29 September 2022: Articles 
SARS-CoV-2 Causing Transient Central Sleep Apnea in Patients Treated for Obstructive Sleep Apnea with Continuous Positive Airway Pressure
Unusual clinical course, Rare coexistence of disease or pathology
Rupendra Ghatak1ABCDEF*, Vishal Saini2ABCDEDOI: 10.12659/AJCR.937427
Am J Case Rep 2022; 23:e937427






Abstract
BACKGROUND: SARS-CoV-2 has globally affected humanity and devastated many families. Here, we attempt to identify which diseases are independent risk factors for severe SARS-CoV-2. There have been multiple studies that have evaluated the impact of obstructive sleep apnea (OSA) on SARS-CoV-2 outcomes, suggesting that OSA is an independent risk factor. SARS-CoV-2 has also been suggested to invade the central nervous system and be responsible for neurological signs and decreasing central respiratory drive. Central sleep apnea (CSA) is defined when apneas and hypopneas are associated with absent or reduced ventilatory effort, respectively, due to diminished central respiratory drive.
CASE REPORT: Here, we describe 2 cases involving patients with OSA that developed transient central sleep apnea after being diagnosed with SARS-CoV-2 by polymerase chain reaction. They had similar past medical histories and presentation of illness. The differences included compliance of continuous positive airway pressure (CPAP), recovery, and severity of central sleep index. We review and address alternate causes for the development of CSA. We hypothesize that continuous and compliant use of CPAP machines may be beneficial in reducing recovery and severity of SARS-CoV-2.
CONCLUSIONS: Our case report calls attention to the acquired central respiratory drive neurological complication associated with SARS-CoV-2. Our case report highlights the plausible existence of a relationship between development of central respiratory drive leading to CSA and SARS-CoV-2 infection. Further studies are needed to explore this relationship, including evaluating whether CSA occurs in SARS-CoV-2 patients with no history of OSA.
Keywords: COVID-19, Sleep Apnea Syndromes, sleep apnea, central, COVID-19, Continuous Positive Airway Pressure, Humans, SARS-CoV-2, Sleep apnea, obstructive
Background
SARS-CoV-2 has globally affected humanity and devastated many families. Here, we attempt to identify which diseases are independent risk factors for severe SARS-CoV-2. There have been multiple studies that evaluated the impact of obstructive sleep apnea (OSA) on SARS-CoV-2 outcomes, with implications that OSA is an independent risk factor [1]. SARSCoV-2 has also been suggested to invade the central nervous system and be responsible for neurological signs and decreasing central respiratory drive [2]. Central sleep apnea (CSA) is defined when apneas and hypopneas are associated with absent or reduced ventilatory effort, respectively, due to diminished central respiratory drive [3]. Here, we describe 2 cases involving patients with OSA that developed transient central sleep apnea after being diagnosed with SARS-CoV-2 by polymerase chain reaction. They had similar past medical histories and presentation of illness. The differences included compliance of continuous positive airway pressure (CPAP), recovery, and severity of central sleep index. We hypothesize that continuous and compliant use of CPAP machines may be beneficial in reducing recovery and severity of SARS-CoV-2.
Case Reports
PATIENT #1:
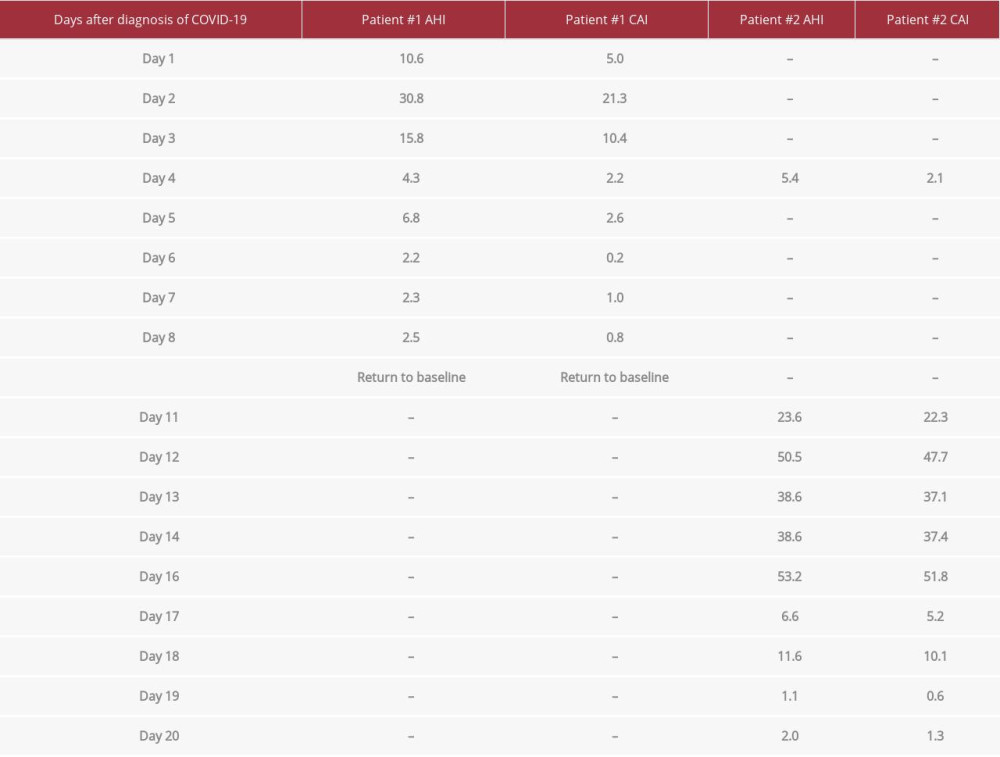
A 41-year-old woman with a past medical history of generalized anxiety disorder, post-traumatic stress disorder, hypothyroidism, and high body mass index (BMI) presented to an outpatient sleep diagnostic lab for evaluation of OSA. She was referred to the lab by her primary care physician, who did not note any recent mood or medication changes. Her concerns included loud snoring, difficulty with supine sleep, nocturnal gasping/choking episodes, daytime naps (non-refreshing), poor concentration, increased irritability, morning headache, sleep fragmentation, spousal disturbance, restless sleep, sleep talking, bruxism, and nocturia. Her Epworth Sleepiness score was 15/24. After evaluation, she was scheduled for a sleep study. Review of the sleep study demonstrated an initial apnea-hypopnea index (AHI) of 9.4 with lowest oxygen saturation of 88%. Treatment with a CPAP machine was ordered. Subsequent follow-up visits showed the patient remained compliant with the machine and remote downloads of the CPAP device demonstrated an average AHI of 1.1 to 2.1/h with CSA 0.1 to 0.6/h.
During the SARS-CoV-2 pandemic, she presented 2 months later with a chief concern of chest congestion, worsening morning headaches, nasal congestion, fatigue, and subjective fevers. She tested positive for SARS-CoV-2 by polymerase chain reaction (PCR) test. We continued to monitor the patient’s remote CPAP downloads (ResMed AirSense 10), which demonstrated significant changes in AHI and development of transient CSA. The downloads did not show any changes in Cheyne-Stokes respirations. Raw waveforms during the central sleep apnea episodes were unfortunately not reported in the download. Of note, prior to diagnosis with SARS-CoV-2 and after resolution of symptoms, the patient’s AHI and CSA episodes returned to baseline. See Table 1.
PATIENT #2:
A 34-year-old man with a past medical history of obstructive sleep apnea, excessive daytime sleepiness, moderate-severe insomnia, high body mass index, gastroesophageal reflux disease, and non-compliance with CPAP therapy presented to an outpatient sleep diagnostic lab with a chief concern of fatigue. He was initially referred to the lab by his primary care physician 2 years prior. He did not note any recent mood or medications changes. He presented during the SARS-CoV-2 pandemic for a routine follow-up. He had concerns of a productive cough, subjective fevers, and shortness of breath. His primary care physician ordered a SARS-CoV-2 by PCR and was confirmed positive. As with patient number 1, we continued to monitor the patient’s remote CPAP downloads (ResMed AirSense 10), which demonstrated significant changes in AHI and development of transient CSA. The downloads did not show any changes in Cheyne-Stokes respirations. Raw waveforms during the central sleep apnea episodes were not reported in the download. Eventually, the patient’s AHI and CSA episodes eventually returned to baseline. Prior to the diagnosis with SARS-CoV-2 and after delayed resolution of symptoms, the patient’s AHI and CSA episodes eventually returned to baseline (Table 1).
Discussion
A literature review revealed no case reports, manuscripts, or trials explaining the relationship between SARS-CoV-2 and central sleep apnea. Our 2 case reports suggest that there is a link between SARS-COV-2 infection and some insult to the central nervous system causing central sleep apnea episodes. Some authors theorize that, in patients with SARS-CoV-2 and obstructive sleep apnea, a pro-inflammatory state is created that diminishes systemic blood vessel endothelium, including the brain. The mechanism of action for this injury is thought to be from oxidative stress, metabolic changes, and a pro-inflammatory phenotype that likely led to endothelial dysfunction and injury [4].
The presentation of the 2 case reports had similarities and differences both in past medical history and course of disease. Both patients had similar concerns, tested positive for SARSCoV-2 by PCR, and had underlying mood disorders without any recent changes in medications. In patient number 1, the mood symptoms worsened during the disease, including poorer concentration and increased irritability. There were no medication changes to her anxiolytic/antidepressant during the infection. Her mood symptoms gradually improved after the disease state resolved. In patient number 2, there was no exacerbation of mood symptoms. We hypothesize there could be a correlation between mood, metabolism, or medication changes causing central sleep apnea episodes. Our case presentations suggest the link is more consistent with SARS-CoV-2 causing an increase in central apnea index (CAI).
It is unclear if the CSA episodes were a result of increased central respiratory drive from SARS-CoV-2. Other important causes of CSA include hypoxia or severe hypoventilation [5]. AHI levels reaching 30-50 suggest a periodic breathing pattern. The high number of CSA events and almost all events were central. We suggest that this is a true finding of CSA and is less likely to be a suppression of controller gain (change in ventilation induced by a change in PaCO2 level), chemoreceptor responsiveness, chemoreceptor sensitivity, plant gain (ability of lungs and respiratory muscles to increase ventilation), or mixing gain, which could be affected by infections through hypoxia, hypoventilation, fluid in the lung, change in lung compliance, or increase in arousals. Neither of our patients had cardiac, pulmonary, or neurologic diseases besides OSA or other findings to suggest these mechanisms of action.
Treatment emergent-sleep apnea (TECSA, formerly complex sleep apnea) describes the appearance of central sleep apnea and/or hypopnea while undergoing treatment for obstructive sleep apnea [6]. Common risk factors of TECSA include cardiac conditions such as coronary artery disease, hypertension, congestive heart failure, atrial fibrillation, and stroke [7]. Ventilatory controller instability as described in the previous paragraph, when severe OSA patients showed a high “loop gain”, was not present in our 2 patients. We recognized TESCA and determined that this sleep-breathing disorder was not associated with risk factors, epidemiological prevalence, or clinical characteristics of our patients. Central sleep apnea was not observed on previous CPAP download data and the patients had predominant OSA at baseline.
Central apneas are defined by the device and algorithms. The algorithms respond to flow changes and could have increased the pressure in response to the SARS-CoV-2 infection inducing more centrals [8]. We are not aware of any wakefulness or coughing that could have caused an artifact that could have been recorded as an open airway apnea [9]. We recognize that positional AHI is a potential factor, but are unable to report on this as it was not recorded during patient interviews. Transient increases in CSA can occur in people traveling to high altitude locations [10]. We did not record if they had any recent travel, this was unlikely to be the cause of the transient CSA. We elected to not include download reports weeks prior and after the SARS-CoV-2 infection because they were similar at baseline AHI and CAI.
We postulate that in patient number 2, CSA episodes developed early in the disease state but were unable to be detected due to non-compliance with the machine. The question remains why did patient number 1 improve and patient number 2 symptomatically took longer to recover and had a worse CAI. We know SARS-CoV-2 is not fully understood. It has differences in presentation and severity. We reviewed and compared both patients. The major difference between the 2 patients was non-compliance. We hypothesize that continuous and compliant use of CPAP may be beneficial in reducing recovery and severity of SARS-CoV-2, especially in patients who develop CSA episodes during a SARS-CoV-2 infection.
We do know that obstructive sleep apnea and SARS-CoV-2 share a similar at-risk clinical presentation of developing extrapulmonary manifestations, including neurological complications [2]. It remains to be seen if SARS-CoV-2 can directly result in the permanent development of CSA. These 2 cases showcase a transient development of central sleep apnea with a return to baseline. In both cases the average AHI of the patient remained slightly elevated after resolution, signifying the patient’s respiratory drive has sustained an unknown assault to either the neurological or respiratory system.
Conclusions
Our case report calls attention to the acquired central respiratory drive neurological complication associated with SARSCoV-2. We hypothesize that continuous and compliant use of CPAP may be beneficial in reducing recovery time and severity of SARS-CoV-2. Our case report highlights the plausible existence of a relationship between development of central respiratory drive leading to CSA and SARS-CoV-2 infection. Further studies are needed to explore this relationship, including evaluating if CSA occurs in SARS-CoV-2 patients with no history of OSA.
References:
1.. Sahni A, Cao M, Obstructive sleep apnea and severe COVID19 infection: Is there a plausible link?: J Clin Sleep Med, 2021; 17(11); 2145-46
2.. Ramasubban S, Goswami L, Banerjee N, Central sleep apnea in a patient with dengue encephalitis: Apollo Med, 2015; 12; 46-49
3.. : International classification of sleep disorders, 2014, Darien, IL, American Academy of Sleep Medicine
4.. Breville G, Adler D, Uginet M, Does endothelial vulnerability in OSA syndrome promote COVID-19 Encephalopathy?: Chest, 2021; 160(2); e161-64
5.. Sowho M, Amatoury J, Kirkness JP, Patil SP, Sleep and respiratory physiology in adults: Clin Chest Med, 2014; 35(3); 469-81
6.. : American Academy of Sleep Medicine, 2014, Darien, IL, USA
7.. Zhang J, Wang Guo HJ, Treatment-emergent central sleep apnea: A unique sleep-disordered breathing: Chin Med J (Engl), 2020; 133(22); 2721-30
8.. Johnson KG, Johnson DC, Bilevel positive airway pressure worsens central apneas during sleep: Chest, 2005; 128(4); 2141-50
9.. Johnson KG, Johnson DC, Treatment of sleep-disordered breathing with positive airway pressure devices: Technology update: Med Devices (Auckl), 2015; 8; 425-37
10.. Ginosar Y, Malhotra A, Schwartz E, High altitude, continuous positive airway pressure, and obstructive sleep apnea: Subjective observations and objective data: High Alt Med Biol, 2013; 14(2); 186-89
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133