08 November 2022: Articles 
Combined Rupture of the Right Anterior Cruciate Ligament and Patellar Tendon on a 28-Year-Old Spanish Professional Handball Player Successfully Treated by Single-Stage Reconstructive Surgery
Challenging differential diagnosis, Clinical situation which can not be reproduced for ethical reasons
Francisco Selva-Sarzo1ABCDEF*, Luis Ignacio Nebot-Sanchis2ACDEFDOI: 10.12659/AJCR.937689
Am J Case Rep 2022; 23:e937689






Abstract
BACKGROUND: We present a case of combined rupture of the right anterior cruciate ligament (ACL) and patellar tendon (PT) in a 28-year-old professional handball player that was successfully treated by single-stage reconstructive surgery. The combined rupture of the ACL and PT is a rare injury pattern, and there are only a few cases reported in the literature. Presently, little evidence exists to guide management decisions for these patients. In comparison to isolated injuries, the combined rupture of the PT and ACL presents many management dilemmas.
CASE REPORT: A professional handball player from the Valencia Handball Club in the Spanish ASOBAL league had a rupture of the PT, ACL, medial collateral ligament, and medial meniscus in May 2004. A PT and ACL reconstruction was performed in a single-stage surgery. The patient returned to the sport and had no complications. He retired from professional competition after the 2016-17 season. Until follow-up in May 2021, he continued to be stable and without symptoms, remaining completely free of pain and arthrofibrosis, and the patella was centered.
CONCLUSIONS: Single-stage reconstruction of the PT and ACL in an elite-level athlete facilitated the continuation of his performance at the highest level of the sport. To the best of our knowledge, this is the only published case of a PT and ACL reconstruction in a single-stage surgical procedure that resulted in the patient making a full return to playing handball in Spain at an elite level. This case has important implications for sports medicine and sports physiotherapy.
Keywords: anterior cruciate ligament reconstruction, Bone-Patellar Tendon-Bone Grafting, Knee Injuries, Male, Humans, Adult, Anterior Cruciate Ligament, Patellar Ligament, Anterior Cruciate Ligament Injuries, Rupture
Background
The combined rupture of the anterior cruciate ligament (ACL) and the patellar tendon (PT) is a rare injury pattern, which is limited to case reports in the literature. Little evidence currently exists to guide treatment decisions for these patients [1].
Compared with isolated injuries, the combined rupture of the PT and ACL presents many management dilemmas. The timing of staged or simultaneous surgical interventions, ACL graft options, and rehabilitation restrictions are important factors which require careful consideration [1].
Owing to the limited number of case reports in the literature, there is a lack of evidence to guide the decision of whether to perform a combined reconstruction procedure or a 2-stage intervention and simultaneous repair/reconstruction. Monitoring the recovery of the patient, techniques used, and timing of when the techniques are used would help to clarify which reconstruction options are best [1].
A single-stage, simultaneous treatment of injuries due to the avulsion of the PT and ACL is possible and has been recommended by many authors [2–4], as it offers the advantage of only 1 surgical procedure and therefore a shorter rehabilitation period. After a single surgery, patients can return to their previous activity level more quickly than after 2 interventions [2,4]. If the ACL is reconstructed in the first 3 weeks after the injury occurs (inflammatory phase), the main postoperative complications reported after a single-stage treatment include low patella, arthrofibrosis, and limited knee flexion [5]. These complications can be attributed to the recommendation to limit knee flexion to between 0° and 30° during the initial recovery period [2,3,6].
One-stage combined surgery has a significantly higher complication rate than 2-stage surgery [7]. The rate of return to pre-injury activity level after surgery was not significantly different between 1-stage (88%) and 2-stage (100%) surgery. There was a significantly greater complication rate (
For the PT to recover, it is necessary to maintain the extension for 2 weeks [8], while for the ACL to recover, it is necessary to increase the flexion [9]. The law of “no pain” was maintained during rehabilitation, in addition to controlling the increase in temperature or local inflammation.
Owing to the rarity of this combined injury and the resultant impossibility of carrying out clinical trials to investigate it, the best surgical option remains unknown and there is no established protocol for the treatment of this injury [4,6,7,10–12].
Also, the specific rehabilitation protocols were not clearly reported for most of the cases included in a systematic review [7].
The main objectives of surgical intervention and subsequent physiotherapy are to restore the extensor mechanism and knee stability [2,8], recover complete articular range of motion while protecting the PT repair [3,8,13], and reproduce the original tension of the ACL in flexion so that knee kinematics are completely reestablished [9,14]. Moreover, the methodology used in this case was supported by excellent functional results and sporting performance during the patient’s 11 years of professional sporting activity after surgery.
This report presents a case of combined rupture of the right ACL and PT in a 28-year-old Spanish professional handball player that was successfully treated by single-stage reconstructive surgery.
Case Report
Informed consent was obtained in writing to access clinical information, radiology reports, and clinical and surgical photographs. Consent was given by the patient and the head of medical services at the Valencia Handball Club. The male patient was a winger who was 28 years old, 1.86 m tall, and 96 kg in weight when he ruptured the PT of his right knee while jumping to throw the ball during an ASOBAL League game in May 2004 (Video 1). He then fell to the floor, with a valgus stress applied to the right knee and internal rotation, causing the rupture of the ACL, the medial collateral ligament, and the medial meniscus. The player did not have a history of previous problems with the right knee.
Three days after the injury occurred, a partial meniscectomy of the posterior horn of the medial meniscus was performed using arthroscopic material. A T2 graft was completed using tendons from the semitendinosus and gracilis muscles for the reconstruction of the ACL and the direct suture of the PT (Figure 1), and a platelet growth factor for alveolar bone and/or soft tissue regeneration [15] was applied to the PT to accelerate healing and biological repair (Figure 2).
Moreover, a support was created using additional tissue from the semitendinosus and gracilis muscles to augment the reconstruction, and the patella was fixed using cerclage wire to protect the aforementioned repair (Figure 3). All this was done through a central-anterior prepatellar incision (Figure 1).
Once the surgery was finished, a ligament knee brace was applied in a flexion angle of 30°. It was worn in the immediate postoperative period and during the first month after surgery to enable progressive walking with the technical help of 2 crutches.
One week after the reconstruction, the patient began a protocol adapted for the rehabilitation of the ACL and PT that consisted of the application of electroanalgesia (Figure 4), cryo-therapy, passive-assisted mobilizations of the affected knee, passive mobilizations of the patella, active mobilizations of the hip and ankle of the injured lower limb, stretches and global massage of the entire musculature, and manual therapy of the healthy lower limb. The protocol was always administered without causing pain.
Once the wound had healed, mobility work was done over the scar (Figure 5) and non-weight bearing proprioception exercises in and out of a pool were added to the program (Figure 6).
Isometric exercises were done working with closed kinetic chains, exercising the core muscles, and electrostimulation was applied to the quadriceps and hamstrings, progressing gradually toward running and specific stretches, all aimed toward preparing the patient for a return to professional sport.
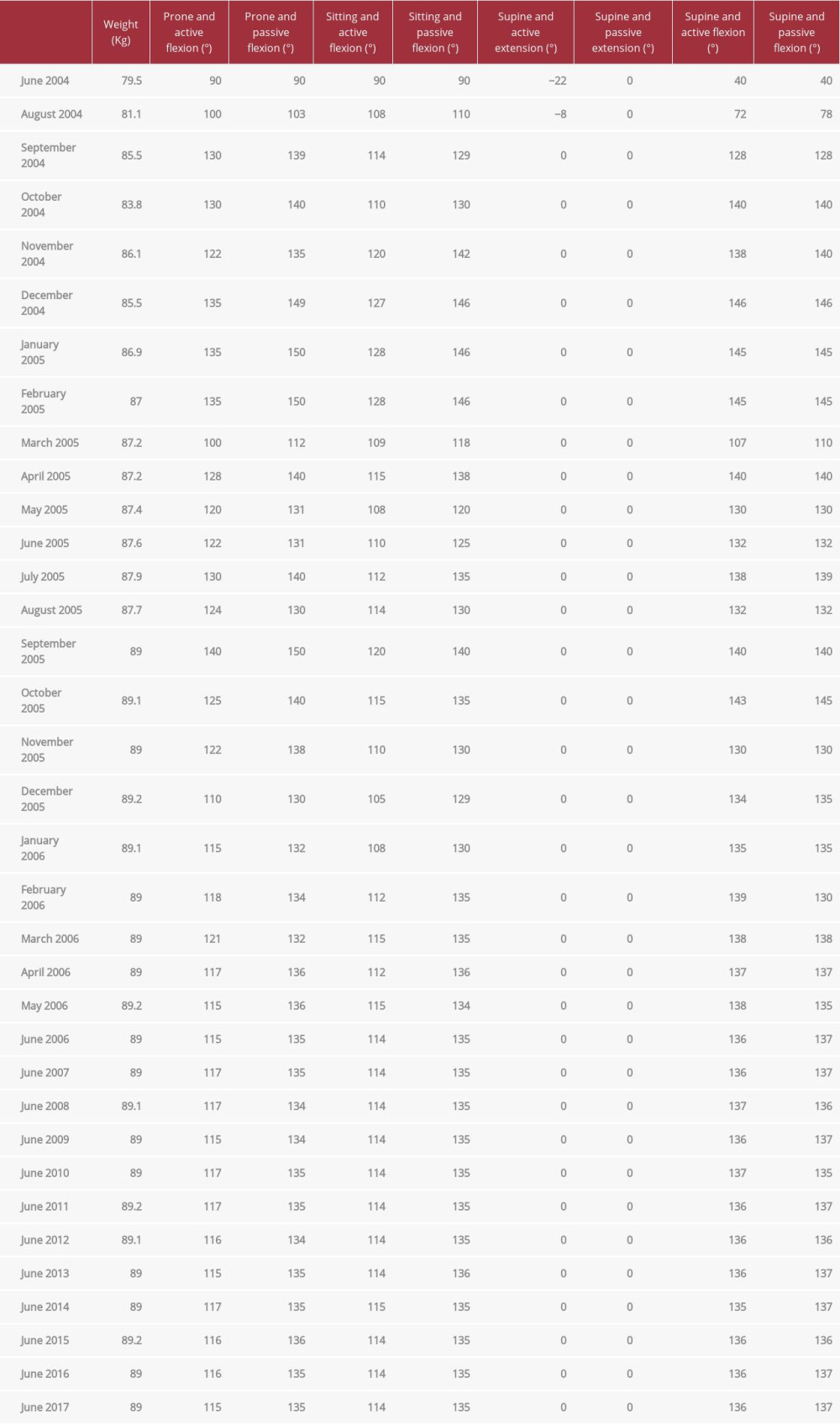
In each physiotherapy session, the increase in temperature and local inflammation were controlled. If they increased slightly, the following session involved less joint movement and the work was focused on the scar and core training. The evolution of joint mobility is shown in Table 1.
Eight months after surgery, the patient had an episode of mechanical arthritis, which forced him to reduce his physical activity, without stopping physiotherapy. He required an arthroscopy with synovectomy to resolve this complication, a procedure that was performed in the ninth month after surgery.
Thirteen months after the reconstruction surgery, the patient returned to professional handball without experiencing further complications, and his progress continued to be monitored for a total of 24 months. Table 1 shows the evolution of the patient’s active and passive mobility during this period.
Discussion
The reconstruction of both structures, the ACL and PT, in a single surgical procedure would appear to be the correct decision for professional sports players, as it reduces recovery times and allows the patients to return to competition earlier than they would after a 2-stage surgical procedure [7].
In cases of the complete rupture of the PT and ACL, surgical repair of the PT in the cases described by Kim et al [16], Gülabi et al [10], Chiang et al [14], Vega et al [17], and Costa-Paz et al [4] was performed using a primary or end-to-end suture of the PT (Krackow suture technique). In our case, the same procedure was performed on the PT, and a support was made using additional tissue from the semitendinosus and gracilis muscles (used to create the ACL graft) in the same way as in the cases described by Vega et al [17] and Gülabi et al [10]. Moreover, in our case, a platelet growth factor was applied during surgery together with the aforementioned support. The repair of the PT was reinforced using a figure-eight wire suture acting as a cerclage, as used in 4 of 21 (19.0%) of the cases described by Matthews [1]. As with our patient, 3 of the patients mentioned by Matthews required secondary surgery to extract the cerclage wire due to pain and interference with the function of the knee. In the case described by Chiang et al [14], the postoperative complication occurred in the same month as the first surgery and also required the removal of the cerclage wire.
Regarding the graft used to reconstruct the ACL, Romanini et al [18] stated that autografts are preferrable to allografts despite the fact that the first option is associated with high donor site morbidity and requires longer surgical intervention [19]. Allografts are associated with a high risk of rejection and infectious disease transmission, as well as with financial complications and/or tissue availability problems [20]. For these reasons, an autograft was used in our case, as it was by Gülabi et al [10], Chiang et al [14], Vega et al [17], and Costa-Paz et al [4].
The decision to perform the reconstruction so soon after the injury occurred was based on the fact that in elite sports the shortest possible recovery time is essential.
Moreover, repairing the PT as quickly as possible is crucial to obtain an optimal functional result [21,22]. Also, according to Kim et al [16], proceeding in this way prevents complications, such as persistent quadriceps atrophy, formation of scar tissue, and degeneration of the torn ends of the tendon, and it prevents future complications related to a prolonged period of knee instability [10,11,14,16,17].
The decision to perform a single-stage surgical intervention must consider various factors, such as the tendon graft availability, condition of the soft tissues, patient’s activity level, and experience of the surgeon [4].
Our patient was advised that the surgery was a complex intervention and the subsequent physiotherapy would be complicated because the treatment objectives for each of the injured structures were so opposed [2,13,14].
Regarding the fitting of a brace immediately after surgery, Gülabi et al [10], Chiang et al [14], Vega et al [17], and Costa-Paz et al [4] immobilized with the knee completely extended. In our case, immobilization was with a flexion angle of 30°.
Using their knowledge of the physiotherapy procedures necessary for the recovery of either the ACL [23] or PT [24] in isolation, the physiotherapist must adapt the treatment program for a patient who has undergone a simultaneous repair to both structures to deliver the greatest benefits and reduce risk as far as possible, because the structures have such opposing postoperative needs.
The specific rehabilitation protocols were not clearly reported for most of the cases included in this systematic review [7]. The conflicting rehabilitation protocols can increase the risk of complications following surgery, especially stiffness [7]. That is why joint mobility is so important and necessary. Postoperative protocols for the PT were variable, specified by each surgeon, and carried out by multiple physical therapists [25].
According to Watson et al [8], physical therapy should also include ipsilateral quadriceps strengthening; however, open-chain exercises are to be avoided for the first 4 months. Patients can return to high impact activities like running at 6 months.
In our case, we already started with a 30º flexion, reinforcing the PT with a cerclage; therefore, the gain in degrees was greater than that indicated by Watson et al [8] (Table 1).
In our patient, his knee was immobilized for a month after surgery, and the immobilization was alternated with periods of physiotherapy, which began a week after surgery and focused on the circulation and scarring of the knee, in addition to patella mobility.
One week after the reconstruction, our patient began a protocol adapted for the rehabilitation of the ACL and PT, consisting of the application of electroanalgesia and cryotherapy, passive-assisted mobilizations of the affected knee, passive mobilizations of the patella, active mobilizations of the hip and ankle of the injured lower limb, stretches and global massage of the entire musculature, and manual therapy of the healthy lower limb. The therapist always complied with the “no pain” therapy, and if the temperature increased and remained for more than 24 h or if the joint became inflamed, the workload was reduced. Once the wound had healed, further exercises were added to the protocol: non-weight-bearing proprioception exercises in and out of a pool, isometric exercises in closed kinetic chains, working the core muscles, and application of electrostimulation to the quadriceps and hamstrings, progressing gradually toward running and specific stretches (Table 1). All exercises were aimed toward preparing the patient for a return to professional sport.
The principal parameter for proper joint stability is joint mobility. The mobility gain of the knee in flexion and extension was our priority so that we could progress to working on building strength with minimal risk of injury and creating proper joint stability [2,13,14].
Six months after surgery, the stability of the knee was complete, with the patient being able to make painless changes in direction, rhythm, and speed of movement. The patient returned to training with his teammates 11 months after surgery (Table 1).
He returned to professional handball 13 months after surgery, without any relapse. Monitoring the progress of the patient’s recovery continued during the 24 months after surgery and then annually for a further 11 years.
The years after surgery did not reveal any significant clinical complications, and the patient maintained his joint mobility ranges (Table 1). No arthrofibrosis or low patella occurred, with the patella remaining in its proper position.
One limitation of this study is that, although we conducted exhaustive monitoring of the patient’s progress during the first 2 years after surgery, such close monitoring could not be continued during the subsequent 11 years of competition because the patient changed clubs; however, communication with him was maintained.
Conclusions
Single-stage reconstruction of the PT and ACL in an elite-level athlete facilitated the continuation of his performance at the highest level of sport. To the best of our knowledge, this is the only published case of a PT and ACL reconstruction in a single-stage surgical procedure that resulted in the patient making a full return to playing handball in Spain at an elite level. The case has important implications for sports medicine and sports physiotherapy.
The physiotherapist must adapt a “no pain” treatment program for a simultaneous repair of both structures, the PT and ACL, because they have such opposing postoperative needs. In our patient, we found none of the main postoperative complications, such as low patella, arthrofibrosis, and limited knee flexion, during his 13 years in competition.
Figures
References:
1.. Matthews AH, Fraser EJ, Parkinson B, Management of simultaneous patellar tendon and anterior cruciate ligament ruptures – a systematic review of available literature: J Orthop Trauma, 2018; 32(8); e320-26
2.. Shillington M, Logan M, Watts M, Myers P, A complex knee injury in a rugby league player: Inj Extra, 2008; 39(10); 327-28
3.. Koukoulias NE, Koumis P, Papadopoulos A, Acute, simultaneous tear of patellar tendon and ACL: Possible mechanism of injury and rationality of the two-stage surgical treatment: BMJ Case Rep, 2011; 2011; bcr0520114178
4.. Costa-Paz M, Muscolo DL, Makino A, Ayerza M, Simultaneous acute rupture of the patellar tendon and the anterior cruciate ligament: Arthroscopy, 2005; 21(9); 1143
5.. Wissman RD, Vonfischer N, Kempf K, Acute concomitant anterior cruciate ligament and patellar tendon tears in a non-dislocated knee: J Clin Imaging Sci, 2012; 2; 3
6.. Steiger C, Coulin B, Vendeuvre T, Distal patellar tendon avulsion associated with an ACL tear in a teenager: A case report and review of the literature: Case Rep Orthop, 2021; 2021; 6686487
7.. Meheux CJ, Jack RA, McCulloch PC, Surgical management of simultaneous anterior cruciate ligament and patellar tendon ruptures: A systematic review: J Knee Surg, 2018; 31(09); 875-83
8.. Watson SL, Kingham YE, Patel RM, Chronic quadriceps tendon ruptures: Primary repair of quadriceps via bioaugmentation and patellar tendon lengthening: Arthrosc Tech, 2022; 11(7); e1209-e17
9.. Pereira VL, Medeiros JV, Nunes GRS, Tibial-graft fixation methods on anterior cruciate ligament reconstructions: A literature review: Knee Surg Relat Res, 2021; 33(1); 7
10.. Gülabi D, Erdem M, Bulut G, Sağlam F, Neglected patellar tendon rupture with anterior cruciate ligament rupture and medial collateral ligament partial rupture: Acta Orthop Traumatol Turc, 2014; 48(2); 231-35
11.. Futch LA, Garth WP, Folsom GJ, Ogard WK, Acute rupture of the anterior cruciate ligament and patellar tendon in a collegiate athlete: Arthroscopy, 2007; 23(1); 112.e1-4
12.. Tsarouhas A, Iosifidis M, Kotzamitelos D, Traios S, Combined rupture of the patellar tendon, anterior cruciate ligament and lateral: Hippokratia, 2011; 15(2); 178-80
13.. Brunkhorst J, Johnson DL, Multiligamentous knee injury concomitant with a patellar tendon rupture: Orthopedics, 2015; 38(1); 45-48
14.. Chiang AS, Shin SS, Jazrawi LM, Rose DJ, Simultaneous ipsilateral ruptures of the anterior cruciate ligament and patellar tendon: A case report: Bull Hosp Jt Dis, 2005; 62; 134-36
15.. Tavelli L, Ravidà A, Barootchi S, Recombinant human platelet-derived growth factor: A systematic review of clinical findings in oral regenerative procedures: JDR Clin Trans Res, 2021; 6(2); 161-73
16.. Kim DH, Lee GC, Park SH, Acute simultaneous ruptures of the anterior cruciate ligament and patellar tendon: Knee Surg Relat Res, 2014; 26(1); 56-60
17.. Vega R, Huanquilef L, Íñiguez M, Rotura simultánea aguda del tendón patelar y ligamento cruzado anterior: Rev Chilena Ortop y Traum, 2006; 47; 131-34
18.. Romanini E, D’Angelo F, De Masi D, Graft selection in arthroscopic anterior cruciate ligament reconstruction: J Orthop Traumatol, 2010; 11; 211-19
19.. Halinen J, Lindahl J, Hirvensalo E, Santavirta S, Operative and nonoperative treatments of medial collateral ligament rupture with early anterior cruciate ligament reconstruction: A prospective randomized study: Am J Sport Med, 2006; 34(7); 1134-40
20.. Kiapour AM, Murray MM, Basic science of anterior cruciate ligament injury and repair: Bone Joint Res, 2014; 3; 20-31
21.. Duthon VB, Fritschy D, Knee extensor mechanism ruptures: Revue Medicale Suisse, 2011; 7(304); 1544-48
22.. Bumbaširević M, Lešić A, Acute injuries of the extensor mechanism of the knee: Curr Orthop, 2005; 19(1); 49-58
23.. Wilk KE, Macrina LC, Cain EL, Recent advances in the rehabilitation of anterior cruciate ligament injuries: J Orthop Sports Phys Ther, 2012; 42(3); 153-71
24.. West JL, Keene JS, Kaplan LD, Early motion after quadriceps and patellar tendon repairs: Outcomes with single-suture augmentation: Am J Sports Med, 2008; 36(2); 316-23
25.. O’Dowd JA, Lehoang DM, Butler RR, Operative treatment of acute patellar tendon ruptures: Am J Sports Med Sep, 2020; 48(11); 2686-91
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133