13 September 2022: Articles 
A Challenging Case of Meningitis in a 64-Year-Old Woman Who Presented with Symptoms of Cerebellar Hemorrhage
Mistake in diagnosis, Diagnostic / therapeutic accidents, Management of emergency care, Rare disease, Educational Purpose (only if useful for a systematic review or synthesis)
Akinori Sasaki1ABEF, Masao Horiuchi1AE, Eiji HiraokaDOI: 10.12659/AJCR.937139
Am J Case Rep 2022; 23:e937139






Abstract
BACKGROUND: There is a recognized association between bacterial meningitis and intracranial hemorrhage. However, acute neurological symptoms at presentation, with confirmation of hemorrhage on imaging, may delay further investigations, including blood culture for diagnosing an infection. This report presents a challenging case of Streptococcus pneumoniae meningitis in a 64-year-old woman who presented with symptoms of cerebellar hemorrhage.
CASE REPORT: This report describes a 64-year-old woman who had a medical history of untreated diabetes mellitus. She was brought to our hospital with headache and impaired consciousness, complicated with fever. Based on the hemorrhage in the left cerebellar hemisphere detected in the head CT findings, the patient was initially diagnosed with cerebellar hemorrhage. However, a positive blood culture after 12 hours of admission made the physician consider a central nervous system infection as the cause of the hemorrhage and perform a lumbar puncture. Therefore, the patient was diagnosed with acute bacterial meningitis caused by Streptococcus pneumoniae, and antibiotic treatment was started immediately. Although her general condition improved after antibiotic treatment, her mental status did not improve completely.
CONCLUSIONS: This report highlights that the clinicians should be aware that bacterial meningitis may result in intracranial hemorrhage. Patients with symptoms of a hemorrhagic stroke should be thoroughly investigated to avoid a delay in the treatment of infection.
Keywords: Intracranial Hemorrhage, Hypertensive, Meningitis, Bacterial, Brain Hemorrhage, Traumatic, Streptococcus pneumoniae, Anti-Bacterial Agents, Cerebral Hemorrhage, Female, Humans, Intracranial Hemorrhages, Meningitis, Pneumococcal, Middle Aged
Background
Bacterial meningitis is a life-threatening disease with an incidence of 2 cases per 100 000 adults worldwide [1]. Approximately 400 adults suffer yearly from bacterial meningitis in Japan [2]. The mortality rate of acute untreated bacterial meningitis is 100% [3]. Additionally, despite the availability of effective antibiotics and intensive neurological care, the overall mortality remains high, with 17–34% of survivors displaying persistent unfavorable neurological outcomes [4–6].
The clinical symptoms of bacterial meningitis include fever, nuchal rigidity, and an altered mental status [4]. Bacterial meningitis can also be complicated by cerebrovascular disorders, including ischemic strokes, intracerebral hemorrhage, and cerebral sinus thrombosis, which are major contributing factors to high disability and mortality among patients [7]. Cerebrovascular complications and ischemic strokes are common in patients with bacterial meningitis, occurring in up to 15% and 10% of cases, respectively [7,8]. Although a study reported that only 2.3% of patients display cerebellar hemorrhage as a complication of bacterial meningitis, the prognosis is poor, requires timely diagnosis, and necessitates prompt treatment [7]. A previous study suggested that infectious intracranial aneurysms and intracerebral vasculitis can cause cerebrovascular complications in bacterial meningitis [9]. In addition, several case reports documented complications of intracranial hemorrhage in patients with bacterial meningitis [10–12].
It is crucial to immediately identify the causative bacterial pathogens and initiate appropriate treatment for patients with bacterial meningitis. Previous studies have shown that a delay in starting antimicrobial treatment is associated with an increase in mortality and residual neurologic deficits [13,14]. Herein, this report presents a challenging case of
Case Report
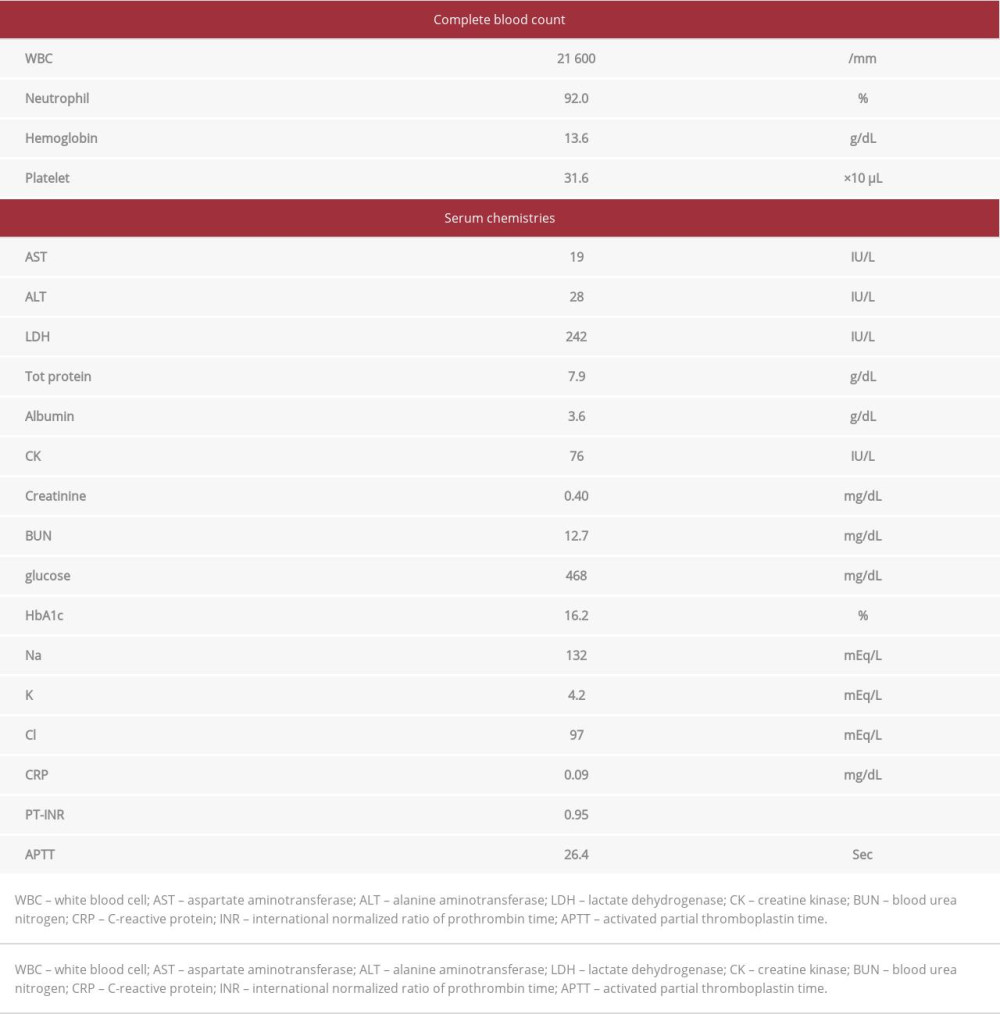
A 64-year-old woman presented with headache 2 days prior to admission. On the day of admission, she was found by family members to have an altered mental status, characterized by incoherent states and newly developed lethargy. The patient was brought to our hospital by ambulance. She had a medical history of untreated diabetes mellitus. On physical examination, she was febrile at 38.6°C, her pulse was 128 beats/minute, and her blood pressure was 180/88 mmHg. She had cognitive impairment, with a Glasgow Coma Scale (GCS) score of 10/15 (E3V2M5). Laboratory findings showed a white blood cell count of 21 600/mm3 (neutrophil, 92%) and a C-reactive protein (CRP) level of 0.09 mg/dL. Serum glucose and hemoglobin A1c levels were elevated to 468 mg/dL and 16.2%, respectively. Liver function, renal function, and serum electrolyte levels were within normal limits (Table 1).
Computed tomography (CT) of the head was performed immediately to examine the cause of the patient’s impaired consciousness. Although physical and neurological findings were examined in the Emergency Department, the progression of the case revealed that this assessment may have been insufficient. Head CT revealed a high-density focus in the left cerebellar hemisphere and fluid collection in the right maxillary paranasal sinus (Figure 1A, 1B). She was diagnosed with cerebellar hemorrhage, which was initially considered the cause of her altered mental status. The patient was admitted to the neurosurgical unit. At this point, bacterial meningitis was not suspected.
She was started on intravenous nicardipine, and the dose was adjusted to maintain systolic blood pressure lower than 140 mmHg. In addition, 2 sets of blood cultures were obtained upon admission to the hospital because the patient was febrile. Both blood cultures grew gram-positive cocci in chains 12 hours after admission. The Department of Internal Medicine was also consulted. On physical examination, the patient’s vital signs were as follows: temperature, 37.8°C; pulse, 102 beats/min, and blood pressure, 142/74 mmHg. The patient’s impaired consciousness continued to worsen (GCS score, 8/15; E2V2M4). A stiff neck was also recognized on clinical examination. The CRP level was elevated to 13.8 mg/dL. She was also noted to have sinusitis on CT on admission (Figure 1B). Considering these findings, we suspected bacterial meningitis and immediately performed a lumbar puncture. Cerebrospinal fluid analysis revealed pleocytosis of 217 cells/mm3 (70% polymorphonuclear), elevated protein level (647 mg/dL), and low glucose level (4 mg/dL). Acute meningitis was strongly suspected to be the underlying cause of her altered mental status, cerebellar hemorrhage, and fever. She was administered 9.9 mg of dexamethasone intravenously 4 times daily, 2 g of ceftriaxone twice daily, and 2 g of vancomycin as a loading dose followed by 1 g twice daily, initiated 12 hours after admission [15].
On day 3 of admission (2 days after initiation of antibiotic treatment), her impaired consciousness persisted; therefore, we decided to perform brain magnetic resonance imaging (MRI). MRI revealed bright sulci with features corresponding to subarachnoid hemorrhage, and no aneurysm was noted on magnetic resonance angiography on day 4 of admission (Figure 2). Septic embolism and infectious endocarditis were suspected to be the cause of the subarachnoid hemorrhage; however, transthoracic echocardiography detected no vegetation or valvular disease.
On day 5, her body temperature normalized.
Discussion
To the best of our knowledge, we present an extremely rare case of acute bacterial meningitis complicated by intracerebral and subarachnoid hemorrhages. This case of bacterial meningitis was complicated by both cerebellar and subarachnoid hemorrhage. In addition, this was a didactic case because her altered mental status was initially attributed only to cerebellar hemorrhage, and the delayed diagnosis of bacterial meningitis might have led to her persistently altered mental status. Thus, the case highlights the need for clinicians to be aware that bacterial meningitis can result in intracranial hemorrhage.
Acute bacterial meningitis is a medical emergency that results in substantial morbidity and mortality despite the availability of effective antibiotic therapy [17]. In particular, pneumococcal meningitis, which is sometimes complicated by neurological (eg, cerebral edema, infarction, intracranial hemorrhage) and systemic (eg, septic shock, acute respiratory distress syndrome, and disseminated intravascular coagulation) complications, is associated with poor prognosis [18]. To improve prognosis, the most important initial issues are timely diagnosis and prompt administration of appropriate antimicrobial therapy. A head CT scan is not always necessary in patients with bacterial meningitis. However, head CT findings should always be taken into consideration before performing a lumbar puncture in patients with suspected bacterial meningitis and an altered mental status [19]. In such cases, blood cultures should be collected immediately, and antibiotic therapy should be started prior to CT.
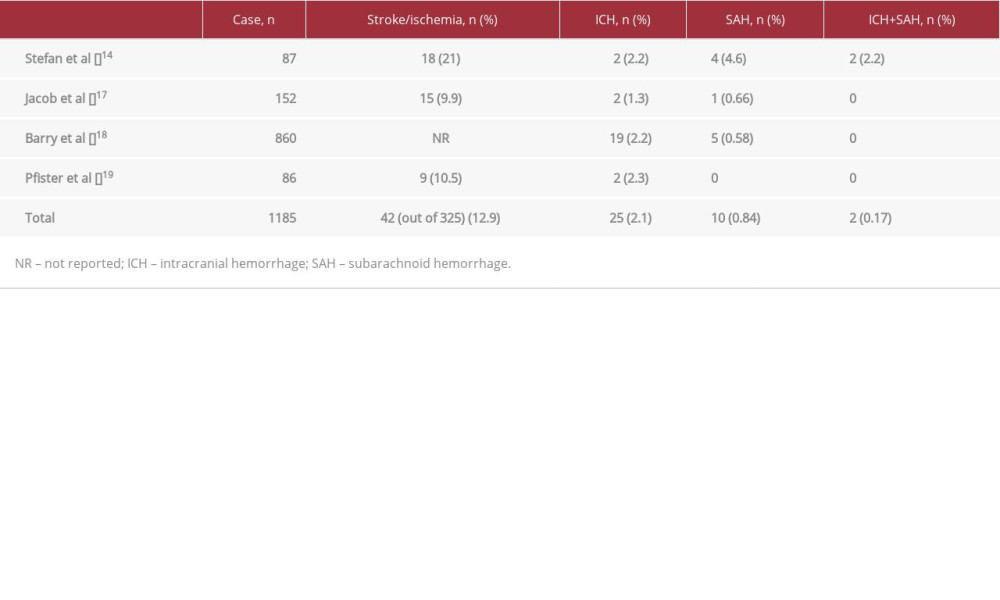
Ischemic stroke is the most common cerebrovascular complication of bacterial meningitis, and subarachnoid and intracranial hemorrhages are very rare [20]. In our extensive literature search, 4 articles investigating the incidence rate of stroke and intracranial hemorrhage related to bacterial meningitis were identified [18,21–23] (Table 2). The review revealed that stroke occurred as a complication in more than 10% of bacterial meningitis cases. Meanwhile, the incidence of both subarachnoid and cerebral hemorrhage as a complication of bacterial meningitis is only 0.2%, as shown in Table 2. Furthermore, cerebellar hemorrhage is a rare complication of bacterial meningitis, and only 1 case has been reported [24]. Because of this rarity, the diagnosis of meningitis can be delayed, as in our case, among patients with intracerebral hemorrhage.
The pathogenetic mechanisms involved in the development of intracerebral hemorrhage likely include a destructive process against the blood vessels and an inflammatory response generated in the subarachnoid space due to the infection. This process may eventually lead to the formation of micro-aneurysms with fatal rupture, resulting in a cerebral hematoma or subarachnoid hemorrhage [25]. Cerebral vasculopathy, including microaneurysms in bacterial meningitis, can occur due to infection by various organisms such as
Stroke, either ischemic or hemorrhagic, associated with bacterial meningitis can occur at an early phase, such as on admission and within 1 week after admission, or at a late phase, such as 1 week or even after successful treatment [8,21,28]. In previous case reports, all the reported cases were complicated with hemorrhagic stroke after the diagnosis of bacterial meningitis [10–12]. On the other hand, when a hemorrhagic stroke is diagnosed on admission, the diagnosis of bacterial meningitis can be delayed, as in our case, through the diagnostic delay mechanism of anchoring and early closure [29]. To prevent this, physicians should be aware that hemorrhagic stroke can be the initial manifestation of bacterial meningitis. Additionally, the emergency physician performed a head CT scan before sufficiently examining the physical findings. If we had taken a more detailed medical history and performed the physical examination more comprehensively, we could have diagnosed and treated the cause immediately. A previous study shows that the incidence of diagnostic delay in emergency departments is higher than in outpatient departments [30]. These diagnostic delays may be caused by insufficient assessment, inappropriate response to diagnostic imaging, and failure to recommend appropriate diagnostic imaging.
In general, patients with cerebellar hemorrhage usually have headaches, nausea, vomiting, vertigo, and ataxia. Unless the hemorrhage is large or complicated by compression of the brainstem, they do not present with an altered level of consciousness [31]. Therefore, when patients are complicated by impaired consciousness despite a small cerebellar hemorrhage without compression of the brainstem, other etiologies should be considered. Additionally, our patient was febrile during the first medical examination. Although fever can occur in cases of ventricular hemorrhage, it usually does not occur in cases of cerebellar hemorrhage [32]. In particular, bacterial meningitis must be considered as a differential diagnosis in patients with cerebellar hemorrhage presenting with altered mental status and fever. In this case, although the patient had a clinical presentation and medical history typical for bacterial meningitis, she was initially misdiagnosed because cerebellar hemorrhage was discovered on head CT examination.
Conclusions
This report highlights that clinicians should be aware that bacterial meningitis can result in intracranial hemorrhage. Patients with symptoms of a hemorrhagic stroke should be thoroughly investigated to avoid a delay in the treatment of infection.
Figures
References:
1.. van de Beek D, de Gans J, Tunkel AR, Wijdicks EFM, Community-acquired bacterial meningitis in adults: N Engl J Med, 2006; 354; 44-53
2.. Kamei S, Takasu T, Nationwide survey of the annual prevalence of viral and other neurological infections in Japanese inpatients: Intern Med, 2000; 39; 894-900
3.. Swartz MN, Bacterial meningitis – a view of the past 90 years: N Engl J Med, 2004; 351; 1826-28
4.. van de Beek D, de Gans J, Spanjaard L, Clinical features and prognostic factors in adults with bacterial meningitis: N Engl J Med, 2004; 351; 1849-59
5.. Flores-Cordero JM, Amaya-Villar R, Rincón-Ferrari MD, Acute community-acquired bacterial meningitis in adults admitted to the Intensive Care Unit: Clinical manifestations, management and prognostic factors: Intensive Care Med, 2003; 29; 1967-73
6.. Thigpen MC, Whitney CG, Messonnier NE, Bacterial meningitis in the United States, 1998–2007: N Engl J Med, 2011; 364; 2016-25
7.. Pfister HW, Borasio GD, Dirnagl U, Cerebrovascular complications of bacterial meningitis in adults: Neurology, 1992; 42; 1497-504
8.. Katchanov J, Heuschmann PU, Endres M, Weber JR, Cerebral infarction in bacterial meningitis: Predictive factors and outcome: J Neurol, 2010; 257; 716-20
9.. Deliran SS, Brouwer MC, van de Beek D, Subarachnoid hemorrhage in bacterial meningitis patients: Cerebrovasc Dis, 2022; 51; 118-24
10.. Matsumoto A, Mino S, Nishiyama T, Intracranial hemorrhage caused by bacterial meningitis: Case report and review of the literature: Asian J Neurosurg, 2019; 14; 234-36
11.. Siddiqui B, Chevenon M, Nandi M, The first documented case of hemorrhagic stroke caused by group B streptococcal meningitis: IDCases, 2015; 2; 118-19
12.. Zou H, Pan KH, Pan HY, Cerebral hemorrhage due to tuberculosis meningitis: A rare case report and literature review: Oncotarget, 2015; 6; 45005-9
13.. Aronin SI, Peduzzi P, Quagliarello VJ, Community-acquired bacterial meningitis: Risk stratification for adverse clinical outcome and effect of antibiotic timing: Ann Intern Med, 1998; 129; 862-69
14.. Bodilsen J, Dalager-Pedersen M, Schønheyder HC, Nielsen H, Time to antibiotic therapy and outcome in bacterial meningitis: A Danish population-based cohort study: BMC Infect Dis, 2016; 16; 392
15.. Tunkel AR, Hartman BJ, Kaplan SL, Practice guidelines for the management of bacterial meningitis: Clin Infect Dis, 2004; 39; 1267-84
16.. Tan TQ, Schutze GE, Mason EO, Kaplan SL: Antimicrob Agents Chemother, 1994; 38; 918-23
17.. Hussein AS, Shafran SD, Acute bacterial meningitis in adults. A 12-year review: Medicine (Baltimore), 2000; 79; 360-68
18.. Kastenbauer S, Pfister HW, Pneumococcal meningitis in adults: Spectrum of complications and prognostic factors in a series of 87 cases: Brain, 2003; 126; 1015-25
19.. Hasbun R, Abrahams J, Jekel J, Quagliarello VJ, Computed tomography of the head before lumbar puncture in adults with suspected meningitis: N Engl J Med, 2001; 345; 1727-33
20.. Swartz MN, Bacterial meningitis: More involved than just the meninges: N Engl J Med, 1984; 311; 912-14
21.. Bodilsen J, Dalager-Pedersen M, Schønheyder HC, Nielsen H, Stroke in community-acquired bacterial meningitis: A Danish population-based study: Int J Infect Dis, 2014; 20; 18-22
22.. Mook-Kanamori BB, Fritz D, Brouwer MC, van der Ende A, van de Beek D, Intracerebral hemorrhages in adults with community associated bacterial meningitis in adults: Should we reconsider anticoagulant therapy?: PLoS One, 2012; 7; e45271
23.. Pfister HW, Feiden W, Einhäupl KM, Spectrum of complications during bacterial meningitis in adults. Results of a prospective clinical study: Arch Neurol, 1993; 50; 575-81
24.. de Souza AL, Sztajnbok J, Seguro AC, Cerebellar hemorrhage as an atypical complication of meningococcal meningitis: Int J Infect Dis, 2008; 12; 558-59
25.. Gironell A, Domingo P, Mancebo J, Hemorrhagic stroke as a complication of bacterial meningitis in adults: Report of three cases and review: Clin Infect Dis, 1995; 21; 1488-91
26.. Magnus J, Parizel PM, Ceulemans B: J Child Neurol, 2011; 26; 1438-43
27.. Sáez-Llorens X, McCracken GH, Bacterial meningitis in children: Lancet, 2003; 361; 2139-48
28.. Kato Y, Takeda H, Dembo T, Tanahashi N, Delayed recurrent ischemic stroke after initial good recovery from pneumococcal meningitis: Intern Med, 2012; 51; 647-50
29.. Nendaz M, Perrier A, Diagnostic errors and flaws in clinical reasoning: Mechanisms and prevention in practice: Swiss Med Wkly, 2012; 142; w13706
30.. Hussain F, Cooper A, Carson-Stevens A, Diagnostic error in the Emergency Department: Learning from national patient safety incident report analysis: BMC Emerg Med, 2019; 19; 77
31.. Datar S, Rabinstein AA, Cerebellar hemorrhage: Neurol Clin, 2014; 32(4); 993-1007
32.. Schwarz S, Häfner K, Aschoff A, Schwab S, Incidence and prognostic significance of fever following intracerebral hemorrhage: Neurology, 2000; 54; 354-61
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133