25 November 2022: Articles 
Two Pediatric Patients with Splanchnic Venous Thrombosis as a Complication of Acute Pancreatitis Successfully Treated with Low-Molecular-Weight Heparin and Rivaroxaban
Unusual clinical course, Unusual or unexpected effect of treatment
Shannon Capraro1ABEF, Melissa Acquazzino2BDE, Mary Drake3DE, Chinenye R. Dike45ABDEF*DOI: 10.12659/AJCR.937599
Am J Case Rep 2022; 23:e937599






Abstract
BACKGROUND: Two Pediatric Patients with Splanchnic Venous Thrombosis as a Complication of Acute Pancreatitis Successfully Treated with Low-Molecular-Weight Heparin and Rivaroxaban
CASE REPORT: Case 1: A 13-year-old girl presented with a second attack of acute pancreatitis. She developed a non-occlusive splenic vein thrombosis diagnosed by CT scan on the sixth day of hospitalization. Injectable low-molecular-weight heparin was started during hospitalization and switched to oral rivaroxaban at discharge. Imaging at follow-up showed resolution of thrombosis. Case 2: A 9-year-old girl with history of acute recurrent pancreatitis presented with a third attack of acute pancreatitis. An occlusive splenic vein thrombosis with extension into the portal vein and superior mesenteric vein and necrotizing pancreatitis was seen on CT scan on the third day of hospitalization. Low-molecular-weight heparin was initiated during hospitalization and was switched to oral rivaroxaban at discharge. Imaging at follow-up demonstrated nearly complete resolution of the extensive thrombosis.
CONCLUSIONS: Splanchnic venous thrombosis remains a rare complication of pediatric pancreatitis. Anticoagulant use in patients with these complications remains controversial. Direct oral anticoagulants are as safe and effective as low-molecular-weight heparin and should be considered for use in children instead of low-molecular-weight heparin due to its advantages, including the availability of enteral forms of administration.
Keywords: Anticoagulants, Pancreatitis, Pediatrics, Venous Thrombosis, Female, Humans, Child, Adolescent, Splenic Vein, Rivaroxaban, Acute Disease, Thrombosis, Heparin, Low-Molecular-Weight
Background
Acute pancreatitis (AP) and its complications have become increasingly recognized in children in the past decade due to improved physician awareness [1]. Splanchnic venous thrombosis is one of the known complications of AP and usually involves the splenic vein [2]. Other vessels, including the portal vein and superior mesenteric vein, can also be affected, either in isolation or in addition to splenic vein thrombosis [2]. A meta-analysis demonstrated a 14.1% incidence rate of pancreatitis-associated splanchnic vein thrombosis in hospitalized adult patients with pancreatitis. In that review, the rate of pancreatitis-associated splanchnic vein thrombosis was 22.6% in patients with AP and 12.4% in patients with chronic pancreatitis (CP) [3]. Pancreatitis-associated splanchnic vein thrombosis is regarded as a local manifestation of the peripancreatic inflammation that occurs with pancreatitis [4].
Pancreatitis-associated splanchnic vein thrombosis is most reported in AP, especially severe AP with necrosis and peripancreatic collections [5]. In a single-center case series of 72 pediatric patients, 15.4% of patients with AP developed splanchnic venous thrombosis, compared to 0% of CP patients [6]. Additionally, in the largest multicenter cohort for pediatric acute recurrent pancreatitis (ARP) and CP (International Study Group of Pediatric Pancreatitis: In Search for a CuRE), out of 410 children in the cohort, vascular complications were mostly reported in moderately severe or severe AP but only reported in 1.2% of the cohort [7]. The benefit of anticoagulant use to prevent or treat pancreatitis-associated splanchnic vein thrombosis is yet to be validated in the literature [2,8]. The best type of anticoagulant to use is also not known. While there are multiple reports and observational studies on anticoagulant use for splanchnic thrombosis associated with acute pancreatitis in adults [2,5,8], pediatric data are limited to a few case reports and case series [6,7,9]. Venous thrombosis in children was traditionally treated with LMWH until a recent FDA approval of use of oral anticoagulants in children following a large clinical trial [10]. That large pediatric clinical trial randomized children into direct oral anticoagulant (rivaroxaban) and standard anticoagulant after at least a 5-day course of heparin and revealed that rivaroxaban was effective without any increased adverse effects (such as bleeding) when compared to standard therapy [10]. In that study, all causes of venous thrombotic events were included, particularly catheter-related thrombosis [10]. It is not clear if any child in the cohort had pancreatitis-associated thrombosis. The use of anticoagulants in pancreatitis-associated splanchnic venous thrombosis remains controversial [2,8]. There are gaps in the literature on the need for and benefit of rivaroxaban in pancreatitis-associated splanchnic venous thrombosis in children. Here, we report the cases of 2 children who developed splenic vein thrombosis during episodes of acute pancreatitis. Initially, low-molecular-weight heparin (LMWH) was used for anticoagulation, and this was transitioned to a direct oral anticoagulant (DOAC) at discharge. Thrombosis resolved on follow-up imaging, without any reported complications.
Case Reports
CASE 1:
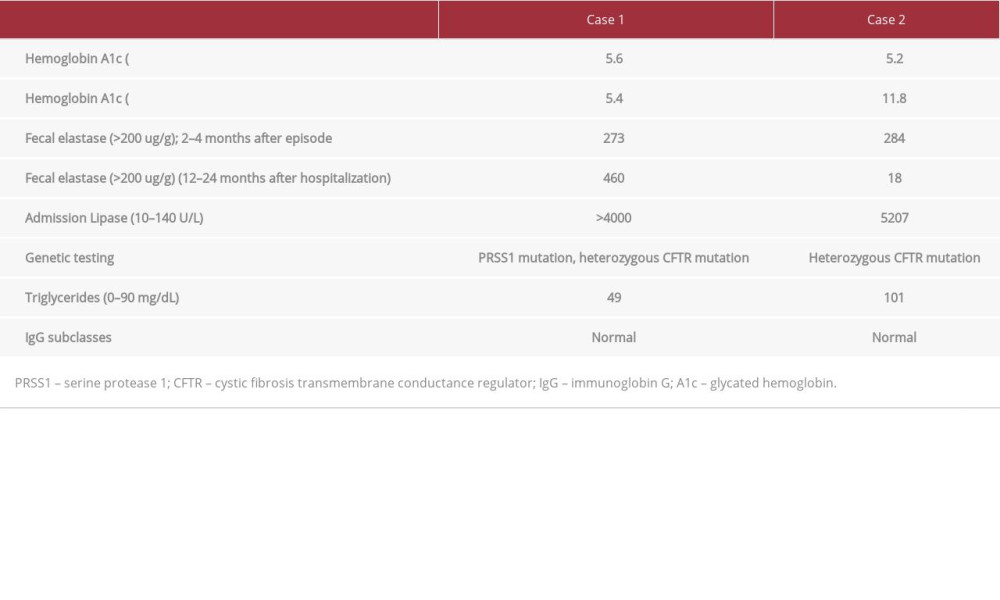
A 13-year-old girl was transferred from a peripheral hospital for her second attack of AP. She also had PRSS1 mutation and obesity (BMI at 99th percentile and Z-score 2.29). She had a family history of pancreatitis in a paternal relative. Diagnosis was made by symptoms of epigastric pain, nausea, and emesis, lipase level of >4000 (at least 28 x ULN) (Table 1), and CT scan results of acute pancreatitis with peripancreatic fat infiltration, without any evidence of thrombosis. She required intravenous fluids and pain control with both non-opioid and opioid analgesics. She was started on prophylactic LMWH (40 mg enoxaparin once daily) upon admission per institution protocol as she was considered high risk for developing venous thrombosis because of the following risk factors: obesity, im-mobility, age/gender (teenage female), and pancreatitis. Given significant nausea, decreased oral intake, and intolerance of intragastric feeds, post-pyloric feeds were initiated on day 5 of admission. Despite this, she continued to worsen, and a repeat CT scan completed on day 6 of hospitalization revealed persistent peripancreatic fat infiltration consistent with pancreatitis with development of a non-occlusive splenic vein thrombosis (Figure 1A) and bilateral pleural effusions without any other complications. Given the development of splenic vein thrombosis while on anticoagulants, the dose of LMWH was increased to treatment dose per recommendations of the hematology team (1 mg/kg every 12 h), and the patient reached target anti-Xa levels within 4 days of initiating the treatment dose. She was switched to oral rivaroxaban (15 mg twice daily for 21 days and then 20 mg daily to complete a 3-month course) at discharge, which was after 10 days of initiating LMWH. She completed a 3-month course of rivaroxaban without any bleeding complications. She was not on any oral contraceptives. Although the splenic vein thrombus was non-occlusive, treatment with anticoagulant was continued for a 3 months per hematology recommendations given development of thrombosis despite prophylactic anticoagulant use. Splenic vein thrombosis had resolved on repeat imaging MRCP at 3 months after discharge (Figure 1B). This imaging, which was also done to evaluate for anatomic anomalies as a possible etiology of ARP, also showed pancreas divisum. Further work-up following that hospitalization was remarkable for PRSS1 and CFTR mutations, with a negative sweat chloride test. She has remained endocrine- and exocrine pancreatic-sufficient.
CASE 2:
A 9-year-old girl with significant history of ARP was transferred from a peripheral hospital for her third attack of AP. She also had a history of obesity (BMI 99th percentile and Z-score 2.27). Remarkable findings at presentation included worsening epi-gastric pain, lipase level of 5207 (Table 1), elevated transaminases, and ultrasound with signs of acute pancreatitis but without gallstones. She required treatment with intravenous fluids, non-opioid analgesics, and opioid analgesics for pain management. She tolerated a clear liquid diet from admission, which was advanced to a regular diet over time. A CT scan was obtained on day 3 of hospitalization given worsening clinical course and fevers. The CT revealed an occlusive splenic vein thrombosis with extension into the portal vein and superior mesenteric vein (Figure 2A), necrotizing pancreatitis, pelvic as-cites, and left pleural effusion with bilateral atelectasis. Given the development of splenic vein thrombosis with portal and superior mesenteric vein thrombosis, a treatment dose LMWH (1 mg/kg every 12 h subcutaneous) was initiated and target anti-Xa levels were achieved. Needle phobia was a major problem for her during hospitalization, during which she cried for several minutes before and after administration of LMWH, resulting in a switch to oral rivaroxaban at hospital discharge, which was 5 days from initiation of LMWH. Imaging (CT scan) done at 3 months after her hospitalization showed that the splenic thrombus had almost completely resolved (Figure 2B). She was not on any contraceptives. She underwent a workup for clotting disorders given a family history of recurrent miscarriages in her mother and early stroke in the maternal grandmother. A workup for thrombosis was done, including Protein C and S activity, Factor V Leiden mutation, Prothrombin 20210 mutation, Lupus anticoagulant, anticardiolipin antibodies, beta-glycoprotein antibodies, factor VIII activity, antithrombin, and homocysteine and these were all negative. She completed a 3-month course of anticoagulation with rivaroxaban, with minor epistaxis resolving without any intervention. She did not have any major bleeding complications. Her pancreatic disease course was complicated by both exocrine and endocrine insufficiency (DM) within 1–2 years following this attack. A workup for a potential cause of chronic pancreatitis, including genetic testing, MRCP, IgG4, celiac panel, and fasting lipid panel, was mostly unremarkable, except for a slightly elevated triglyceride and non-pathogenic heterozygous CFTR mutations (Table 1).
Discussion
We report 2 cases of children with pancreatitis-associated splenic vein thrombosis occurring during moderately severe to severe AP attacks that were successfully managed with oral anticoagulants. Splanchnic vein thrombosis is a known but unusual complication of pancreatitis in children, with a reported incidence of only 1.2% in the INSPPIRE cohort [7]. The splenic vein is the most common vein involved. Other possible complications of acute pancreatitis include pancreatic fluid collections, pancreatic necrosis, extra pancreatic organ dysfunction, and peptic ulcer disease and others [11,12].
The use of anticoagulants in pancreatitis-associated splanchnic venous thrombosis remains controversial in practice, and evidence-based guidelines are lacking. Some authors argue that these thromboses occur as part of the inflammatory process during an episode of pancreatitis, and the thromboses will spontaneously recanalize when the acute inflammation has resolved. They report similar recanalization rates in their patients who had pancreatitis-associated splanchnic venous thrombosis treated with anticoagulants and those who did not have anticoagulant intervention [2,4,5,7,13]. Additionally, a recent meta-analysis concluded that there is no evidence to encourage routine use of anticoagulants in patients with splanchnic venous thrombosis associated with pancreatitis and that prospective studies are needed [13]. Traditionally, LMWH was used to treat thrombosis in children until recent FDA approval for use of oral anticoagulant in this age group following a large multicenter international clinical trial [10]. Both pediatric and adult studies have shown DOAC to be as efficacious as LMWH in resolving thromboses [10,14–16]. The advantages of direct oral anticoagulants over LMWH in children include the ability of precise body weight dosing in an oral form (tablet or suspension) without need to monitor blood levels. DOAC use, as with other anticoagulants, has been associated with an increased risk of bleeding, especially in patients taking concomitant antiplatelet or NSAID medications. In contrast to LMWH, DOACs may not have a readily available reversal agent, which may be a factor limiting their use in children. Furthermore, use of DOACs has been shown to significantly increase the risk of bleeding in patients undergoing endoscopic retrograde cholangiopancreatography (ERCP) [17].
Acute gastrointestinal (GI) bleeding can complicate the course of pancreatitis and this risk can be further increased with use of anticoagulants in pancreatitis-associated thrombosis. Although some authors report no risk of complications or bleeding with anticoagulant use in their cohorts [5, 18], there is a report of 1 case of significant GI bleeding associated with anticoagulant use for portal venous thrombosis resulting from pancreatitis [19]. Both children in our case series received anticoagulants and only 1 had some epistaxis, which did not require intervention. There were no major bleeding complications seen in either case.
A recent study showed that early systemic anticoagulant use can prevent splanchnic venous thromboses associated with pancreatitis without increased risk of bleeding [20], but the authors concluded that this finding needs to be validated by prospective studies. Interestingly, 1 of our patients developed thrombosis even while on enoxaparin prophylaxis.
Needle phobia has been known for decades and is estimated to occur in at least 10% of the population [21]. A systematic review estimated that up to 50% of adolescents have needle phobia [22], and it has been shown to affect rates of vaccination and compliance to therapy in those undergoing treatment.
Needle phobia is therefore another reason to consider DOAC therapy in children with pancreatitis-associated splanchnic venous thrombosis in whom anticoagulant therapy is being considered. Our second patient exhibited extreme needle phobia while receiving LMWH in the hospital, leading her mother to request a switch to an oral anticoagulant agent. Both children, but especially the second child, were happy with the switch from LMWH (injection) to a DOAC (oral).
In summary, we report 2 pediatric cases with pancreatitis-associated splenic vein thrombosis treated successfully with DOAC after achieving therapeutic anti-Xa levels with LMWH, without any major bleeding complications.
Conclusions
The treatment of pancreatitis-associated thrombosis in children with anticoagulants remains controversial. If anticoagulation is considered, DOAC should be preferred given its advantages over LMWH in children, including precise body weight dosing in an oral form (tablet or suspension) over the parenteral forms of LMWH, without need to monitor blood levels.
Figures
References:
1.. Morinville VD, Barmada MM, Lowe ME, Increasing incidence of acute pancreatitis at an American pediatric tertiary care center: Is greater awareness among physicians responsible?: Pancreas, 2010; 39(10); 5-8
2.. Easler J, Muddana V, Furlan A, Portosplenomesenteric venous thrombosis in patients with acute pancreatitis is associated with pancreatic necrosis and usually has a benign course: Clin Gastroenterol Hepatol, 2014; 12(5); 854-62
3.. Butler JR, Eckert GJ, Zyromski NJ, Natural history of pancreatitis-induced splenic vein thrombosis: A systematic review and meta-analysis of its incidence and rate of gastrointestinal bleeding: HPB (Oxford), 2011; 13(12); 839-45
4.. Nadkarni NA, Khanna S, Vege SS, Splanchnic venous thrombosis and pancreatitis: Pancreas, 2013; 42(6); 924-31
5.. Gonzelez HJ, Sahay SJ, Samadi B, Splanchnic vein thrombosis in severe acute pancreatitis: A 2-year, single-institution experience: HPB (Oxford), 2011; 13(12); 860-64
6.. Fayyaz Z, Cheema HA, Suleman H, Clinical presentation, aetiology and complications of pancreatitis in children: J Ayub Med Coll Abbottabad, 2015; 27(3); 628-32
7.. Dike CR, Cress G, Fishman DS, Vascular complications in pediatric pancreatitis: A case series: J Pediatr Gastroenterol Nutr, 2021; 73(4); e94-e97
8.. Norton W, Lazaraviciute G, Ramsay G, Current practice of anticoagulant in the treatment of splanchnic vein thrombosis secondary to acute pancreatitis: Hepatobiliary Pancreat Dis Int, 2020; 19(2); 116-21
9.. Figueroa-Sánchez M, Nuño- Guzmán CM, Álvarez-López MC, Case report: Splanchnic vein thrombosis as a complication of necrotizing acute pancreatitis in a pediatric patient: Front Surg, 2022; 9; 747671
10.. Male C, Lensing AW, Palumbo JS, Rivaroxaban compared with standard anticoagulants for the treatment of acute venous thromboembolism in children: A randomised, controlled, phase 3 trial: Lancet Haematol, 2020; 7(1); e18-e27
11.. Lee KM, Paik CN, Chung WC, Yang JM, Association between acute pancreatitis and peptic ulcer disease: World J Gastroenterol, 2011; 17(8); 1058-62
12.. Tyberg A, Karia K, Gabr M, Management of pancreatic fluid collections: A comprehensive review of the literature: World J Gastroenterol, 2016; 22(7); 2256-70
13.. Hajibandeh S, Hajibandeh S, Agrawal S, Anticoagulation versus no anticoagulation for splanchnic venous thrombosis secondary to acute pancreatitis: Do we really need to treat the incidental findings?: Pancreas, 2020; 49(9); e84-e85
14.. Burnett AE, Mahan CE, Vazquez SR, Guidance for the practical management of the direct oral anticoagulants (DOACs) in VTE treatment: J Thromb Thrombolysis, 2016; 41(1); 206-32
15.. Djulbegovic M, and Lee AI. An update on the “novel” and direct oral anticoagulants, and long-term anticoagulant therapy: Clin Chest Med, 2018; 39(3); 583-93
16.. Albisetti M, Use of direct oral anticoagulants in children and adolescents: Hamostaseologie, 2020; 40(1); 64-73
17.. Parras Castañera E, Rodríguez López P, Álvarez A, Predictive factors for post-ercp bleeding. Influence of direct oral anticoagulants: Rev Esp Enferm Dig, 2020; 113(8); 591-96
18.. Harris S, Nadkarni NA, Naina HV, Vege SS, Splanchnic vein thrombosis in acute pancreatitis: A single-center experience: Pancreas, 2013; 42(8); 1251-54
19.. Park WS, Kim HI, Jeon BJ, Should anticoagulants be administered for portal vein thrombosis associated with acute pancreatitis?: World J Gastroenterol, 2012; 18(42); 6168-71
20.. Zhou J, Zhang H, Mao W, Efficacy and safety of early systemic anticoagulation for preventing splanchnic thrombosis in acute necrotizing pancreatitis: Pancreas, 2020; 49(9); 1220-24
21.. Hamilton JG, Needle phobia: A neglected diagnosis: J Fam Pract, 1995; 41(2); 169-75
22.. McLenon J, Rogers MA, The fear of needles: A systematic review and meta-analysis: J Adv Nurs, 2019; 75(1); 30-42
Figures
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952791

Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133