol, 2017; 274(2); 1161-66
3.. Meccariello G, Cammaroto G, Montevecchi F, Transoral robotic surgery for the management of obstructive sleep apnea: A systematic review and meta-analysis: Eur Arch Otorhinolaryngol, 2017; 274(2); 647-53
4.. Soutar DS, Scheker LR, Tanner NS, McGregor IA, The radial forearm flap: A versatile method for intra-oral reconstruction: Br J Plast Surg, 1983; 36(1); 1-8
5.. Lin HS, Rowley JA, Folbe AJ, Transoral robotic surgery for treatment of obstructive sleep apnea: Factors predicting surgical response: Laryngoscope, 2015; 125(4); 1013-20
6.. Muderris T, Sevil E, Bercin S, Oropharyngeal stenosis after transoral robotic lingual tonsillectomy: J Craniofac Surg, 2015; 26(3); 853-55
7.. Hay A, Migliacci J, Karassawa Zanoni D, Complications following transoral robotic surgery (TORS): A detailed institutional review of complications: Oral Oncol, 2017; 67; 160-66
8.. Santos VB, Ruffy ML, Polisar IA, Stenosis of the oropharynx treated with intralesional triamcinolone: Ear Nose Throat J, 1977; 56(4); 164-67
9.. Suh GD, Evaluation of open midline glossectomy in the multilevel surgical management of obstructive sleep apnea syndrome: Otolaryngol Head Neck Surg, 2013; 148(1); 166-71
10.. Karaman M, Gün T, Temelkuran B, Comparison of fiber delivered CO2 laser and electrocautery in transoral robot assisted tongue base surgery: Eur Arch Otorhinolaryngol, 2017; 274(5); 2273-79
11.. Benazzo M, Canzi P, Occhini A, Transoral robotic surgery with laser for head and neck cancers: A feasibility study: ORL J Otorhinolaryngol Relat Spec, 2012; 74(3); 124-28
12.. Benazzo M, Canzi P, Mauramati S, Transoral robot-assisted surgery in supraglottic and oropharyngeal squamous cell carcinoma: Laser versus monopolar electrocautery: J Clin Med, 2019; 8(12); 2166
13.. Shi S, Xia Y, Zhu M, Characterization of upper airway obstruction by fiber-optic nasolaryngoscopy and MRI in preoperative OSAHS patients: ORL J Otorhinolaryngol Relat Spec, 2014; 76(6); 321-28
14.. Lo Giudice A, Ronsivalle V, Gastaldi G, Leonardi R, Assessment of the accuracy of imaging software for 3D rendering of the upper airway, usable in orthodontic and craniofacial clinical settings: Prog Orthod, 2022; 23(1); 22
15.. Leonardi R, Lo Giudice A, Farronato M, Fully automatic segmentation of sinonasal cavity and pharyngeal airway based on convolutional neural networks: Am J Orthod Dentofacial Orthop, 2021; 159(6); 824-835.e1
16.. Prager JD, Hopkins BS, Propst EJ, Oropharyngeal stenosis: A complication of multilevel, single-stage upper airway surgery in children: Arch Otolaryngol Head Neck Surg, 2010; 136(11); 1111-15
17.. McLaughlin KE, Jacobs IN, Todd NW, Management of nasopharyngeal and oropharyngeal stenosis in children: Laryngoscope, 1997; 107(10); 1322-31
18.. Tompkins JJ, Vaughn CA, Shaikh FA, Palatopharyngoplasty with bilateral buccal mucosal graft repair to alleviate oropharyngeal stenosis: Int J Pediatr Otorhinolaryngol, 2015; 79(9); 1579-81
19.. Haller JR, Gray SD, Severe pharyngeal stenosis treated with inferiorly based sternocleidomastoid myocutaneous flap: Ann Otol Rhinol Laryngol, 1999; 108(8); 731-34
20.. Banerjee D, Wang JC, Demke JC, Novel use of tissue expander for dilation of oropharyngeal stenosis: Int J Pediatr Otorhinolaryngol, 2014; 78(11); 2018-20
21.. Sabri A, Oropharyngeal reconstruction: Current state of the art: Curr Opin Otolaryngol Head Neck Surg, 2003; 11(4); 251-54
22.. Mann RJ, O’Brien AL, Adams NS, Repair of oropharyngeal stenosis with bilateral buccal myomucosal flaps: Ann Plast Surg, 2017; 79(2); 162-65
23.. Jung BK, Song SY, Kim SH, Lateral oropharyngeal wall coverage with buccinator myomucosal and buccal fat pad flaps: Arch Plast Surg, 2015; 42(4); 453-60
24.. Asairinachan A, O’Duffy F, Li MP, Facial artery musculomucosal flaps in oropharyngeal reconstruction following salvage transoral robotic surgery: A review of outcomes: J Laryngol Otol, 2019; 133(10); 884-88
25.. Aladimi MT, Han B, Li C, Factors to consider when deciding on the type of free-flap reconstruction of head and neck soft tissue defects: ORL J Otorhinolaryngol Relat Spec, 2017; 79(4); 230-38
26.. Sweeny L, Rosenthal EL, Light T, Outcomes and cost implications of microvascular reconstructions of the head and neck: Head Neck, 2019; 41(4); 930-39
27.. Varkey P, Tan NC, Chen HC, Corrosive injury of oral cavity – a rare presentation: J Plast Reconstr Aesthet Surg, 2006; 59(10); 1110-13
28.. Ichioka S, Nakatsuka T, Minegishi Y, Microsurgical reconstruction for caustic injuries of the oral cavity and esophagus: J Reconstr Microsurg, 2000; 16(5); 357-61
29.. Annino DJ, Goguen LA, Mitomycin C for the treatment of pharyngoesophageal stricture after total laryngopharyngectomy and microvascular free tissue reconstruction: Laryngoscope, 2003; 113(9); 1499-502
30.. Hirshoren N, Eliashar R, Wound-healing modulation in upper airway stenosis-Myths and facts: Head Neck, 2009; 31(1); 111-26
31.. Jones LM, Guillory VL, Mair EA, Total nasopharyngeal stenosis: Treatment with laser excision, nasopharyngeal obturators, and topical mitomycin-C: Otolaryngol Head Neck Surg, 2005; 133(5); 795-98
32.. Perepelitsyn I, Shapshay SM, Endoscopic treatment of laryngeal and tracheal stenosis-has mitomycin C improved the outcome?: Otolaryngol Head Neck Surg, 2004; 131(1); 16-20
33.. Méndez-Nieto CM, Zarate-Mondragón F, Ramírez-Mayans J, Flores-Flores M, Topical mitomycin C versus intralesional triamcinolone in the management of esophageal stricture due to caustic ingestion: Rev Gastroenterol Mex, 2015; 80(4); 248-54
Figures
Tables
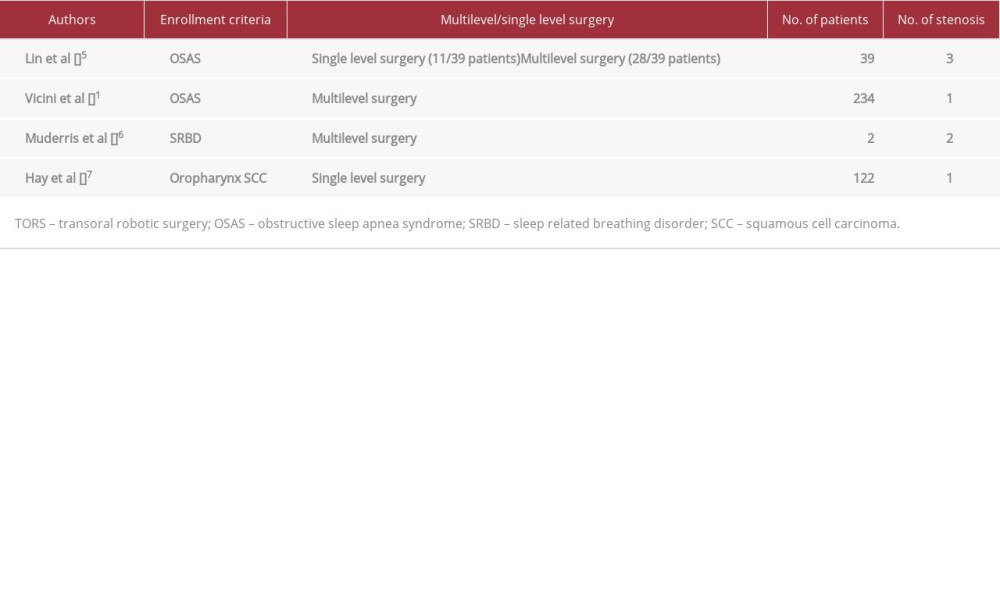 Table 1.. Oropharyngeal stenosis after TORS: review of the literature.
Table 1.. Oropharyngeal stenosis after TORS: review of the literature. Table 2.. Therapeutic options for oropharyngeal stenosis: review of the literature.Table 1.. Oropharyngeal stenosis after TORS: review of the literature.Table 2.. Therapeutic options for oropharyngeal stenosis: review of the literature.
Table 2.. Therapeutic options for oropharyngeal stenosis: review of the literature.Table 1.. Oropharyngeal stenosis after TORS: review of the literature.Table 2.. Therapeutic options for oropharyngeal stenosis: review of the literature. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report  22,760,204
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133